Download as pptx, pdf, or txt
You might also like
- N4465 Assignment Weeks 1 - 3 Template-5 - 19Document22 pagesN4465 Assignment Weeks 1 - 3 Template-5 - 19horsewhisper920% (1)
- Health Illness and Medicine in CanadaDocument9 pagesHealth Illness and Medicine in CanadaSony SubediNo ratings yet
- Excitotoxins The Taste That KillsDocument324 pagesExcitotoxins The Taste That Killsvladaems100% (2)
- Case Study - PneumoniaDocument14 pagesCase Study - Pneumonianeil garcia89% (36)
- Pathophysiology of Alzheimer DiseaseDocument2 pagesPathophysiology of Alzheimer DiseaseTrixia Almendral100% (1)
- Hematology CruzDocument97 pagesHematology CruzSarah EugenioNo ratings yet
- Clinical Chemistry - PITUITARY HORMONES TRANSDocument7 pagesClinical Chemistry - PITUITARY HORMONES TRANSCamella Beatrice Lujan ValleNo ratings yet
- Lymphoid NeoplasmsDocument7 pagesLymphoid NeoplasmsMaribel SchullNo ratings yet
- Automation in Clinical ChemistryDocument28 pagesAutomation in Clinical ChemistryJoyce VitalNo ratings yet
- Merged Must KnowDocument297 pagesMerged Must KnowRegine VelascoNo ratings yet
- Hematology 1 NotesDocument40 pagesHematology 1 NotesAyessa SheinleeNo ratings yet
- Laboratory 9 Digestive SystemDocument8 pagesLaboratory 9 Digestive SystemClyde Alec (Clydealec)No ratings yet
- Cerebrospinal Fluid) AnalysisDocument20 pagesCerebrospinal Fluid) AnalysisRosemary ShirimaNo ratings yet
- HematologyDocument37 pagesHematologykurt Allen MacarilayNo ratings yet
- Hemacytometer Activity Revised 7-23-13Document6 pagesHemacytometer Activity Revised 7-23-13Jaelani AlchotriNo ratings yet
- Blood and Blood ComponentsDocument51 pagesBlood and Blood ComponentsJeevitha VanithaNo ratings yet
- MLS 422 Diagnostic MicrobiologyDocument50 pagesMLS 422 Diagnostic MicrobiologyMayowa OgunmolaNo ratings yet
- Staining & CytopathologyDocument12 pagesStaining & CytopathologyStephanie Kate Arriola100% (1)
- IlovemymomDocument149 pagesIlovemymomREYSYMAE CABRALNo ratings yet
- Hema2 Lec Lab 1Document48 pagesHema2 Lec Lab 1Yo Issei HyodonoNo ratings yet
- 2.2 Bacterial Cell Structure and FunctionDocument26 pages2.2 Bacterial Cell Structure and FunctionDhouby PianoNo ratings yet
- Staphylococcus Streptococcus: Propertie S Morpholo Gy Culture & Biochemi Cal ReactionsDocument3 pagesStaphylococcus Streptococcus: Propertie S Morpholo Gy Culture & Biochemi Cal ReactionsmadhuNo ratings yet
- BloodDocument8 pagesBloodnn nnNo ratings yet
- MABB Presentation 5 24 2022Document39 pagesMABB Presentation 5 24 2022Ayman MehassebNo ratings yet
- Chapter 17 Cytology SpecimensDocument2 pagesChapter 17 Cytology SpecimensHalidah Rahawarin100% (1)
- Draft Micro NotesDocument2 pagesDraft Micro NotesIAN GABRIELLE MERCADO CUYNONo ratings yet
- Molecular Diagnosis in HaematologyDocument23 pagesMolecular Diagnosis in HaematologyUmar'Farouq Oni100% (1)
- Virus ClassificationDocument5 pagesVirus ClassificationNUR AIN NADHIRAH SHAMSUL BADRINo ratings yet
- MUST To KNOW in Clinical ChemistryDocument54 pagesMUST To KNOW in Clinical ChemistryDuke Harvey TenchavezNo ratings yet
- Clinical Chemistry 2: Shift Unit 2: EnzymologyDocument54 pagesClinical Chemistry 2: Shift Unit 2: EnzymologyDericNo ratings yet
- Neisse RiaDocument49 pagesNeisse RiaSubhada GosaviNo ratings yet
- MUST To KNOW in HistopathologyDocument34 pagesMUST To KNOW in HistopathologyDuke Harvey TenchavezNo ratings yet
- Clinical ChemistryDocument24 pagesClinical ChemistryQueency Dangilan100% (1)
- Immunohematology and Blood BankingDocument9 pagesImmunohematology and Blood BankingMark Daniel LerioNo ratings yet
- My CologyDocument3 pagesMy CologyAbdul Samad NoonariNo ratings yet
- Automation in Clinical ChemistryDocument2 pagesAutomation in Clinical ChemistrySEBASTIEN ZOE RODRIGUEZNo ratings yet
- Analysis of Urine and Other Body FluidsDocument9 pagesAnalysis of Urine and Other Body FluidsPajarillaga Franz Erick QuintoNo ratings yet
- Enterobacteriaceace Part 1Document48 pagesEnterobacteriaceace Part 1Krenz CatiboNo ratings yet
- Lesson 3 His LabDocument35 pagesLesson 3 His LabCookie MonsterNo ratings yet
- Chapter 22Document13 pagesChapter 22Ivy Jan OcateNo ratings yet
- Antimicrobial Agents: Prof. Khaled H. Abu-ElteenDocument133 pagesAntimicrobial Agents: Prof. Khaled H. Abu-ElteenMing GamonganNo ratings yet
- Hematology ReviewerDocument12 pagesHematology ReviewerPatty RomeroNo ratings yet
- Here, Only 1 Few Stages Undergo Subdivision (Sabi Ni Maam)Document6 pagesHere, Only 1 Few Stages Undergo Subdivision (Sabi Ni Maam)Jaenie Grace AliganNo ratings yet
- Osteoid Osteoma and Osteoblastoma: Review ArticleDocument12 pagesOsteoid Osteoma and Osteoblastoma: Review ArticleAnggi MartaNo ratings yet
- Bloodandcoagulation 171230045036Document85 pagesBloodandcoagulation 171230045036Parmarkeval PravnibhaiNo ratings yet
- 33-Hemostasis and Coagulation ProfileDocument40 pages33-Hemostasis and Coagulation ProfileOsman Mohamed MuhumedNo ratings yet
- AUBF LAB WEEK 4 Chemical Examination of UrineDocument2 pagesAUBF LAB WEEK 4 Chemical Examination of UrineAndrei Tumarong AngoluanNo ratings yet
- Enterobacteriaceae Handout (Lec & Lab)Document15 pagesEnterobacteriaceae Handout (Lec & Lab)Lucille MarieNo ratings yet
- AutoverificationDocument5 pagesAutoverificationRuny RunyNo ratings yet
- Mod 1Document26 pagesMod 1SEAN MELNOR LOSBAÑESNo ratings yet
- Booklet Blood Culture 2018Document19 pagesBooklet Blood Culture 2018Karmass JallalNo ratings yet
- 5 - Must To Know Clinical MicrosDocument44 pages5 - Must To Know Clinical MicrosRudolph Jr. TaubNo ratings yet
- Blood Loss: Acute Chronic Inadequate Production of Normal Blood CellsDocument11 pagesBlood Loss: Acute Chronic Inadequate Production of Normal Blood CellsSheila Amor BodegasNo ratings yet
- 5 - Microscopic Examination of UrineDocument19 pages5 - Microscopic Examination of UrineKunware TropaNo ratings yet
- Anaerobes: Gram Positive CocciDocument4 pagesAnaerobes: Gram Positive CocciCindy Mae Flores UtlegNo ratings yet
- Digital Pathology and Artificial Intelligence As The Next Chapter in Diagnostic HematopathologyDocument7 pagesDigital Pathology and Artificial Intelligence As The Next Chapter in Diagnostic HematopathologyKira Cao0% (1)
- InjuryDocument12 pagesInjurynxdNo ratings yet
- Enterobius VermicularisDocument17 pagesEnterobius Vermicularisvels schoolg12No ratings yet
- Gram Negative HandoutDocument1 pageGram Negative HandoutAnna CrisNo ratings yet
- Carbohydrates Trace Elements VitaminsDocument31 pagesCarbohydrates Trace Elements VitaminsSophia Gail ChingNo ratings yet
- 1 SEMR421 Bacteriology Part 1Document10 pages1 SEMR421 Bacteriology Part 1Micah Daniel TapiaNo ratings yet
- 6.1 AE 1 MP (Questionnaire) PDFDocument44 pages6.1 AE 1 MP (Questionnaire) PDFMae AnnNo ratings yet
- Aubf Lec Reviewer MidtermDocument129 pagesAubf Lec Reviewer MidtermTrangia, SharmaineNo ratings yet
- The Diagnostic Use of ADVIA 2120i Siemens and An "APL Criteria" CanDocument9 pagesThe Diagnostic Use of ADVIA 2120i Siemens and An "APL Criteria" CananggaririnNo ratings yet
- Analysis of Urine and Other Body Fluids - , RMT Sputum & Bronchoalveolar Lavage (Bal)Document11 pagesAnalysis of Urine and Other Body Fluids - , RMT Sputum & Bronchoalveolar Lavage (Bal)jeffreyNo ratings yet
- INCOME TAXATION (Performance Task)Document2 pagesINCOME TAXATION (Performance Task)Stephany PolinarNo ratings yet
- PD 2146 EjDocument2 pagesPD 2146 EjStephany PolinarNo ratings yet
- Tax RatesDocument6 pagesTax RatesStephany PolinarNo ratings yet
- REM LAW AnnotationDocument18 pagesREM LAW AnnotationStephany PolinarNo ratings yet
- Criminal LawDocument81 pagesCriminal LawStephany PolinarNo ratings yet
- Kagaw Notes 100Document33 pagesKagaw Notes 100Stephany PolinarNo ratings yet
- QuotesDocument2 pagesQuotesStephany PolinarNo ratings yet
- Level of Stress ASPALALS GROUP Edited VerDocument67 pagesLevel of Stress ASPALALS GROUP Edited VerStephany PolinarNo ratings yet
- How To Evaluate FSDocument8 pagesHow To Evaluate FSStephany PolinarNo ratings yet
- Data (Ana Mae)Document6 pagesData (Ana Mae)Stephany PolinarNo ratings yet
- Data Gathering (AutoRecovered)Document24 pagesData Gathering (AutoRecovered)Stephany PolinarNo ratings yet
- Civil Law Persons and Family RelationsDocument63 pagesCivil Law Persons and Family RelationsStephany Polinar100% (1)
- 114 115Document2 pages114 115Stephany PolinarNo ratings yet
- Updated Ej Foh-Wip-Job Order Cost SystemDocument29 pagesUpdated Ej Foh-Wip-Job Order Cost SystemStephany PolinarNo ratings yet
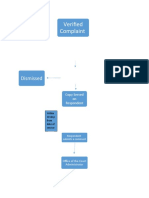
- Verified Complaint: DismissedDocument4 pagesVerified Complaint: DismissedStephany PolinarNo ratings yet
- Labor LawDocument45 pagesLabor LawStephany PolinarNo ratings yet
- OBLICONDocument24 pagesOBLICONStephany PolinarNo ratings yet
- Final Examination: Criminal Law ReviewDocument18 pagesFinal Examination: Criminal Law ReviewStephany PolinarNo ratings yet
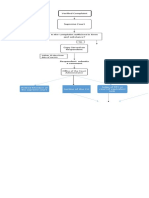
- Is The Complaint Sufficient in Form and Substance?Document2 pagesIs The Complaint Sufficient in Form and Substance?Stephany PolinarNo ratings yet
- TRUST RECEIPTS LAW NOTES by SAPDocument5 pagesTRUST RECEIPTS LAW NOTES by SAPStephany PolinarNo ratings yet
- Agency CollatedDocument36 pagesAgency CollatedStephany PolinarNo ratings yet
- Civil Law Partnership Agency TrustsDocument47 pagesCivil Law Partnership Agency TrustsStephany Polinar100% (1)
- Polinar LCS PDFDocument3 pagesPolinar LCS PDFStephany PolinarNo ratings yet
- Regional Trial Court: People of The PhilippinesDocument2 pagesRegional Trial Court: People of The PhilippinesStephany PolinarNo ratings yet
- 1 BIR - TRAIN - Briefing - Introduction To TRAINDocument23 pages1 BIR - TRAIN - Briefing - Introduction To TRAINStephany PolinarNo ratings yet
- Republic of The Philippines Department of Justice Office of The City Prosecutor City of ZamboangaDocument2 pagesRepublic of The Philippines Department of Justice Office of The City Prosecutor City of ZamboangaStephany PolinarNo ratings yet
- Manual de Operacion BBC 16Document184 pagesManual de Operacion BBC 16Yeison RamirezNo ratings yet
- What Is The Topic About?Document2 pagesWhat Is The Topic About?SHER-A JANNARALNo ratings yet
- EXPRESS Trial 2008Document10 pagesEXPRESS Trial 2008Dr. Sergio Oscar AlunniNo ratings yet
- Lupus Thesis StatementDocument7 pagesLupus Thesis Statementaprilwatsonlittlerock100% (2)
- Epilepsy 70Document24 pagesEpilepsy 70g. aimolaNo ratings yet
- Lesson 4Document21 pagesLesson 4hk_scribdNo ratings yet
- Cta Poster PresentationDocument1 pageCta Poster PresentationsreejithNo ratings yet
- Foreigner Physical Examination FormDocument2 pagesForeigner Physical Examination Formxreinx932No ratings yet
- Elizabeth Malin EDLD 5315 Literature ReviewDocument24 pagesElizabeth Malin EDLD 5315 Literature ReviewebbyfuentesNo ratings yet
- Anastasiia CooperDocument49 pagesAnastasiia CooperAnastasiia CooperNo ratings yet
- Whole Body DonationDocument4 pagesWhole Body DonationWhitneyWrichNo ratings yet
- Anomalous Pulmonary Venous Drainage: A Pictorial Essay With A CT FocusDocument13 pagesAnomalous Pulmonary Venous Drainage: A Pictorial Essay With A CT FocusIchel Silva FndzNo ratings yet
- ISMT12 - Day 169 - Sheila - Spinal MeningitisDocument14 pagesISMT12 - Day 169 - Sheila - Spinal Meningitisbosnia agusNo ratings yet
- PLOS Manuscript Body Formatting GuidelinesDocument4 pagesPLOS Manuscript Body Formatting GuidelinesNicolás Lozano SuárezNo ratings yet
- Session 5 Presentation Cleaning DisinfectionDocument22 pagesSession 5 Presentation Cleaning DisinfectionPrincess Anne ChavezNo ratings yet
- Bioram DengueDocument46 pagesBioram DengueDIAGNOSTICO MOLECULAR LESP COLIMANo ratings yet
- Cardiology OSCEsDocument85 pagesCardiology OSCEsMed StudentNo ratings yet
- HealthallergyDocument11 pagesHealthallergyMary Rose QuimanjanNo ratings yet
- SW EotE - Critical InjuryDocument1 pageSW EotE - Critical InjuryNatália Capelari100% (1)
- Prosthetics and OrthoticsDocument53 pagesProsthetics and OrthoticsAkbar AziziNo ratings yet
- EhrDocument4 pagesEhrapi-608465780No ratings yet
- Techniques and Guidelines For Social Work Practice, 7/EDocument71 pagesTechniques and Guidelines For Social Work Practice, 7/EAnanta ChaliseNo ratings yet
- "Neuro Rehabilitation": Presented byDocument52 pages"Neuro Rehabilitation": Presented byArchana VermaNo ratings yet
- Unit 17 Assignment Brief 2Document3 pagesUnit 17 Assignment Brief 2fatii.seedNo ratings yet
- IATF Resolution No. 90Document3 pagesIATF Resolution No. 90Steph GNo ratings yet