
Routes of Administration
Routes of Administration
You might also like
- RCDSO Guidelines Role of OpioidsDocument16 pagesRCDSO Guidelines Role of OpioidsMonaNo ratings yet
- Practical Implications of Cytotoxic Drug AdministrDocument10 pagesPractical Implications of Cytotoxic Drug AdministrSundas EjazNo ratings yet
- Nombre Del Estudiante: CARMITA GERONIMO GARCIADocument6 pagesNombre Del Estudiante: CARMITA GERONIMO GARCIAcarmita geronimo garciaNo ratings yet
- Parenteral Drug Delivery: Clinical Pharmacy Guide: Cancer Drug Treatment Assessment and Review 5 EditionDocument9 pagesParenteral Drug Delivery: Clinical Pharmacy Guide: Cancer Drug Treatment Assessment and Review 5 EditionIssac GeorgeNo ratings yet
- Title - BT Treatment Procedure For Vaginal CarcinomaDocument21 pagesTitle - BT Treatment Procedure For Vaginal CarcinomaparvezNo ratings yet
- Interstitial High-Dose-Rate Gynecologic Brachytherapy: Clinical Workflow Experience From Three Academic InstitutionsDocument10 pagesInterstitial High-Dose-Rate Gynecologic Brachytherapy: Clinical Workflow Experience From Three Academic Institutions980Denis FernandezNo ratings yet
- Acesso Vascular EmergenciaDocument9 pagesAcesso Vascular EmergenciaSílvia TrindadeNo ratings yet
- ChemotherapyDocument7 pagesChemotherapyAlan CJNo ratings yet
- Central Venous AccessDocument20 pagesCentral Venous AccessCarlos GuerreroNo ratings yet
- Acesso Venoso TecnicaDocument16 pagesAcesso Venoso TecnicaNatascha CabralNo ratings yet
- Extravasation Guidelines 2007Document42 pagesExtravasation Guidelines 2007crahanknotNo ratings yet
- Chapter 14A Pituitary Adenomas and CraniopharyngiomasDocument8 pagesChapter 14A Pituitary Adenomas and CraniopharyngiomasMohammad Ali IsmailNo ratings yet
- Care Bundle For Insertion and Maintenance of Central Venous Catheters Within The Renal and Transplant UnitDocument14 pagesCare Bundle For Insertion and Maintenance of Central Venous Catheters Within The Renal and Transplant Unitnavjav100% (1)
- Case StudyDocument9 pagesCase StudyCheyserine MagaoayNo ratings yet
- Intravenous TherapyDocument10 pagesIntravenous TherapyS. AmberNo ratings yet
- Oncology Nursing Part 2Document25 pagesOncology Nursing Part 2Ayessa Yvonne PanganibanNo ratings yet
- Parenteral Preparation PDFDocument17 pagesParenteral Preparation PDFHely Patel100% (1)
- Surgical Bed Side ProceduressDocument62 pagesSurgical Bed Side Proceduressdrhiwaomer100% (1)
- 2009 Venous AccessDocument3 pages2009 Venous AccessDaniela MéndezNo ratings yet
- Tindakan TorakosentesisDocument15 pagesTindakan TorakosentesisAyu Ayu AyuNo ratings yet
- Extravasation of Systemic Hemato-Oncological Therapies - FullDocument5 pagesExtravasation of Systemic Hemato-Oncological Therapies - FullYosr Samia Abou Sedira100% (1)
- Management of Patient With Liver CancerDocument48 pagesManagement of Patient With Liver CancerFarah NaazNo ratings yet
- Enfermeria CateterDocument13 pagesEnfermeria CateterJaime Augusto Quimbayo GuarnizoNo ratings yet
- Anesthetic Management: Hysterectomy: in This IssueDocument8 pagesAnesthetic Management: Hysterectomy: in This IssueTerrence ClemonsNo ratings yet
- Overview of Central Venous AccessDocument13 pagesOverview of Central Venous AccessnathanaelandryNo ratings yet
- Anaesthetic Management of The Child With Haematological Malignancy - BJA Education - Oxford AcademicDocument19 pagesAnaesthetic Management of The Child With Haematological Malignancy - BJA Education - Oxford Academicpradeep danielNo ratings yet
- Welcome TO Intensive Care UnitDocument42 pagesWelcome TO Intensive Care UnitKharene Lirazan100% (1)
- Violeta 2Document10 pagesVioleta 2Georgiana StoicaNo ratings yet
- ParenteralDocument4 pagesParenteralreymar.martinez88No ratings yet
- Radical Cystectomy: History of The ProcedureDocument6 pagesRadical Cystectomy: History of The ProcedureIvy MinaNo ratings yet
- Oncology BulletsDocument11 pagesOncology BulletsDonaJeanNo ratings yet
- Kuter DJ - Thrombotic Complications of Central Venous Catheters in Cancer PatientsDocument10 pagesKuter DJ - Thrombotic Complications of Central Venous Catheters in Cancer PatientsFarid RakhmanNo ratings yet
- Cesaroetal AnnHematol2016Document11 pagesCesaroetal AnnHematol2016yanuar esthoNo ratings yet
- Bridging The IV Access Gap With Midline CathetersDocument3 pagesBridging The IV Access Gap With Midline CathetersCosmin RusneacNo ratings yet
- Rehabilitation and Treatment of Spinal Cord TumorsDocument8 pagesRehabilitation and Treatment of Spinal Cord TumorsAndreea SlabuNo ratings yet
- Abdominal Mass Removal: Hugh H. Allen, M.DDocument6 pagesAbdominal Mass Removal: Hugh H. Allen, M.DAbbyKristekNo ratings yet
- Https:emedicine Medscape Com:article:2047080-PrintDocument5 pagesHttps:emedicine Medscape Com:article:2047080-Printmiss beeNo ratings yet
- Guidelines On The Insertion and Management of CentralDocument18 pagesGuidelines On The Insertion and Management of CentralAgustina ItinNo ratings yet
- Absceso y Fistula AnalDocument24 pagesAbsceso y Fistula AnalSinue PumaNo ratings yet
- Complications of Central Venous Port Systems: A Pictorial ReviewDocument12 pagesComplications of Central Venous Port Systems: A Pictorial ReviewMANGNo ratings yet
- Peripherally Inserted Central Venous Acces - 2021 - Seminars in Pediatric SurgerDocument8 pagesPeripherally Inserted Central Venous Acces - 2021 - Seminars in Pediatric Surgeralergo.ramirezNo ratings yet
- Acute Lymphocytic Leukemia FinalDocument30 pagesAcute Lymphocytic Leukemia FinalYuwi50% (2)
- NURSING CARE OF PATIENTS RECEIVING CHEMOTHERAPY KemoterapiDocument41 pagesNURSING CARE OF PATIENTS RECEIVING CHEMOTHERAPY KemoterapiEni ListiantiNo ratings yet
- Insertion Mangement Peripheral IVCannulaDocument20 pagesInsertion Mangement Peripheral IVCannulaAadil AadilNo ratings yet
- 2022-AnorectalAbscess FistulainAno RectovaginalFistula-CPGDocument22 pages2022-AnorectalAbscess FistulainAno RectovaginalFistula-CPGEmanuella CirinoNo ratings yet
- Intravenous FluidsDocument3 pagesIntravenous FluidsKristine Artes AguilarNo ratings yet
- Breast Ultrasound For The Interventionalist: Madhavi Raghu, MD, and Regina Hooley, MDDocument7 pagesBreast Ultrasound For The Interventionalist: Madhavi Raghu, MD, and Regina Hooley, MDrasminojNo ratings yet
- Proposal Research NewDocument25 pagesProposal Research NewNndaydnaNo ratings yet
- SOGC DVT ProphylaxisDocument16 pagesSOGC DVT Prophylaxisibrahimnazeh96No ratings yet
- Roles of Bone Marrow Transplant Unit Nurses IncludesDocument10 pagesRoles of Bone Marrow Transplant Unit Nurses IncludesGleden UmayamNo ratings yet
- Types of GastrostomyDocument4 pagesTypes of GastrostomyChad AlsayNo ratings yet
- Anesthesia and Perioperative Management of Colorectal Surgical Patients - Specific Issues (Part 2)Document10 pagesAnesthesia and Perioperative Management of Colorectal Surgical Patients - Specific Issues (Part 2)Syauqi DarussalamNo ratings yet
- ChemoDocument54 pagesChemoKarren FernandezNo ratings yet
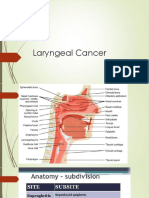
- Laryngeal Cancer 1Document49 pagesLaryngeal Cancer 1Kpj KpjNo ratings yet
- C AnnulationDocument15 pagesC AnnulationSaffronMaeNo ratings yet
- Routes of Drug AdministrationDocument4 pagesRoutes of Drug AdministrationJoeyNo ratings yet
- Picc Infection PDFDocument16 pagesPicc Infection PDFMahesh ChandraNo ratings yet
- Central Venous Access DevicesDocument6 pagesCentral Venous Access DevicesAllan MacacapagalNo ratings yet
- Endoscopy - Hysteroscopy and Laparoscopy Indications, Contraindications and ComplicationsDocument16 pagesEndoscopy - Hysteroscopy and Laparoscopy Indications, Contraindications and Complicationsselatur100% (1)
- Cancer Regional Therapy: HAI, HIPEC, HILP, ILI, PIPAC and BeyondFrom EverandCancer Regional Therapy: HAI, HIPEC, HILP, ILI, PIPAC and BeyondNo ratings yet
- Intravenous Therapy Administration: a practical guideFrom EverandIntravenous Therapy Administration: a practical guideRating: 4 out of 5 stars4/5 (1)
- Drug Development: New Chemical Entity DevelopmentDocument6 pagesDrug Development: New Chemical Entity DevelopmentDeenNo ratings yet
- Drug-Induced Hepatotoxicity - Overview, Metabolism of Drugs, Clinical and Pathological Manifestations of Drug-Induced Liver DiseaseDocument20 pagesDrug-Induced Hepatotoxicity - Overview, Metabolism of Drugs, Clinical and Pathological Manifestations of Drug-Induced Liver Diseaseal ghiffari muhammad rayhan100% (1)
- European Consensus On The Management of RDSDocument41 pagesEuropean Consensus On The Management of RDSDeddy Supriyadi100% (1)
- Pyanosid - Powder 3753 K 0317 Engl - 01Document5 pagesPyanosid - Powder 3753 K 0317 Engl - 01Ionuţ BuţurcăNo ratings yet
- End-Plate PotentialDocument7 pagesEnd-Plate PotentialSitrak OnyNo ratings yet
- Basic Pharmacology: NTA Level 4 Semester 2Document12 pagesBasic Pharmacology: NTA Level 4 Semester 2MabusiNo ratings yet
- Beginners Guide To Anabolic Steroids PDFDocument84 pagesBeginners Guide To Anabolic Steroids PDFLeo AlbertoNo ratings yet
- Clin Pharm 151 Review Test A. Multiple ChoiceDocument4 pagesClin Pharm 151 Review Test A. Multiple ChoiceAngel GoNo ratings yet
- TYRX BrochureDocument28 pagesTYRX Brochureleo chiuNo ratings yet
- B Pharm 4 Sem Pharmalite - inDocument17 pagesB Pharm 4 Sem Pharmalite - inGanga (Sandeep Pilania)No ratings yet
- Febuxostat in GoutDocument7 pagesFebuxostat in GoutLia NadaNo ratings yet
- Pharmacovigilance Responsibilities of Medicine Sponsors: Australian Recommendations and RequirementsDocument44 pagesPharmacovigilance Responsibilities of Medicine Sponsors: Australian Recommendations and RequirementsResmy JoseNo ratings yet
- Unit 3 - Cology 3Document25 pagesUnit 3 - Cology 3Shreyas ShreyuNo ratings yet
- ChromoblastomycosisDocument90 pagesChromoblastomycosisTara Sefanya KairupanNo ratings yet
- How To Cite A Record On A Clinical Trials Register: Table: Examples of Citation Format Registry Example CitationDocument1 pageHow To Cite A Record On A Clinical Trials Register: Table: Examples of Citation Format Registry Example CitationSebastiánRodríguezNo ratings yet
- Acupuncture and Cancer - David O'Regan, Jacqueine Filshie - The Royal Marsden Hospital, London and Surrey, UKDocument6 pagesAcupuncture and Cancer - David O'Regan, Jacqueine Filshie - The Royal Marsden Hospital, London and Surrey, UKFredericoNo ratings yet
- DHEA and Its Transformation Into Androgens and Estrogens in Peripheral Target Tissues: IntracrinologyDocument28 pagesDHEA and Its Transformation Into Androgens and Estrogens in Peripheral Target Tissues: IntracrinologyFernanda PérezNo ratings yet
- MBBS - General Medicine Reg Id: KMC - 142105 RX ID: 406824261Document1 pageMBBS - General Medicine Reg Id: KMC - 142105 RX ID: 406824261Dipam HalderNo ratings yet
- Zyrtec: Tablet Core: Tablet CoatingDocument5 pagesZyrtec: Tablet Core: Tablet CoatingDwi WirastomoNo ratings yet
- Sincope Vs Crisis - Lancet Neurol 2006 PDFDocument10 pagesSincope Vs Crisis - Lancet Neurol 2006 PDFLina HerreraNo ratings yet
- Prescription: DownloadDocument12 pagesPrescription: DownloadkalpanajainNo ratings yet
- Handy Chart PsychosisDocument3 pagesHandy Chart Psychosismerryavie45No ratings yet
- History of PharmacyDocument33 pagesHistory of Pharmacymalokkhan183No ratings yet
- Kontrol Anes PasienDocument4 pagesKontrol Anes Pasienzidni fatayanNo ratings yet
- CV - 5-2023Document7 pagesCV - 5-2023api-668616332No ratings yet
- CDHO Factsheet AsthmaDocument4 pagesCDHO Factsheet AsthmaIlse AnzuresNo ratings yet
- Classification of Hormones: By. Dr. Luna PhukanDocument13 pagesClassification of Hormones: By. Dr. Luna Phukanacrehell8No ratings yet
- Daftar Harga: Pt. Bernofarm Marketing IvDocument4 pagesDaftar Harga: Pt. Bernofarm Marketing IvSofyan HadiNataNo ratings yet
- Excipient-Free Pulmonary Insulin Dry PowderDocument9 pagesExcipient-Free Pulmonary Insulin Dry PowderYaninaDeLafuenteNo ratings yet
























































































Download as pptx, pdf, or txt
You might also like
- RCDSO Guidelines Role of OpioidsDocument16 pagesRCDSO Guidelines Role of OpioidsMonaNo ratings yet
- Practical Implications of Cytotoxic Drug AdministrDocument10 pagesPractical Implications of Cytotoxic Drug AdministrSundas EjazNo ratings yet
- Nombre Del Estudiante: CARMITA GERONIMO GARCIADocument6 pagesNombre Del Estudiante: CARMITA GERONIMO GARCIAcarmita geronimo garciaNo ratings yet
- Parenteral Drug Delivery: Clinical Pharmacy Guide: Cancer Drug Treatment Assessment and Review 5 EditionDocument9 pagesParenteral Drug Delivery: Clinical Pharmacy Guide: Cancer Drug Treatment Assessment and Review 5 EditionIssac GeorgeNo ratings yet
- Title - BT Treatment Procedure For Vaginal CarcinomaDocument21 pagesTitle - BT Treatment Procedure For Vaginal CarcinomaparvezNo ratings yet
- Interstitial High-Dose-Rate Gynecologic Brachytherapy: Clinical Workflow Experience From Three Academic InstitutionsDocument10 pagesInterstitial High-Dose-Rate Gynecologic Brachytherapy: Clinical Workflow Experience From Three Academic Institutions980Denis FernandezNo ratings yet
- Acesso Vascular EmergenciaDocument9 pagesAcesso Vascular EmergenciaSílvia TrindadeNo ratings yet
- ChemotherapyDocument7 pagesChemotherapyAlan CJNo ratings yet
- Central Venous AccessDocument20 pagesCentral Venous AccessCarlos GuerreroNo ratings yet
- Acesso Venoso TecnicaDocument16 pagesAcesso Venoso TecnicaNatascha CabralNo ratings yet
- Extravasation Guidelines 2007Document42 pagesExtravasation Guidelines 2007crahanknotNo ratings yet
- Chapter 14A Pituitary Adenomas and CraniopharyngiomasDocument8 pagesChapter 14A Pituitary Adenomas and CraniopharyngiomasMohammad Ali IsmailNo ratings yet
- Care Bundle For Insertion and Maintenance of Central Venous Catheters Within The Renal and Transplant UnitDocument14 pagesCare Bundle For Insertion and Maintenance of Central Venous Catheters Within The Renal and Transplant Unitnavjav100% (1)
- Case StudyDocument9 pagesCase StudyCheyserine MagaoayNo ratings yet
- Intravenous TherapyDocument10 pagesIntravenous TherapyS. AmberNo ratings yet
- Oncology Nursing Part 2Document25 pagesOncology Nursing Part 2Ayessa Yvonne PanganibanNo ratings yet
- Parenteral Preparation PDFDocument17 pagesParenteral Preparation PDFHely Patel100% (1)
- Surgical Bed Side ProceduressDocument62 pagesSurgical Bed Side Proceduressdrhiwaomer100% (1)
- 2009 Venous AccessDocument3 pages2009 Venous AccessDaniela MéndezNo ratings yet
- Tindakan TorakosentesisDocument15 pagesTindakan TorakosentesisAyu Ayu AyuNo ratings yet
- Extravasation of Systemic Hemato-Oncological Therapies - FullDocument5 pagesExtravasation of Systemic Hemato-Oncological Therapies - FullYosr Samia Abou Sedira100% (1)
- Management of Patient With Liver CancerDocument48 pagesManagement of Patient With Liver CancerFarah NaazNo ratings yet
- Enfermeria CateterDocument13 pagesEnfermeria CateterJaime Augusto Quimbayo GuarnizoNo ratings yet
- Anesthetic Management: Hysterectomy: in This IssueDocument8 pagesAnesthetic Management: Hysterectomy: in This IssueTerrence ClemonsNo ratings yet
- Overview of Central Venous AccessDocument13 pagesOverview of Central Venous AccessnathanaelandryNo ratings yet
- Anaesthetic Management of The Child With Haematological Malignancy - BJA Education - Oxford AcademicDocument19 pagesAnaesthetic Management of The Child With Haematological Malignancy - BJA Education - Oxford Academicpradeep danielNo ratings yet
- Welcome TO Intensive Care UnitDocument42 pagesWelcome TO Intensive Care UnitKharene Lirazan100% (1)
- Violeta 2Document10 pagesVioleta 2Georgiana StoicaNo ratings yet
- ParenteralDocument4 pagesParenteralreymar.martinez88No ratings yet
- Radical Cystectomy: History of The ProcedureDocument6 pagesRadical Cystectomy: History of The ProcedureIvy MinaNo ratings yet
- Oncology BulletsDocument11 pagesOncology BulletsDonaJeanNo ratings yet
- Kuter DJ - Thrombotic Complications of Central Venous Catheters in Cancer PatientsDocument10 pagesKuter DJ - Thrombotic Complications of Central Venous Catheters in Cancer PatientsFarid RakhmanNo ratings yet
- Cesaroetal AnnHematol2016Document11 pagesCesaroetal AnnHematol2016yanuar esthoNo ratings yet
- Bridging The IV Access Gap With Midline CathetersDocument3 pagesBridging The IV Access Gap With Midline CathetersCosmin RusneacNo ratings yet
- Rehabilitation and Treatment of Spinal Cord TumorsDocument8 pagesRehabilitation and Treatment of Spinal Cord TumorsAndreea SlabuNo ratings yet
- Abdominal Mass Removal: Hugh H. Allen, M.DDocument6 pagesAbdominal Mass Removal: Hugh H. Allen, M.DAbbyKristekNo ratings yet
- Https:emedicine Medscape Com:article:2047080-PrintDocument5 pagesHttps:emedicine Medscape Com:article:2047080-Printmiss beeNo ratings yet
- Guidelines On The Insertion and Management of CentralDocument18 pagesGuidelines On The Insertion and Management of CentralAgustina ItinNo ratings yet
- Absceso y Fistula AnalDocument24 pagesAbsceso y Fistula AnalSinue PumaNo ratings yet
- Complications of Central Venous Port Systems: A Pictorial ReviewDocument12 pagesComplications of Central Venous Port Systems: A Pictorial ReviewMANGNo ratings yet
- Peripherally Inserted Central Venous Acces - 2021 - Seminars in Pediatric SurgerDocument8 pagesPeripherally Inserted Central Venous Acces - 2021 - Seminars in Pediatric Surgeralergo.ramirezNo ratings yet
- Acute Lymphocytic Leukemia FinalDocument30 pagesAcute Lymphocytic Leukemia FinalYuwi50% (2)
- NURSING CARE OF PATIENTS RECEIVING CHEMOTHERAPY KemoterapiDocument41 pagesNURSING CARE OF PATIENTS RECEIVING CHEMOTHERAPY KemoterapiEni ListiantiNo ratings yet
- Insertion Mangement Peripheral IVCannulaDocument20 pagesInsertion Mangement Peripheral IVCannulaAadil AadilNo ratings yet
- 2022-AnorectalAbscess FistulainAno RectovaginalFistula-CPGDocument22 pages2022-AnorectalAbscess FistulainAno RectovaginalFistula-CPGEmanuella CirinoNo ratings yet
- Intravenous FluidsDocument3 pagesIntravenous FluidsKristine Artes AguilarNo ratings yet
- Breast Ultrasound For The Interventionalist: Madhavi Raghu, MD, and Regina Hooley, MDDocument7 pagesBreast Ultrasound For The Interventionalist: Madhavi Raghu, MD, and Regina Hooley, MDrasminojNo ratings yet
- Proposal Research NewDocument25 pagesProposal Research NewNndaydnaNo ratings yet
- SOGC DVT ProphylaxisDocument16 pagesSOGC DVT Prophylaxisibrahimnazeh96No ratings yet
- Roles of Bone Marrow Transplant Unit Nurses IncludesDocument10 pagesRoles of Bone Marrow Transplant Unit Nurses IncludesGleden UmayamNo ratings yet
- Types of GastrostomyDocument4 pagesTypes of GastrostomyChad AlsayNo ratings yet
- Anesthesia and Perioperative Management of Colorectal Surgical Patients - Specific Issues (Part 2)Document10 pagesAnesthesia and Perioperative Management of Colorectal Surgical Patients - Specific Issues (Part 2)Syauqi DarussalamNo ratings yet
- ChemoDocument54 pagesChemoKarren FernandezNo ratings yet
- Laryngeal Cancer 1Document49 pagesLaryngeal Cancer 1Kpj KpjNo ratings yet
- C AnnulationDocument15 pagesC AnnulationSaffronMaeNo ratings yet
- Routes of Drug AdministrationDocument4 pagesRoutes of Drug AdministrationJoeyNo ratings yet
- Picc Infection PDFDocument16 pagesPicc Infection PDFMahesh ChandraNo ratings yet
- Central Venous Access DevicesDocument6 pagesCentral Venous Access DevicesAllan MacacapagalNo ratings yet
- Endoscopy - Hysteroscopy and Laparoscopy Indications, Contraindications and ComplicationsDocument16 pagesEndoscopy - Hysteroscopy and Laparoscopy Indications, Contraindications and Complicationsselatur100% (1)
- Cancer Regional Therapy: HAI, HIPEC, HILP, ILI, PIPAC and BeyondFrom EverandCancer Regional Therapy: HAI, HIPEC, HILP, ILI, PIPAC and BeyondNo ratings yet
- Intravenous Therapy Administration: a practical guideFrom EverandIntravenous Therapy Administration: a practical guideRating: 4 out of 5 stars4/5 (1)
- Drug Development: New Chemical Entity DevelopmentDocument6 pagesDrug Development: New Chemical Entity DevelopmentDeenNo ratings yet
- Drug-Induced Hepatotoxicity - Overview, Metabolism of Drugs, Clinical and Pathological Manifestations of Drug-Induced Liver DiseaseDocument20 pagesDrug-Induced Hepatotoxicity - Overview, Metabolism of Drugs, Clinical and Pathological Manifestations of Drug-Induced Liver Diseaseal ghiffari muhammad rayhan100% (1)
- European Consensus On The Management of RDSDocument41 pagesEuropean Consensus On The Management of RDSDeddy Supriyadi100% (1)
- Pyanosid - Powder 3753 K 0317 Engl - 01Document5 pagesPyanosid - Powder 3753 K 0317 Engl - 01Ionuţ BuţurcăNo ratings yet
- End-Plate PotentialDocument7 pagesEnd-Plate PotentialSitrak OnyNo ratings yet
- Basic Pharmacology: NTA Level 4 Semester 2Document12 pagesBasic Pharmacology: NTA Level 4 Semester 2MabusiNo ratings yet
- Beginners Guide To Anabolic Steroids PDFDocument84 pagesBeginners Guide To Anabolic Steroids PDFLeo AlbertoNo ratings yet
- Clin Pharm 151 Review Test A. Multiple ChoiceDocument4 pagesClin Pharm 151 Review Test A. Multiple ChoiceAngel GoNo ratings yet
- TYRX BrochureDocument28 pagesTYRX Brochureleo chiuNo ratings yet
- B Pharm 4 Sem Pharmalite - inDocument17 pagesB Pharm 4 Sem Pharmalite - inGanga (Sandeep Pilania)No ratings yet
- Febuxostat in GoutDocument7 pagesFebuxostat in GoutLia NadaNo ratings yet
- Pharmacovigilance Responsibilities of Medicine Sponsors: Australian Recommendations and RequirementsDocument44 pagesPharmacovigilance Responsibilities of Medicine Sponsors: Australian Recommendations and RequirementsResmy JoseNo ratings yet
- Unit 3 - Cology 3Document25 pagesUnit 3 - Cology 3Shreyas ShreyuNo ratings yet
- ChromoblastomycosisDocument90 pagesChromoblastomycosisTara Sefanya KairupanNo ratings yet
- How To Cite A Record On A Clinical Trials Register: Table: Examples of Citation Format Registry Example CitationDocument1 pageHow To Cite A Record On A Clinical Trials Register: Table: Examples of Citation Format Registry Example CitationSebastiánRodríguezNo ratings yet
- Acupuncture and Cancer - David O'Regan, Jacqueine Filshie - The Royal Marsden Hospital, London and Surrey, UKDocument6 pagesAcupuncture and Cancer - David O'Regan, Jacqueine Filshie - The Royal Marsden Hospital, London and Surrey, UKFredericoNo ratings yet
- DHEA and Its Transformation Into Androgens and Estrogens in Peripheral Target Tissues: IntracrinologyDocument28 pagesDHEA and Its Transformation Into Androgens and Estrogens in Peripheral Target Tissues: IntracrinologyFernanda PérezNo ratings yet
- MBBS - General Medicine Reg Id: KMC - 142105 RX ID: 406824261Document1 pageMBBS - General Medicine Reg Id: KMC - 142105 RX ID: 406824261Dipam HalderNo ratings yet
- Zyrtec: Tablet Core: Tablet CoatingDocument5 pagesZyrtec: Tablet Core: Tablet CoatingDwi WirastomoNo ratings yet
- Sincope Vs Crisis - Lancet Neurol 2006 PDFDocument10 pagesSincope Vs Crisis - Lancet Neurol 2006 PDFLina HerreraNo ratings yet
- Prescription: DownloadDocument12 pagesPrescription: DownloadkalpanajainNo ratings yet
- Handy Chart PsychosisDocument3 pagesHandy Chart Psychosismerryavie45No ratings yet
- History of PharmacyDocument33 pagesHistory of Pharmacymalokkhan183No ratings yet
- Kontrol Anes PasienDocument4 pagesKontrol Anes Pasienzidni fatayanNo ratings yet
- CV - 5-2023Document7 pagesCV - 5-2023api-668616332No ratings yet
- CDHO Factsheet AsthmaDocument4 pagesCDHO Factsheet AsthmaIlse AnzuresNo ratings yet
- Classification of Hormones: By. Dr. Luna PhukanDocument13 pagesClassification of Hormones: By. Dr. Luna Phukanacrehell8No ratings yet
- Daftar Harga: Pt. Bernofarm Marketing IvDocument4 pagesDaftar Harga: Pt. Bernofarm Marketing IvSofyan HadiNataNo ratings yet
- Excipient-Free Pulmonary Insulin Dry PowderDocument9 pagesExcipient-Free Pulmonary Insulin Dry PowderYaninaDeLafuenteNo ratings yet