
Back To Basics - Urology - Dr. James Watterson 2009 - Compressed
Back To Basics - Urology - Dr. James Watterson 2009 - Compressed
You might also like
- 1 s2.0 S1936878X23000335 Main PDFDocument6 pages1 s2.0 S1936878X23000335 Main PDFrindayusticiaNo ratings yet
- Biology Investigatory ProjectDocument61 pagesBiology Investigatory ProjectJIYA NAIR66% (61)
- PALS Study GuideDocument25 pagesPALS Study GuideVitor Hugo G CorreiaNo ratings yet
- Fast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeFrom EverandFast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeNo ratings yet
- Pharma ExamDocument5 pagesPharma ExamMclavin LoveNo ratings yet
- HematuriaDocument15 pagesHematurianisaw_2No ratings yet
- Hematuria: Ikobho A. DDocument28 pagesHematuria: Ikobho A. DPrincewill SeiyefaNo ratings yet
- MS, Frcs (England), Frcs (Edinburgh), Frcs (Glasgow)Document52 pagesMS, Frcs (England), Frcs (Edinburgh), Frcs (Glasgow)Anis HospitalNo ratings yet
- Eva Bolton Haematuria Presentation WebDocument52 pagesEva Bolton Haematuria Presentation WebereczkieNo ratings yet
- Guidelines For UrologyDocument91 pagesGuidelines For UrologyAruna HarikrishnanNo ratings yet
- Microhematuria Case Study: Medical Student Case-Based LearningDocument30 pagesMicrohematuria Case Study: Medical Student Case-Based LearningjenegneNo ratings yet
- Cystic Diseases of The Kidney. Renal NeoplasmsDocument31 pagesCystic Diseases of The Kidney. Renal NeoplasmsFate ChanNo ratings yet
- Introduction To UrologyDocument48 pagesIntroduction To UrologyvaiyenNo ratings yet
- EAU - Bladder Stones (19!02!21)Document21 pagesEAU - Bladder Stones (19!02!21)Nhi NhiNo ratings yet
- Lecture Notes On Medical Nursing IiiDocument614 pagesLecture Notes On Medical Nursing IiiAnim Richard DuoduNo ratings yet
- Case Based Teaching - Urology: Haematuria & Renal TransplantDocument21 pagesCase Based Teaching - Urology: Haematuria & Renal Transplantamoody95No ratings yet
- Introduction Nephrology - History, Exam and InvestigationsDocument39 pagesIntroduction Nephrology - History, Exam and InvestigationsDaniel KilonzoNo ratings yet
- Benign Prostatic HyperplasiaDocument36 pagesBenign Prostatic Hyperplasiamomodou s jallowNo ratings yet
- Haematuria: Definition / Supporting InformationDocument8 pagesHaematuria: Definition / Supporting InformationdrsaleemNo ratings yet
- Brad J Hornberger Cystoscopy Indications and Preparation. UAPA CME Conference 2012 (30 Min)Document36 pagesBrad J Hornberger Cystoscopy Indications and Preparation. UAPA CME Conference 2012 (30 Min)Cristian OrozcoNo ratings yet
- Urologic Stone Disease 2005Document51 pagesUrologic Stone Disease 2005jamilNo ratings yet
- NMSC Gross HematuriaDocument41 pagesNMSC Gross HematuriaStoned PickleNo ratings yet
- HematuriaDocument1 pageHematuriaskf1027No ratings yet
- Congenital Urological Conditions - Dr. HawkarDocument38 pagesCongenital Urological Conditions - Dr. HawkarBashar KhalilNo ratings yet
- Approach To Patient With Renal DiseaseDocument74 pagesApproach To Patient With Renal DiseaseSaja SaqerNo ratings yet
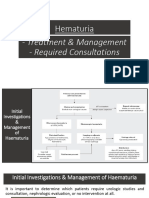
- Hematuria Treatment Management and Required ConsultationsDocument10 pagesHematuria Treatment Management and Required ConsultationsDiyana ZatyNo ratings yet
- Urinary RetentionDocument28 pagesUrinary RetentionSchoeb MuhammadNo ratings yet
- Uti Cme Ho PresentationDocument34 pagesUti Cme Ho PresentationJunaidahMubarakAliNo ratings yet
- Urinary Tract InvestigationDocument28 pagesUrinary Tract InvestigationZell 46No ratings yet
- Presentation Liver UltrasoundDocument21 pagesPresentation Liver UltrasoundDanielle FosterNo ratings yet
- Acutecholangitis 110927014348 Phpapp01Document25 pagesAcutecholangitis 110927014348 Phpapp01shintameliaNo ratings yet
- Examination of The Gastrointestinal TractDocument44 pagesExamination of The Gastrointestinal TractDrNaveen Singh Rajpurohit Kadu100% (1)
- Seminar On Tumor of Genito-Urinary SystemDocument33 pagesSeminar On Tumor of Genito-Urinary SystemLakshay AroraNo ratings yet
- Management of Malignant AscitesDocument34 pagesManagement of Malignant Ascitesadaiah Soibi-HarryNo ratings yet
- Obstructive JaundiceDocument37 pagesObstructive JaundiceDronacharya RouthNo ratings yet
- FibrothecomaDocument94 pagesFibrothecomaMindy SantiagoNo ratings yet
- Alterations in Urinary FunctionDocument35 pagesAlterations in Urinary FunctionAaLona RobinsonNo ratings yet
- Jurnal HematuriaDocument6 pagesJurnal HematuriaErlin IrawatiNo ratings yet
- Urinary Tract Infection: UpdateDocument42 pagesUrinary Tract Infection: UpdateakNo ratings yet
- HematuriaDocument86 pagesHematuriaMohamad Arif MustaphaNo ratings yet
- Renal and Urological Disorders: General ApproachDocument30 pagesRenal and Urological Disorders: General ApproachIrma HermaliaNo ratings yet
- 07 - Basics of Adrenal Urinary Tract Prostate and Testicle ImagingDocument139 pages07 - Basics of Adrenal Urinary Tract Prostate and Testicle ImagingHusam AbuodehNo ratings yet
- Introduction in UrologyDocument69 pagesIntroduction in UrologyKaram SaadNo ratings yet
- Imaging of Acute PancreatitisDocument53 pagesImaging of Acute PancreatitisLazar VučetićNo ratings yet
- DD Hematuria FixDocument12 pagesDD Hematuria FixirmaNo ratings yet
- Urinary Symptoms - DR RashaDocument70 pagesUrinary Symptoms - DR RashaRasha TelebNo ratings yet
- Obscure Gi BleedingDocument76 pagesObscure Gi Bleedingbittuhimi24No ratings yet
- Benign Prostatic Hyperplasia: DR Arun Gnyawali Resident, 1 Year Nepalgunj Medical CollegeDocument27 pagesBenign Prostatic Hyperplasia: DR Arun Gnyawali Resident, 1 Year Nepalgunj Medical CollegeHemanta PunNo ratings yet
- Surg 2 JaundicedDocument94 pagesSurg 2 Jaundicedapi-3728522No ratings yet
- OJ EditedDocument57 pagesOJ EditedrobelNo ratings yet
- Uti RukayyyahDocument40 pagesUti Rukayyyahajusdabo95No ratings yet
- URORADIOLOGYDocument34 pagesURORADIOLOGYMeg AmoonNo ratings yet
- Patho SlidesDocument46 pagesPatho Slidesapi-400411160No ratings yet
- Hepatocellular Carcinoma and Other Hepatic MassesDocument59 pagesHepatocellular Carcinoma and Other Hepatic MassesIsaac MwangiNo ratings yet
- Benign Hepatobiliary DisordersDocument29 pagesBenign Hepatobiliary DisordershafizahhoshniNo ratings yet
- Trauma, Malignancy, Congenital Abnormalities of Urogenital SystemDocument64 pagesTrauma, Malignancy, Congenital Abnormalities of Urogenital SystemDapot SianiparNo ratings yet
- Genitourinary TuberculosisDocument15 pagesGenitourinary TuberculosisMrunal Dive100% (1)
- Acute Urine RetentionDocument30 pagesAcute Urine Retentiondilekamunasinghe4No ratings yet
- Recent Management of Calculous Biliary DiseaseDocument35 pagesRecent Management of Calculous Biliary DiseaseAbhishek SarafNo ratings yet
- SURG - Hepatobiliary, Pancreas, SpleenDocument230 pagesSURG - Hepatobiliary, Pancreas, SpleenJoan Timbol100% (1)
- Faiza Hashim Soomro PG-Gen SurgeryDocument47 pagesFaiza Hashim Soomro PG-Gen SurgeryFaiza Hashim SoomroNo ratings yet
- Biliary Surgery: Presenter: DR Muhuga JR Facilitator: DR MwashambwaDocument54 pagesBiliary Surgery: Presenter: DR Muhuga JR Facilitator: DR MwashambwaSamar AhmadNo ratings yet
- Middle Age Man With Nephrotic Syndrome, Ascitis and Edema: Raika Jamali MDDocument66 pagesMiddle Age Man With Nephrotic Syndrome, Ascitis and Edema: Raika Jamali MDyusnafratilova16No ratings yet
- Hematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesFrom EverandHematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesRating: 5 out of 5 stars5/5 (2)
- New DOCX DocumentDocument12 pagesNew DOCX DocumentDr Anais AsimNo ratings yet
- The Punjab Animals Slaughter Control ActDocument20 pagesThe Punjab Animals Slaughter Control ActDr Anais AsimNo ratings yet
- Group #9Document75 pagesGroup #9Dr Anais AsimNo ratings yet
- Bovine Spongiform EncephalopathyDocument66 pagesBovine Spongiform EncephalopathyDr Anais AsimNo ratings yet
- MedicineDocument82 pagesMedicineDr Anais AsimNo ratings yet
- Biosecruity GrowerDocument15 pagesBiosecruity GrowerDr Anais AsimNo ratings yet
- Milking ParlorsDocument5 pagesMilking ParlorsDr Anais AsimNo ratings yet
- Blue Tongue by NabeelDocument115 pagesBlue Tongue by NabeelDr Anais AsimNo ratings yet
- Foot Mouth DiseaseDocument73 pagesFoot Mouth DiseaseDr Anais AsimNo ratings yet
- Affection of EarDocument43 pagesAffection of EarDr Anais AsimNo ratings yet
- SurgeyDocument37 pagesSurgeyDr Anais AsimNo ratings yet
- Affections of HoofDocument48 pagesAffections of HoofDr Anais AsimNo ratings yet
- General AnesthesiaDocument22 pagesGeneral AnesthesiaDr Anais AsimNo ratings yet
- MedicineDocument6 pagesMedicineDr Anais AsimNo ratings yet
- Corrected Feasibility Report For 40 Dairy Cattles in BahIawalpur Region ...Document4 pagesCorrected Feasibility Report For 40 Dairy Cattles in BahIawalpur Region ...Dr Anais AsimNo ratings yet
- Exosomes 8thDocument5 pagesExosomes 8thDr Anais AsimNo ratings yet
- Cystotomy 37 LDocument19 pagesCystotomy 37 LDr Anais AsimNo ratings yet
- Milk Collection Systems in PakistanDocument24 pagesMilk Collection Systems in PakistanDr Anais AsimNo ratings yet
- AssignmentDocument9 pagesAssignmentDr Anais AsimNo ratings yet
- Circulatory Disturbances 2014Document102 pagesCirculatory Disturbances 2014Dr Anais AsimNo ratings yet
- Acts by Raza HameedDocument25 pagesActs by Raza HameedDr Anais AsimNo ratings yet
- CestodesDocument6 pagesCestodesDr Anais AsimNo ratings yet
- Different Forms and Designs of Feed MillDocument66 pagesDifferent Forms and Designs of Feed MillDr Anais AsimNo ratings yet
- AncyclostomaDocument3 pagesAncyclostomaDr Anais AsimNo ratings yet
- 21 Animal Nutrition and FeedsDocument59 pages21 Animal Nutrition and FeedsDr Anais AsimNo ratings yet
- 20 Dairy Feed Management Final For Karachi 28march08Document71 pages20 Dairy Feed Management Final For Karachi 28march08Dr Anais AsimNo ratings yet
- Diroflaria ImmitisDocument15 pagesDiroflaria ImmitisDr Anais AsimNo ratings yet
- Urea NPN SourcesDocument60 pagesUrea NPN SourcesDr Anais AsimNo ratings yet
- Feed Raw Material Handling and StorageDocument57 pagesFeed Raw Material Handling and StorageDr Anais AsimNo ratings yet
- StrongloidesDocument2 pagesStrongloidesDr Anais AsimNo ratings yet
- Biomedical Signals and Sensors II - Linking Acoustic and Optic Biosignals and Biomedical Sensors (PDFDrive)Document233 pagesBiomedical Signals and Sensors II - Linking Acoustic and Optic Biosignals and Biomedical Sensors (PDFDrive)QSilvaNo ratings yet
- Pediatric Cardiology Thesis TopicsDocument4 pagesPediatric Cardiology Thesis Topicspzblktgld100% (2)
- Koding ICDDocument15 pagesKoding ICDriandy putraNo ratings yet
- The Circulatory System ReviewerDocument4 pagesThe Circulatory System ReviewerKaten KyoukotsuNo ratings yet
- MS Wrep IIDocument51 pagesMS Wrep IIiana-almocera-6970No ratings yet
- 260-Article Text-875-1-10-20220728Document4 pages260-Article Text-875-1-10-20220728hasan andrianNo ratings yet
- Ebook Tintinallis Emergency Medicine Manual PDF Full Chapter PDFDocument67 pagesEbook Tintinallis Emergency Medicine Manual PDF Full Chapter PDFsusan.fulton134100% (38)
- Smoking and DiabetesDocument5 pagesSmoking and DiabetesgiannidietNo ratings yet
- Comparison of The Haemodynamic Effects and Seizure Activity During Modified ECT With Thiopentone and Propofol Used As Inducing AgentsDocument15 pagesComparison of The Haemodynamic Effects and Seizure Activity During Modified ECT With Thiopentone and Propofol Used As Inducing AgentsIOSR Journal of PharmacyNo ratings yet
- Nclex Cardio QuestionsDocument4 pagesNclex Cardio QuestionsMichelleNo ratings yet
- PendingWorklist - 2023 02 07 - 2023 02 09Document31 pagesPendingWorklist - 2023 02 07 - 2023 02 09Neil JostenNo ratings yet
- Chest Wall, Lung, MediastinumDocument124 pagesChest Wall, Lung, MediastinumKenn BrillanteNo ratings yet
- Biological Science Class 11 SyllabusDocument10 pagesBiological Science Class 11 SyllabusSwapnil Das HCS - 46No ratings yet
- New Born Assess PPT FrankDocument118 pagesNew Born Assess PPT FrankPooja HardiyaNo ratings yet
- PrometricDocument34 pagesPrometricsundus youssefNo ratings yet
- Syncope 3Document19 pagesSyncope 3Pratyush PrateekNo ratings yet
- Pharmacology Bundle 20221 2 PDFDocument42 pagesPharmacology Bundle 20221 2 PDFسلطان محمد فوزي سلمانNo ratings yet
- Forehead Flap: DR Dipti Patil (1 MDS) Dept of Oral Maxillofacial Surgery KCDS, BangloreDocument42 pagesForehead Flap: DR Dipti Patil (1 MDS) Dept of Oral Maxillofacial Surgery KCDS, BangloreDipti PatilNo ratings yet
- Neuraxial Anesthesia in Patient With ScoliosisDocument5 pagesNeuraxial Anesthesia in Patient With ScoliosisIndra T Budianto0% (1)
- What Is Acanthosis Nigricans?: DarkeningDocument2 pagesWhat Is Acanthosis Nigricans?: DarkeningIulianaNo ratings yet
- CTEPH - JACC 2020 - FocusDocument15 pagesCTEPH - JACC 2020 - FocusDaniela PekeNo ratings yet
- Dr. K. Subramanian Consultant Neurosurgeon Anuradha Clinic & Sooriya HospitalDocument22 pagesDr. K. Subramanian Consultant Neurosurgeon Anuradha Clinic & Sooriya HospitalDheerajJonnalagaddaNo ratings yet
- TMX428 TMX58 Service Manual EnglishDocument159 pagesTMX428 TMX58 Service Manual Englishedgar corroNo ratings yet
- NCP (Coronary Artery Disease) - PacateDocument7 pagesNCP (Coronary Artery Disease) - PacateKristile Ann PacateNo ratings yet
- Cardiac Oral Presentations - Program-Escvs 2017 PDFDocument32 pagesCardiac Oral Presentations - Program-Escvs 2017 PDFGhenadie BostanNo ratings yet
- Congestive Heart Failure ReportDocument6 pagesCongestive Heart Failure ReportSunshine_Bacla_4275100% (1)






















































































































Download as ppt, pdf, or txt
You might also like
- 1 s2.0 S1936878X23000335 Main PDFDocument6 pages1 s2.0 S1936878X23000335 Main PDFrindayusticiaNo ratings yet
- Biology Investigatory ProjectDocument61 pagesBiology Investigatory ProjectJIYA NAIR66% (61)
- PALS Study GuideDocument25 pagesPALS Study GuideVitor Hugo G CorreiaNo ratings yet
- Fast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeFrom EverandFast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeNo ratings yet
- Pharma ExamDocument5 pagesPharma ExamMclavin LoveNo ratings yet
- HematuriaDocument15 pagesHematurianisaw_2No ratings yet
- Hematuria: Ikobho A. DDocument28 pagesHematuria: Ikobho A. DPrincewill SeiyefaNo ratings yet
- MS, Frcs (England), Frcs (Edinburgh), Frcs (Glasgow)Document52 pagesMS, Frcs (England), Frcs (Edinburgh), Frcs (Glasgow)Anis HospitalNo ratings yet
- Eva Bolton Haematuria Presentation WebDocument52 pagesEva Bolton Haematuria Presentation WebereczkieNo ratings yet
- Guidelines For UrologyDocument91 pagesGuidelines For UrologyAruna HarikrishnanNo ratings yet
- Microhematuria Case Study: Medical Student Case-Based LearningDocument30 pagesMicrohematuria Case Study: Medical Student Case-Based LearningjenegneNo ratings yet
- Cystic Diseases of The Kidney. Renal NeoplasmsDocument31 pagesCystic Diseases of The Kidney. Renal NeoplasmsFate ChanNo ratings yet
- Introduction To UrologyDocument48 pagesIntroduction To UrologyvaiyenNo ratings yet
- EAU - Bladder Stones (19!02!21)Document21 pagesEAU - Bladder Stones (19!02!21)Nhi NhiNo ratings yet
- Lecture Notes On Medical Nursing IiiDocument614 pagesLecture Notes On Medical Nursing IiiAnim Richard DuoduNo ratings yet
- Case Based Teaching - Urology: Haematuria & Renal TransplantDocument21 pagesCase Based Teaching - Urology: Haematuria & Renal Transplantamoody95No ratings yet
- Introduction Nephrology - History, Exam and InvestigationsDocument39 pagesIntroduction Nephrology - History, Exam and InvestigationsDaniel KilonzoNo ratings yet
- Benign Prostatic HyperplasiaDocument36 pagesBenign Prostatic Hyperplasiamomodou s jallowNo ratings yet
- Haematuria: Definition / Supporting InformationDocument8 pagesHaematuria: Definition / Supporting InformationdrsaleemNo ratings yet
- Brad J Hornberger Cystoscopy Indications and Preparation. UAPA CME Conference 2012 (30 Min)Document36 pagesBrad J Hornberger Cystoscopy Indications and Preparation. UAPA CME Conference 2012 (30 Min)Cristian OrozcoNo ratings yet
- Urologic Stone Disease 2005Document51 pagesUrologic Stone Disease 2005jamilNo ratings yet
- NMSC Gross HematuriaDocument41 pagesNMSC Gross HematuriaStoned PickleNo ratings yet
- HematuriaDocument1 pageHematuriaskf1027No ratings yet
- Congenital Urological Conditions - Dr. HawkarDocument38 pagesCongenital Urological Conditions - Dr. HawkarBashar KhalilNo ratings yet
- Approach To Patient With Renal DiseaseDocument74 pagesApproach To Patient With Renal DiseaseSaja SaqerNo ratings yet
- Hematuria Treatment Management and Required ConsultationsDocument10 pagesHematuria Treatment Management and Required ConsultationsDiyana ZatyNo ratings yet
- Urinary RetentionDocument28 pagesUrinary RetentionSchoeb MuhammadNo ratings yet
- Uti Cme Ho PresentationDocument34 pagesUti Cme Ho PresentationJunaidahMubarakAliNo ratings yet
- Urinary Tract InvestigationDocument28 pagesUrinary Tract InvestigationZell 46No ratings yet
- Presentation Liver UltrasoundDocument21 pagesPresentation Liver UltrasoundDanielle FosterNo ratings yet
- Acutecholangitis 110927014348 Phpapp01Document25 pagesAcutecholangitis 110927014348 Phpapp01shintameliaNo ratings yet
- Examination of The Gastrointestinal TractDocument44 pagesExamination of The Gastrointestinal TractDrNaveen Singh Rajpurohit Kadu100% (1)
- Seminar On Tumor of Genito-Urinary SystemDocument33 pagesSeminar On Tumor of Genito-Urinary SystemLakshay AroraNo ratings yet
- Management of Malignant AscitesDocument34 pagesManagement of Malignant Ascitesadaiah Soibi-HarryNo ratings yet
- Obstructive JaundiceDocument37 pagesObstructive JaundiceDronacharya RouthNo ratings yet
- FibrothecomaDocument94 pagesFibrothecomaMindy SantiagoNo ratings yet
- Alterations in Urinary FunctionDocument35 pagesAlterations in Urinary FunctionAaLona RobinsonNo ratings yet
- Jurnal HematuriaDocument6 pagesJurnal HematuriaErlin IrawatiNo ratings yet
- Urinary Tract Infection: UpdateDocument42 pagesUrinary Tract Infection: UpdateakNo ratings yet
- HematuriaDocument86 pagesHematuriaMohamad Arif MustaphaNo ratings yet
- Renal and Urological Disorders: General ApproachDocument30 pagesRenal and Urological Disorders: General ApproachIrma HermaliaNo ratings yet
- 07 - Basics of Adrenal Urinary Tract Prostate and Testicle ImagingDocument139 pages07 - Basics of Adrenal Urinary Tract Prostate and Testicle ImagingHusam AbuodehNo ratings yet
- Introduction in UrologyDocument69 pagesIntroduction in UrologyKaram SaadNo ratings yet
- Imaging of Acute PancreatitisDocument53 pagesImaging of Acute PancreatitisLazar VučetićNo ratings yet
- DD Hematuria FixDocument12 pagesDD Hematuria FixirmaNo ratings yet
- Urinary Symptoms - DR RashaDocument70 pagesUrinary Symptoms - DR RashaRasha TelebNo ratings yet
- Obscure Gi BleedingDocument76 pagesObscure Gi Bleedingbittuhimi24No ratings yet
- Benign Prostatic Hyperplasia: DR Arun Gnyawali Resident, 1 Year Nepalgunj Medical CollegeDocument27 pagesBenign Prostatic Hyperplasia: DR Arun Gnyawali Resident, 1 Year Nepalgunj Medical CollegeHemanta PunNo ratings yet
- Surg 2 JaundicedDocument94 pagesSurg 2 Jaundicedapi-3728522No ratings yet
- OJ EditedDocument57 pagesOJ EditedrobelNo ratings yet
- Uti RukayyyahDocument40 pagesUti Rukayyyahajusdabo95No ratings yet
- URORADIOLOGYDocument34 pagesURORADIOLOGYMeg AmoonNo ratings yet
- Patho SlidesDocument46 pagesPatho Slidesapi-400411160No ratings yet
- Hepatocellular Carcinoma and Other Hepatic MassesDocument59 pagesHepatocellular Carcinoma and Other Hepatic MassesIsaac MwangiNo ratings yet
- Benign Hepatobiliary DisordersDocument29 pagesBenign Hepatobiliary DisordershafizahhoshniNo ratings yet
- Trauma, Malignancy, Congenital Abnormalities of Urogenital SystemDocument64 pagesTrauma, Malignancy, Congenital Abnormalities of Urogenital SystemDapot SianiparNo ratings yet
- Genitourinary TuberculosisDocument15 pagesGenitourinary TuberculosisMrunal Dive100% (1)
- Acute Urine RetentionDocument30 pagesAcute Urine Retentiondilekamunasinghe4No ratings yet
- Recent Management of Calculous Biliary DiseaseDocument35 pagesRecent Management of Calculous Biliary DiseaseAbhishek SarafNo ratings yet
- SURG - Hepatobiliary, Pancreas, SpleenDocument230 pagesSURG - Hepatobiliary, Pancreas, SpleenJoan Timbol100% (1)
- Faiza Hashim Soomro PG-Gen SurgeryDocument47 pagesFaiza Hashim Soomro PG-Gen SurgeryFaiza Hashim SoomroNo ratings yet
- Biliary Surgery: Presenter: DR Muhuga JR Facilitator: DR MwashambwaDocument54 pagesBiliary Surgery: Presenter: DR Muhuga JR Facilitator: DR MwashambwaSamar AhmadNo ratings yet
- Middle Age Man With Nephrotic Syndrome, Ascitis and Edema: Raika Jamali MDDocument66 pagesMiddle Age Man With Nephrotic Syndrome, Ascitis and Edema: Raika Jamali MDyusnafratilova16No ratings yet
- Hematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesFrom EverandHematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesRating: 5 out of 5 stars5/5 (2)
- New DOCX DocumentDocument12 pagesNew DOCX DocumentDr Anais AsimNo ratings yet
- The Punjab Animals Slaughter Control ActDocument20 pagesThe Punjab Animals Slaughter Control ActDr Anais AsimNo ratings yet
- Group #9Document75 pagesGroup #9Dr Anais AsimNo ratings yet
- Bovine Spongiform EncephalopathyDocument66 pagesBovine Spongiform EncephalopathyDr Anais AsimNo ratings yet
- MedicineDocument82 pagesMedicineDr Anais AsimNo ratings yet
- Biosecruity GrowerDocument15 pagesBiosecruity GrowerDr Anais AsimNo ratings yet
- Milking ParlorsDocument5 pagesMilking ParlorsDr Anais AsimNo ratings yet
- Blue Tongue by NabeelDocument115 pagesBlue Tongue by NabeelDr Anais AsimNo ratings yet
- Foot Mouth DiseaseDocument73 pagesFoot Mouth DiseaseDr Anais AsimNo ratings yet
- Affection of EarDocument43 pagesAffection of EarDr Anais AsimNo ratings yet
- SurgeyDocument37 pagesSurgeyDr Anais AsimNo ratings yet
- Affections of HoofDocument48 pagesAffections of HoofDr Anais AsimNo ratings yet
- General AnesthesiaDocument22 pagesGeneral AnesthesiaDr Anais AsimNo ratings yet
- MedicineDocument6 pagesMedicineDr Anais AsimNo ratings yet
- Corrected Feasibility Report For 40 Dairy Cattles in BahIawalpur Region ...Document4 pagesCorrected Feasibility Report For 40 Dairy Cattles in BahIawalpur Region ...Dr Anais AsimNo ratings yet
- Exosomes 8thDocument5 pagesExosomes 8thDr Anais AsimNo ratings yet
- Cystotomy 37 LDocument19 pagesCystotomy 37 LDr Anais AsimNo ratings yet
- Milk Collection Systems in PakistanDocument24 pagesMilk Collection Systems in PakistanDr Anais AsimNo ratings yet
- AssignmentDocument9 pagesAssignmentDr Anais AsimNo ratings yet
- Circulatory Disturbances 2014Document102 pagesCirculatory Disturbances 2014Dr Anais AsimNo ratings yet
- Acts by Raza HameedDocument25 pagesActs by Raza HameedDr Anais AsimNo ratings yet
- CestodesDocument6 pagesCestodesDr Anais AsimNo ratings yet
- Different Forms and Designs of Feed MillDocument66 pagesDifferent Forms and Designs of Feed MillDr Anais AsimNo ratings yet
- AncyclostomaDocument3 pagesAncyclostomaDr Anais AsimNo ratings yet
- 21 Animal Nutrition and FeedsDocument59 pages21 Animal Nutrition and FeedsDr Anais AsimNo ratings yet
- 20 Dairy Feed Management Final For Karachi 28march08Document71 pages20 Dairy Feed Management Final For Karachi 28march08Dr Anais AsimNo ratings yet
- Diroflaria ImmitisDocument15 pagesDiroflaria ImmitisDr Anais AsimNo ratings yet
- Urea NPN SourcesDocument60 pagesUrea NPN SourcesDr Anais AsimNo ratings yet
- Feed Raw Material Handling and StorageDocument57 pagesFeed Raw Material Handling and StorageDr Anais AsimNo ratings yet
- StrongloidesDocument2 pagesStrongloidesDr Anais AsimNo ratings yet
- Biomedical Signals and Sensors II - Linking Acoustic and Optic Biosignals and Biomedical Sensors (PDFDrive)Document233 pagesBiomedical Signals and Sensors II - Linking Acoustic and Optic Biosignals and Biomedical Sensors (PDFDrive)QSilvaNo ratings yet
- Pediatric Cardiology Thesis TopicsDocument4 pagesPediatric Cardiology Thesis Topicspzblktgld100% (2)
- Koding ICDDocument15 pagesKoding ICDriandy putraNo ratings yet
- The Circulatory System ReviewerDocument4 pagesThe Circulatory System ReviewerKaten KyoukotsuNo ratings yet
- MS Wrep IIDocument51 pagesMS Wrep IIiana-almocera-6970No ratings yet
- 260-Article Text-875-1-10-20220728Document4 pages260-Article Text-875-1-10-20220728hasan andrianNo ratings yet
- Ebook Tintinallis Emergency Medicine Manual PDF Full Chapter PDFDocument67 pagesEbook Tintinallis Emergency Medicine Manual PDF Full Chapter PDFsusan.fulton134100% (38)
- Smoking and DiabetesDocument5 pagesSmoking and DiabetesgiannidietNo ratings yet
- Comparison of The Haemodynamic Effects and Seizure Activity During Modified ECT With Thiopentone and Propofol Used As Inducing AgentsDocument15 pagesComparison of The Haemodynamic Effects and Seizure Activity During Modified ECT With Thiopentone and Propofol Used As Inducing AgentsIOSR Journal of PharmacyNo ratings yet
- Nclex Cardio QuestionsDocument4 pagesNclex Cardio QuestionsMichelleNo ratings yet
- PendingWorklist - 2023 02 07 - 2023 02 09Document31 pagesPendingWorklist - 2023 02 07 - 2023 02 09Neil JostenNo ratings yet
- Chest Wall, Lung, MediastinumDocument124 pagesChest Wall, Lung, MediastinumKenn BrillanteNo ratings yet
- Biological Science Class 11 SyllabusDocument10 pagesBiological Science Class 11 SyllabusSwapnil Das HCS - 46No ratings yet
- New Born Assess PPT FrankDocument118 pagesNew Born Assess PPT FrankPooja HardiyaNo ratings yet
- PrometricDocument34 pagesPrometricsundus youssefNo ratings yet
- Syncope 3Document19 pagesSyncope 3Pratyush PrateekNo ratings yet
- Pharmacology Bundle 20221 2 PDFDocument42 pagesPharmacology Bundle 20221 2 PDFسلطان محمد فوزي سلمانNo ratings yet
- Forehead Flap: DR Dipti Patil (1 MDS) Dept of Oral Maxillofacial Surgery KCDS, BangloreDocument42 pagesForehead Flap: DR Dipti Patil (1 MDS) Dept of Oral Maxillofacial Surgery KCDS, BangloreDipti PatilNo ratings yet
- Neuraxial Anesthesia in Patient With ScoliosisDocument5 pagesNeuraxial Anesthesia in Patient With ScoliosisIndra T Budianto0% (1)
- What Is Acanthosis Nigricans?: DarkeningDocument2 pagesWhat Is Acanthosis Nigricans?: DarkeningIulianaNo ratings yet
- CTEPH - JACC 2020 - FocusDocument15 pagesCTEPH - JACC 2020 - FocusDaniela PekeNo ratings yet
- Dr. K. Subramanian Consultant Neurosurgeon Anuradha Clinic & Sooriya HospitalDocument22 pagesDr. K. Subramanian Consultant Neurosurgeon Anuradha Clinic & Sooriya HospitalDheerajJonnalagaddaNo ratings yet
- TMX428 TMX58 Service Manual EnglishDocument159 pagesTMX428 TMX58 Service Manual Englishedgar corroNo ratings yet
- NCP (Coronary Artery Disease) - PacateDocument7 pagesNCP (Coronary Artery Disease) - PacateKristile Ann PacateNo ratings yet
- Cardiac Oral Presentations - Program-Escvs 2017 PDFDocument32 pagesCardiac Oral Presentations - Program-Escvs 2017 PDFGhenadie BostanNo ratings yet
- Congestive Heart Failure ReportDocument6 pagesCongestive Heart Failure ReportSunshine_Bacla_4275100% (1)