Download as pptx, pdf, or txt
You might also like
- BTKV - Cardiac - Carpentier's Reconstructive Valve SurgeryDocument363 pagesBTKV - Cardiac - Carpentier's Reconstructive Valve SurgeryDavid Christian100% (1)
- Oculomotor Nerve: DR / Hytham NafadyDocument52 pagesOculomotor Nerve: DR / Hytham NafadyGetLyricsNo ratings yet
- Oculomotor NerveDocument4 pagesOculomotor NerveHuzaifah IbrahimNo ratings yet
- Optic Nerve: Presented By: Aqsa Irfan Presented To: Dr. Sania ZehraDocument21 pagesOptic Nerve: Presented By: Aqsa Irfan Presented To: Dr. Sania ZehraAqsa100% (1)
- Anatomy of Eyelid: Presenter:-Dr. Vijayalaxmi Moderator:-Dr. SanjanaDocument49 pagesAnatomy of Eyelid: Presenter:-Dr. Vijayalaxmi Moderator:-Dr. SanjanaRidhi Bhandari100% (1)
- What Is AstigmatismDocument2 pagesWhat Is AstigmatismJA QuibzNo ratings yet
- Anatomy and Physiology of Visual PathwayDocument39 pagesAnatomy and Physiology of Visual PathwayAdarsh KeshariNo ratings yet
- Medical Neuroscience Tutorial Notes: Blood Supply To The BrainDocument6 pagesMedical Neuroscience Tutorial Notes: Blood Supply To The BrainsoyyosoloyoNo ratings yet
- Blood Supply of Cerebral CortexDocument3 pagesBlood Supply of Cerebral CortexashrafNo ratings yet
- Clinical Skills Week 1Document3 pagesClinical Skills Week 1Aishah SiddiqahNo ratings yet
- 06 Refractive ErrorDocument12 pages06 Refractive ErrorMwanja MosesNo ratings yet
- Epidural Hematoma Neuro SurgeryDocument2 pagesEpidural Hematoma Neuro SurgeryA Novita Dewi AryantiNo ratings yet
- Optic Nerve (Cranial Nerve Ii) : Abdul Wahab RasyidDocument12 pagesOptic Nerve (Cranial Nerve Ii) : Abdul Wahab RasyidWahab Rasyid100% (1)
- Anatomy of Visual Pathway, Field Defects AND Its Lesions.: By-Dr. Ruchi PherwaniDocument43 pagesAnatomy of Visual Pathway, Field Defects AND Its Lesions.: By-Dr. Ruchi Pherwanisafasayed100% (1)
- The Pupillary Light Reflex PathwayDocument5 pagesThe Pupillary Light Reflex PathwayNauli PanjaitanNo ratings yet
- Pupillary Dilatation ReflexDocument7 pagesPupillary Dilatation ReflexEden Canonizado ChengNo ratings yet
- Excitation of HeartDocument17 pagesExcitation of HeartdevdsantoshNo ratings yet
- Encephalitis Is An Acute Inflammation of The Brain. Encephalitis With Meningitis IsDocument4 pagesEncephalitis Is An Acute Inflammation of The Brain. Encephalitis With Meningitis IsDivya GuptaNo ratings yet
- 3.1 Anatomy and Physiology of The Eye - Nov. 3 - Dr. CastilloDocument13 pages3.1 Anatomy and Physiology of The Eye - Nov. 3 - Dr. CastilloHanako Sasaki AranillaNo ratings yet
- Cranial Nerve Nadz FinalDocument58 pagesCranial Nerve Nadz Finalnadzirah ruslanNo ratings yet
- AdelineDocument34 pagesAdelineEmmanuel NdukaNo ratings yet
- Pupillary Pathways &reactions: Assistant Professor, Department of Ophthalmology Nepalgunj Medical CollegeDocument16 pagesPupillary Pathways &reactions: Assistant Professor, Department of Ophthalmology Nepalgunj Medical CollegeDrBikram ThapaNo ratings yet
- Anatomy of RetinaDocument39 pagesAnatomy of Retinadr_dev100% (1)
- Retina: Zarieh Dawn L. Novela Medicine 2Document50 pagesRetina: Zarieh Dawn L. Novela Medicine 2Zari NovelaNo ratings yet
- Oculomotor Nerve: Arista Prima NDocument7 pagesOculomotor Nerve: Arista Prima NArista Prima N100% (1)
- Diseases of The Optic Nerve 09Document25 pagesDiseases of The Optic Nerve 09somebody_maNo ratings yet
- TF00001028 (Autosaved)Document10 pagesTF00001028 (Autosaved)Cid MusaNo ratings yet
- Neurology: by Dennis Jason Alcantara, RN, USRN, MAN CanDocument213 pagesNeurology: by Dennis Jason Alcantara, RN, USRN, MAN CanKristel-Mia Dimalanta RamosNo ratings yet
- Anatomy of The Uvea: Ruth Antolin, MD Doh Eye CenterDocument75 pagesAnatomy of The Uvea: Ruth Antolin, MD Doh Eye CenterRuth AntolinNo ratings yet
- PBL Modul Blindness KLP 14Document25 pagesPBL Modul Blindness KLP 14033010969No ratings yet
- Auditory SystemDocument2 pagesAuditory SystemLyron GuemoNo ratings yet
- Optic Disc EvaluationDocument45 pagesOptic Disc EvaluationAnurag SrivastavaNo ratings yet
- Pupillary Reflexes: Rohith. A Roll No-66Document34 pagesPupillary Reflexes: Rohith. A Roll No-66Karthikeyan100% (1)
- The Swinging Flashlight Test: Learning Objective: Facts About The PupilDocument3 pagesThe Swinging Flashlight Test: Learning Objective: Facts About The Pupilsiti hazard aldinaNo ratings yet
- Visual SystemDocument37 pagesVisual Systemmalinda100% (1)
- Pupillary PathwayDocument21 pagesPupillary PathwaySurbhi Bharti100% (1)
- NystagmusDocument37 pagesNystagmusMalik AllahbachayaNo ratings yet
- Anatomy Pupillary Pathways AND Abnormal Pupils: Dr. Ravula Hasika M.S.Ophthalmology (1 YR)Document100 pagesAnatomy Pupillary Pathways AND Abnormal Pupils: Dr. Ravula Hasika M.S.Ophthalmology (1 YR)Sonia Afika Aziza100% (1)
- Traktus UveaDocument90 pagesTraktus UveaAudrey Ira Yunita100% (1)
- Cornea-Anatomy and PhysiologyDocument10 pagesCornea-Anatomy and PhysiologyMido KimoNo ratings yet
- Visual ND Pupillary PathwayDocument43 pagesVisual ND Pupillary PathwayAdarsh KeshariNo ratings yet
- Colour Vision AnomaliesDocument27 pagesColour Vision AnomaliesGershon Hayford100% (1)
- Head and Spinal Cord Injury (Ci)Document111 pagesHead and Spinal Cord Injury (Ci)azmerawNo ratings yet
- Dr. Azza ZakiDocument53 pagesDr. Azza ZakiVandana Ravi100% (1)
- Development of EyeDocument21 pagesDevelopment of Eyeklauss starNo ratings yet
- Automated RefractionDocument5 pagesAutomated RefractionCarpetali GatitaNo ratings yet
- Motor TractDocument4 pagesMotor TractRaden Achmad Candra PutraNo ratings yet
- WSD Brochure Update1Document8 pagesWSD Brochure Update1Fabianto SantosoNo ratings yet
- Optic NeuritisDocument32 pagesOptic NeuritisNajaf Ali Khan100% (1)
- LR Vor VSRDocument53 pagesLR Vor VSRAlfira UlfaNo ratings yet
- Physiology of VisionDocument12 pagesPhysiology of VisionAlexis Bondad100% (2)
- Visual PathwayDocument39 pagesVisual Pathwayhuman anatomyNo ratings yet
- Anatomy and Physiology of Optic Nerve.: Dr. Sumit Pandey, MD Lecturer, COMSDocument61 pagesAnatomy and Physiology of Optic Nerve.: Dr. Sumit Pandey, MD Lecturer, COMSNaman Mishra100% (1)
- Vision Photoreceptor MechanismDocument29 pagesVision Photoreceptor MechanismTanishq Hitesh GuptaNo ratings yet
- Anatomy of UveaDocument46 pagesAnatomy of UveaSukhman kaur ButtarNo ratings yet
- Week 4 - Development of The EyeDocument5 pagesWeek 4 - Development of The EyeAleia GoNo ratings yet
- Nystagmus HDocument6 pagesNystagmus HReza AkbarNo ratings yet
- EmbryologyDocument28 pagesEmbryologyKamleshwari RenganathanNo ratings yet
- Review of Anatomy of The EarDocument16 pagesReview of Anatomy of The EarSahrish IqbalNo ratings yet
- Hey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsFrom EverandHey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsNo ratings yet
- Cranial NervesDocument61 pagesCranial NervesGuo YageNo ratings yet
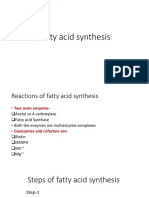
- Fatty Acid Synthesis 11.12.19Document18 pagesFatty Acid Synthesis 11.12.19Sanreet Randhawa100% (1)
- Lipid ChemistryDocument93 pagesLipid ChemistrySanreet RandhawaNo ratings yet
- Lipid - Digestion and AbsorptionDocument26 pagesLipid - Digestion and AbsorptionSanreet Randhawa100% (2)
- EnzymesDocument95 pagesEnzymesSanreet RandhawaNo ratings yet
- Anatomy 3.0: Anatomical EmbryologicalDocument49 pagesAnatomy 3.0: Anatomical EmbryologicalShenali SilvaNo ratings yet
- Diagnosa Gagal NafasDocument34 pagesDiagnosa Gagal NafasFariz Auliadi KhalilNo ratings yet
- Cardiovascular Module2Document27 pagesCardiovascular Module2Gracia MayaNo ratings yet
- Jaundice: Signs and SymptomsDocument6 pagesJaundice: Signs and Symptomshero111983No ratings yet
- 1 PredDocument7 pages1 PredandreaNo ratings yet
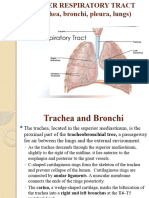
- Lower Resp TractDocument32 pagesLower Resp TractTakshikaNo ratings yet
- Clinical ExaminationsDocument1,596 pagesClinical ExaminationsmdasNo ratings yet
- Pulp LectureDocument71 pagesPulp LectureMohamad TallNo ratings yet
- MCH Urology Dissertation TopicsDocument7 pagesMCH Urology Dissertation TopicsBuyAPaperOnlineBaltimore100% (1)
- Obat NefrotoksikDocument5 pagesObat NefrotoksikIndah Nur LathifahNo ratings yet
- Congenital Heart Diseases: Non Cyanotic PlethoraDocument43 pagesCongenital Heart Diseases: Non Cyanotic PlethoraFauzi SatriaNo ratings yet
- C2 ExamDocument29 pagesC2 ExamauNo ratings yet
- What Is EcgDocument5 pagesWhat Is EcgLeeyan MeeNo ratings yet
- Transport of Substances in Humans (LQ)Document13 pagesTransport of Substances in Humans (LQ)Wan Ching ChanNo ratings yet
- PDF Quick Reference Guide To Pediatric Care 2Nd Edition Deepak M Kamat Ebook Full ChapterDocument53 pagesPDF Quick Reference Guide To Pediatric Care 2Nd Edition Deepak M Kamat Ebook Full Chapterlarry.bagwell682100% (3)
- Gastrointestinal DisordersDocument4 pagesGastrointestinal DisordersJerica Mae VenoyaNo ratings yet
- CVS ExamDocument35 pagesCVS Examtravis efraimNo ratings yet
- MCQ - Cardiovasuclar SystemDocument3 pagesMCQ - Cardiovasuclar SystemAmacus NirvanaNo ratings yet
- LABORATORY EXERCISE The Gastrointestinal System With Accessory GlandDocument5 pagesLABORATORY EXERCISE The Gastrointestinal System With Accessory GlandGelo AlonzoNo ratings yet
- Deep Vein Thrombosis Oet Reading Task SampleDocument6 pagesDeep Vein Thrombosis Oet Reading Task SampleKrischen CaiseNo ratings yet
- Buerger Allen Exercise To Improve Peripheral Vascular CirculationDocument4 pagesBuerger Allen Exercise To Improve Peripheral Vascular CirculationArun KumarNo ratings yet
- NatokinaseDocument6 pagesNatokinasefabadioNo ratings yet
- Hypertension in Geriatrics 2010Document51 pagesHypertension in Geriatrics 2010Andre HawkNo ratings yet
- Sledai-2K: Data Collection Sheet: Total ScoreDocument1 pageSledai-2K: Data Collection Sheet: Total ScoreSuryadi Limardi0% (1)
- Quality of Life of Patients Who Have Undergone Percutaneous Transluminal Coronary Angioplasty (PTCA) and Coronary Artery Bypass Graft (CABG) in A Selected Hospital, KottayamDocument3 pagesQuality of Life of Patients Who Have Undergone Percutaneous Transluminal Coronary Angioplasty (PTCA) and Coronary Artery Bypass Graft (CABG) in A Selected Hospital, KottayamInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- DVT NotesDocument3 pagesDVT NotesTodd EvansNo ratings yet
- Pericardial Effusion and Cardiac TamponadeDocument18 pagesPericardial Effusion and Cardiac TamponadeSiti Hamidah Abd Aziz100% (1)
- Head To Toe Checklist (Masroni)Document13 pagesHead To Toe Checklist (Masroni)hillary elsaNo ratings yet
- Chap22 PDFDocument9 pagesChap22 PDFSam CryshnaNo ratings yet