Download as pptx, pdf, or txt
You might also like
- Sabiston Biliary System NotesDocument5 pagesSabiston Biliary System NotessvidrillionNo ratings yet
- Basic Emergency Skills in Trauma Part 3 - Penetrating Abdoninal Injury - Dr. Oliver BelarmaDocument3 pagesBasic Emergency Skills in Trauma Part 3 - Penetrating Abdoninal Injury - Dr. Oliver BelarmaRaquel ReyesNo ratings yet
- Current Trends in Management of CholedocholithiasisDocument35 pagesCurrent Trends in Management of Choledocholithiasisrajan kumar100% (6)
- Conservative Management of Perforated Peptic UlcerDocument4 pagesConservative Management of Perforated Peptic UlcerAfiani JannahNo ratings yet
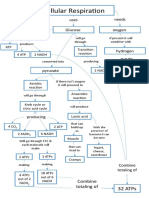
- Cellular Respiration Concept MapDocument1 pageCellular Respiration Concept MapmawakizakiNo ratings yet
- Heroes Unlimited Fillable Character Sheet by Madmanmike-D7khjl0 PDFDocument1 pageHeroes Unlimited Fillable Character Sheet by Madmanmike-D7khjl0 PDFspeedy_petey100% (1)
- (DERMA) 03 TineasDocument9 pages(DERMA) 03 TineasJolaine ValloNo ratings yet
- 7 Abdominal TraumaDocument9 pages7 Abdominal TraumaMyrtle Yvonne RagubNo ratings yet
- 4.2 Abdominal Wall Hernia (Jerome Villacorta's Conflicted Copy 2014-03-22)Document7 pages4.2 Abdominal Wall Hernia (Jerome Villacorta's Conflicted Copy 2014-03-22)Miguel C. DolotNo ratings yet
- Surgery 1.1 Fluid and Electrolyte Balance - Azares PDFDocument7 pagesSurgery 1.1 Fluid and Electrolyte Balance - Azares PDFAceking MarquezNo ratings yet
- Incisional Hernia RepairDocument6 pagesIncisional Hernia RepairLouis FortunatoNo ratings yet
- (Surg 3A) Spleen and Friends-Dr. Segismundo, Dr. Broqueza (Aisle Paler, Joseph Tolentino)Document15 pages(Surg 3A) Spleen and Friends-Dr. Segismundo, Dr. Broqueza (Aisle Paler, Joseph Tolentino)Aria Jean MostajoNo ratings yet
- Abdominal Trauma: Fatin Amirah KamaruddinDocument29 pagesAbdominal Trauma: Fatin Amirah Kamaruddinvirz23No ratings yet
- Topical Hemostatic Agents in Surgery PDFDocument10 pagesTopical Hemostatic Agents in Surgery PDFFernanda SouzaNo ratings yet
- Breast Schwartz TransDocument7 pagesBreast Schwartz TransBea MarizNo ratings yet
- Bile Duct InjuryDocument62 pagesBile Duct InjuryShashidhara Puttaraj100% (1)
- Atlas of Gastrointestinal Endoscopy and Related PathologyDocument2 pagesAtlas of Gastrointestinal Endoscopy and Related PathologyMaria PatituNo ratings yet
- Surgical Oncology and Breast BiopsyDocument12 pagesSurgical Oncology and Breast Biopsybo gum parkNo ratings yet
- BURNS - Surgery Trans2Document9 pagesBURNS - Surgery Trans2JAMPTNo ratings yet
- The Spleen - A Surgical Perspective: by Col. Abrar Hussain ZaidiDocument43 pagesThe Spleen - A Surgical Perspective: by Col. Abrar Hussain Zaidiabrar_zaidiNo ratings yet
- In Service Exam For Breast DR Paul BalisiDocument11 pagesIn Service Exam For Breast DR Paul BalisiAmiel Francisco ReyesNo ratings yet
- Colorectal Cancer 1Document71 pagesColorectal Cancer 1Anupam SisodiaNo ratings yet
- Abdominal Trauma: Dr. Sri Indah Aruminingsih, SP - RadDocument135 pagesAbdominal Trauma: Dr. Sri Indah Aruminingsih, SP - RadwidyastutiNo ratings yet
- Prosthetic Material in Inguinal Hernia RepairDocument23 pagesProsthetic Material in Inguinal Hernia RepairAnca NicaNo ratings yet
- (Basic Surg A) Immunology and TransplantationDocument7 pages(Basic Surg A) Immunology and TransplantationAimie DagaleaNo ratings yet
- An Updated Review of Cystic Hepatic LesionsDocument8 pagesAn Updated Review of Cystic Hepatic LesionsMayerlin CalvacheNo ratings yet
- Postcholecystectomy SyndromeDocument27 pagesPostcholecystectomy SyndromeMonica TurnerNo ratings yet
- Approach To Patients With Abdominal Pain-ValenDocument49 pagesApproach To Patients With Abdominal Pain-ValenCitra Sucipta0% (1)
- PRETEST SURGERY - TRAUMA QUESTION 2 - Dr. Mariana UngurDocument1 pagePRETEST SURGERY - TRAUMA QUESTION 2 - Dr. Mariana UngurMariana UngurNo ratings yet
- Dr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza HospitalDocument83 pagesDr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza Hospitalpt.mahmoudNo ratings yet
- Colorectal Ca (CRC) .: Malueth Abraham, MBCHB ViDocument36 pagesColorectal Ca (CRC) .: Malueth Abraham, MBCHB ViMalueth AnguiNo ratings yet
- Surgery QuestionsDocument19 pagesSurgery QuestionsdocaliNo ratings yet
- Blunt Adominal TraumaDocument14 pagesBlunt Adominal TraumaMuhammad Bima AkbarNo ratings yet
- (HLMN 5-19) Evaluation of The Adult With Abdominal Pain - UpToDateDocument21 pages(HLMN 5-19) Evaluation of The Adult With Abdominal Pain - UpToDateandylumanNo ratings yet
- Placement and Management of Thoracostomy Tubes - UpToDateDocument24 pagesPlacement and Management of Thoracostomy Tubes - UpToDateAndres Felipe Cuspoca OrduzNo ratings yet
- Surgery II - Pancreas 2014Document20 pagesSurgery II - Pancreas 2014Medisina101No ratings yet
- Management of Anastomotic Complications of Colorectal SurgeryDocument13 pagesManagement of Anastomotic Complications of Colorectal Surgerydadupipa100% (1)
- Penetrating Abdominal TraumaDocument3 pagesPenetrating Abdominal TraumaamrulNo ratings yet
- Clinical Surgery in General RCS Course ManualDocument2 pagesClinical Surgery in General RCS Course ManualsafiNo ratings yet
- Laparoscopic SurgeryDocument10 pagesLaparoscopic Surgerynainacurthberrt50% (2)
- Nir Hus Absite Review Q10Document11 pagesNir Hus Absite Review Q10nir4846No ratings yet
- Spindle Cell LesionsDocument8 pagesSpindle Cell LesionsdrmanishsharmaNo ratings yet
- Endoscopic SurgeryDocument152 pagesEndoscopic SurgeryiciNo ratings yet
- Breast CancerDocument4 pagesBreast CancerMaikka IlaganNo ratings yet
- 5B Surgery 1st-2nd SE #28-32 #17-18Document3 pages5B Surgery 1st-2nd SE #28-32 #17-18Liza SoberkaayoNo ratings yet
- Absite CH 32 BilliaryDocument14 pagesAbsite CH 32 BilliaryJames JosephNo ratings yet
- Acute Limb IschemiaDocument16 pagesAcute Limb IschemiaMohammad Husni BanisalmanNo ratings yet
- Phyllodes Tumors of The Breast UpToDateDocument22 pagesPhyllodes Tumors of The Breast UpToDateSean SialanaNo ratings yet
- Bowel AnastomosisDocument30 pagesBowel AnastomosismrashaiedehNo ratings yet
- 5 General Principles in TraumaDocument10 pages5 General Principles in TraumaMyrtle Yvonne RagubNo ratings yet
- Updates in Management of Enterocutaneous FistulaDocument35 pagesUpdates in Management of Enterocutaneous Fistulabashiru100% (1)
- Schwartz's Principles of Surgery 11th EditionDocument13 pagesSchwartz's Principles of Surgery 11th EditionKobe Brian Franco PeterosNo ratings yet
- A Disease Study On: AppendectomyDocument8 pagesA Disease Study On: Appendectomybryan leguiabNo ratings yet
- The Surgical Anatomy of The Nerve Laryngeal RecurrensDocument2 pagesThe Surgical Anatomy of The Nerve Laryngeal RecurrensvaNo ratings yet
- PRINCIPLES OF SURGERY (James R. Hupp Chapter 3 Notes) : 1. Develop A Surgical DiagnosisDocument5 pagesPRINCIPLES OF SURGERY (James R. Hupp Chapter 3 Notes) : 1. Develop A Surgical DiagnosisSonia LeeNo ratings yet
- ABC AbdomenDocument57 pagesABC AbdomenSyahmi KhalidNo ratings yet
- Intra Abdominal Crush InjuryDocument44 pagesIntra Abdominal Crush InjuryJustine JimenezNo ratings yet
- Biliary InjuryDocument9 pagesBiliary InjurySINAN SHAWKATNo ratings yet
- Management of Acute Pancreatitis - UpToDateDocument33 pagesManagement of Acute Pancreatitis - UpToDateCesar Luna RamirezNo ratings yet
- Diabetic Foot Ulcers Prevention & ManagementDocument59 pagesDiabetic Foot Ulcers Prevention & Managementcharity kalinowsky100% (2)
- Gangrenous Sigmoid Volvulus - A Case Report With Review of LiteratureDocument4 pagesGangrenous Sigmoid Volvulus - A Case Report With Review of LiteratureInternational Organization of Scientific Research (IOSR)No ratings yet
- Power Shuttle, Valve Assembly With PtoDocument3 pagesPower Shuttle, Valve Assembly With PtoRetropartes AcevedoNo ratings yet
- GamesDocument6 pagesGamesCarlos Vicente E. Torralba0% (1)
- Link Belt HC 268Document8 pagesLink Belt HC 268juan ochoaNo ratings yet
- Modul 7 Ali, Susi, UmaDocument11 pagesModul 7 Ali, Susi, UmaAli MustaqimNo ratings yet
- Reasoning: Data Arrangement-2Document7 pagesReasoning: Data Arrangement-2Ujjwal KumarNo ratings yet
- The Most Important Rules of FootballDocument4 pagesThe Most Important Rules of FootballJusara SaltarinNo ratings yet
- Powerade EnduranceDocument6 pagesPowerade EndurancecarlosalarconrNo ratings yet
- TaɪɡəDocument14 pagesTaɪɡəPaulina Cardinale0% (1)
- The Business of Tennis Clothes Has Grown in The Past Few YearsDocument3 pagesThe Business of Tennis Clothes Has Grown in The Past Few YearsArdias PurboyonoNo ratings yet
- List of Teen FilmsDocument21 pagesList of Teen FilmsDonaldFeanor ParrotNo ratings yet
- Gmail - Dharmshala Dalhousie Tour PackageDocument5 pagesGmail - Dharmshala Dalhousie Tour PackageJack JiNo ratings yet
- 3E - Living Greyhawk - COR2-04 - Birthday BashDocument26 pages3E - Living Greyhawk - COR2-04 - Birthday BashdebiannetNo ratings yet
- 2 - Q4 ScienceDocument16 pages2 - Q4 Sciencemaximo meridaNo ratings yet
- Dimitri Bertsekas and John N Tsitsiklis - Introduction To ProbabilityDocument6 pagesDimitri Bertsekas and John N Tsitsiklis - Introduction To ProbabilityKAUSHIKNo ratings yet
- Myferrari - Purosangue - S0rbunzDocument10 pagesMyferrari - Purosangue - S0rbunzGreggs ShopukNo ratings yet
- August Test F2Document11 pagesAugust Test F2meiphengchanNo ratings yet
- Evil Dead Rise - Google Search PDFDocument1 pageEvil Dead Rise - Google Search PDFSahilNo ratings yet
- Individual Assignment Hasrizal - Bolshoy Ice DomeDocument3 pagesIndividual Assignment Hasrizal - Bolshoy Ice Domehasrizal razaliNo ratings yet
- Gaming LanguageDocument9 pagesGaming LanguageNedelcu Lăcrămioara LarisaNo ratings yet
- PANAMA COC For Naval PersonnelDocument3 pagesPANAMA COC For Naval PersonnelPayasam Abhilash100% (1)
- 1Document121 pages1CarlosBecerraNo ratings yet
- 2010 Ford New Fiesta 1.6 Duratec SDocument16 pages2010 Ford New Fiesta 1.6 Duratec Seswar6280100% (1)
- 5am Morning Ritual PDFDocument25 pages5am Morning Ritual PDFSri Dharan100% (5)
- Squash Courts Specifications PDFDocument21 pagesSquash Courts Specifications PDFNurul Izzaty HayesNo ratings yet
- Central Problems: Paradox of Half GuardDocument19 pagesCentral Problems: Paradox of Half GuardTamerNo ratings yet
- Pokemon Fusion GeneratorDocument1 pagePokemon Fusion GeneratorFrost MourneNo ratings yet
- Toyota LC HZJ78 02 CL ClutchDocument4 pagesToyota LC HZJ78 02 CL Clutchyannis.spinnerNo ratings yet
- EE265 Worksheet 10Document5 pagesEE265 Worksheet 10dddNo ratings yet