Download as pptx, pdf, or txt
You might also like
- IB Biology (Student Workbook) (Richard Allan)Document456 pagesIB Biology (Student Workbook) (Richard Allan)Masood Ahmad93% (15)
- Biology Lab 1 Bioinformatic Report CorrectedDocument5 pagesBiology Lab 1 Bioinformatic Report CorrectedKasia DrewniakNo ratings yet
- Infections Part 2Document56 pagesInfections Part 2nicu.aiims24No ratings yet
- Waqas Ahmed Usmani ROLL NO 17-78Document41 pagesWaqas Ahmed Usmani ROLL NO 17-78Waqas Ahmed UsmaniNo ratings yet
- WHO GuidelinesDocument45 pagesWHO GuidelinessebastianNo ratings yet
- Congenital Syphilis Clinical Pocket CardDocument2 pagesCongenital Syphilis Clinical Pocket Cardf.sistersonNo ratings yet
- PertussisDocument11 pagesPertussissribaccayNo ratings yet
- Paediatric Guidelines Nephrotic Syndrome 2018Document8 pagesPaediatric Guidelines Nephrotic Syndrome 2018lilydariniNo ratings yet
- Febrile SeizureDocument43 pagesFebrile Seizureabrarbashir40No ratings yet
- Case Files in PediaDocument16 pagesCase Files in Pediavimal rajNo ratings yet
- Syphilis in PregnancyDocument34 pagesSyphilis in Pregnancylalee704No ratings yet
- Pertussis: Dr. Turki Bukhari Pediatric R2 at PSMMCDocument23 pagesPertussis: Dr. Turki Bukhari Pediatric R2 at PSMMCnarNo ratings yet
- Common Tropical Disease in ThailandDocument84 pagesCommon Tropical Disease in ThailandDr.Sathaporn KunnathumNo ratings yet
- Optional Vaccination-2Document57 pagesOptional Vaccination-2Sainath GhaliNo ratings yet
- COVID in PregnancyDocument5 pagesCOVID in PregnancyRajanNo ratings yet
- Eposter Infants of Mothers With Syphilis Glabela CPDocument1 pageEposter Infants of Mothers With Syphilis Glabela CPGlabela Christiana PandangoNo ratings yet
- 5 PertussisDocument25 pages5 PertussisDevendra Singh TomarNo ratings yet
- Topic 10 PMTCTDocument20 pagesTopic 10 PMTCTElungatNo ratings yet
- Upadated Management of TB: Dr. Mohammed Aqib Javed Assistatnt Registrar, MU-I SZMCHDocument47 pagesUpadated Management of TB: Dr. Mohammed Aqib Javed Assistatnt Registrar, MU-I SZMCHNusrat JahanNo ratings yet
- COVID-19 Made Easy - Edited MarsillaDocument57 pagesCOVID-19 Made Easy - Edited MarsillaSyamim AsyrafNo ratings yet
- Hiv Co-Morbidities, Ois and NcdsDocument49 pagesHiv Co-Morbidities, Ois and NcdszawadiNo ratings yet
- Paediatric HivDocument8 pagesPaediatric Hivian ismailNo ratings yet
- Community MedicineDocument48 pagesCommunity MedicineKulgaurav RegmiNo ratings yet
- Respiratory Tract Infections - Med DidacticsDocument59 pagesRespiratory Tract Infections - Med Didacticsapi-649060644No ratings yet
- Einc-Updates 231024 214348Document7 pagesEinc-Updates 231024 214348Alexander Nicole DomingoNo ratings yet
- SyphilisDocument22 pagesSyphilisKishor K AdhikariNo ratings yet
- Toxoplasmosis in PregnancyDocument45 pagesToxoplasmosis in PregnancyTahta PambudiNo ratings yet
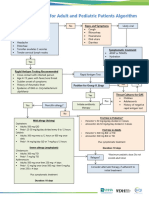
- Outpatient Acute Pharyngitis For Adults and Pediatric Patients Algorithm - FinalDocument1 pageOutpatient Acute Pharyngitis For Adults and Pediatric Patients Algorithm - Finaljmor.3009No ratings yet
- HIV in ChildrenDocument11 pagesHIV in ChildrenVaibhav KrishnaNo ratings yet
- Hiv TreatmentDocument54 pagesHiv TreatmentCharlie BravoNo ratings yet
- 2 Newborn NPIDocument52 pages2 Newborn NPIJoy B. DaladagNo ratings yet
- Hiv in Children AnnDocument6 pagesHiv in Children AnnAdakun SamuelNo ratings yet
- Brucella Presentation To UploadDocument31 pagesBrucella Presentation To UploadDrishti PoudelNo ratings yet
- Opportunistic Infections: Dr. Baldev S. PrajapatiDocument69 pagesOpportunistic Infections: Dr. Baldev S. PrajapatiZazzZaffaNo ratings yet
- STIDocument53 pagesSTIRima HajjarNo ratings yet
- 5.b.intrauterine InfectionDocument31 pages5.b.intrauterine InfectionPriyanka Dyah SetioriniNo ratings yet
- CASE PRESENTATION PneumoniaDocument13 pagesCASE PRESENTATION PneumoniaHari Singh RathoreNo ratings yet
- Sine Derivates IM Versus Quinine IV in TreatmentDocument18 pagesSine Derivates IM Versus Quinine IV in TreatmentNiek VersteegdeNo ratings yet
- Antimicrobial Treatment Guidelines For Common Infections enDocument111 pagesAntimicrobial Treatment Guidelines For Common Infections enRoofia VahedianNo ratings yet
- Donor Screening and ProcessingDocument6 pagesDonor Screening and ProcessingIya BangalanNo ratings yet
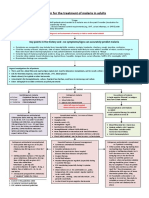
- Algorithm For The Treatment of Malaria in AdultsDocument1 pageAlgorithm For The Treatment of Malaria in AdultsRihab IsmaeelNo ratings yet
- 13 - std1Document1 page13 - std1api-221111168No ratings yet
- IMUNISASI2Document29 pagesIMUNISASI2RatnaSuryatiNo ratings yet
- CH 008 Enteric Fever PDFDocument7 pagesCH 008 Enteric Fever PDFVibojaxNo ratings yet
- Covid-19 Protocols - We Should FollowDocument16 pagesCovid-19 Protocols - We Should Followsakib hossainNo ratings yet
- Treatment, Care and Support For HIV Exposed - 7 Session 2Document79 pagesTreatment, Care and Support For HIV Exposed - 7 Session 2Dr. Hem Sagar GautamNo ratings yet
- 3 Hypertension in PregnancyDocument36 pages3 Hypertension in PregnancySwee WaiNo ratings yet
- Cover Sheet Complicated or Recurrent Uti Pathway 11/2009: Background InformationDocument9 pagesCover Sheet Complicated or Recurrent Uti Pathway 11/2009: Background InformationVisual CortexNo ratings yet
- Viral Hepatitis: Dr. Shami Pokhrel Lecturer Dept. of Pediatrics, LMCDocument12 pagesViral Hepatitis: Dr. Shami Pokhrel Lecturer Dept. of Pediatrics, LMCShami PokhrelNo ratings yet
- Typhoid Fever: Presented By: Dave Jay S. Manriquez, BSN, RNDocument33 pagesTyphoid Fever: Presented By: Dave Jay S. Manriquez, BSN, RNArkais Massah100% (1)
- Case Melita FixedDocument40 pagesCase Melita FixedMelita Aditya SariNo ratings yet
- IMMUNIZATION ScheduleDocument2 pagesIMMUNIZATION Schedulejhonny100% (1)
- Clinical Manifestations and Treatment of Syphilis - UpToDateDocument2 pagesClinical Manifestations and Treatment of Syphilis - UpToDateCarmenDuganNo ratings yet
- Rational Antibiotic UseDocument35 pagesRational Antibiotic UseRahul SharmaNo ratings yet
- TyphoidDocument12 pagesTyphoidmansoorminahil149No ratings yet
- FinalDocument42 pagesFinalmanish shresthaNo ratings yet
- DiphtheriaDocument5 pagesDiphtheriahertezjogie669No ratings yet
- Pprom 1 1Document20 pagesPprom 1 1Tehreem AzharNo ratings yet
- Guidelines Ut I 2012Document1 pageGuidelines Ut I 2012Siti ZulaikhahNo ratings yet
- Prenatal Care AndreDocument29 pagesPrenatal Care AndreAndre PutraNo ratings yet
- Prenatal Care AndreDocument29 pagesPrenatal Care AndreAndre PutraNo ratings yet
- What Is Genetic Testing Results For LifeDocument24 pagesWhat Is Genetic Testing Results For LiferamumyselfNo ratings yet
- Nama: Endah Suryani NPM: 0661 16 179 Kelas: KELAS E'16Document5 pagesNama: Endah Suryani NPM: 0661 16 179 Kelas: KELAS E'16Endah SuryaniNo ratings yet
- Aplastic Hemolitic 2021 OlgaDocument43 pagesAplastic Hemolitic 2021 OlgalaibaNo ratings yet
- Liver Cirrhosis TreatmentDocument5 pagesLiver Cirrhosis TreatmentPrajith NairNo ratings yet
- D0685 Biology Paper2Document9 pagesD0685 Biology Paper2Aryan SinghNo ratings yet
- Complement: Kathleen Basa Kris Nicole de Guzman Jessica Mae Ong 3HmtDocument70 pagesComplement: Kathleen Basa Kris Nicole de Guzman Jessica Mae Ong 3HmtCherry Reyes-Principe100% (1)
- MARCH - 2023wDocument25 pagesMARCH - 2023wcariappa canvaNo ratings yet
- Biology (044) - Practical Lab Manual (Term - 1)Document24 pagesBiology (044) - Practical Lab Manual (Term - 1)Tejeswar MajhiNo ratings yet
- Lecture 23-Structure and Physiology of Bacteria-Dr. Nenes Prastiwi, M.biomed (2023)Document38 pagesLecture 23-Structure and Physiology of Bacteria-Dr. Nenes Prastiwi, M.biomed (2023)artha maressaNo ratings yet
- 3.infectious MononucleosisDocument9 pages3.infectious Mononucleosiselka.kgmaNo ratings yet
- Cellular and Molecular Mechanisms of Curcumin in Prevention and Treatment of DiseaseDocument55 pagesCellular and Molecular Mechanisms of Curcumin in Prevention and Treatment of DiseaseJorge Luis Plasencia CubaNo ratings yet
- Peptococcus PeptostreptococcusDocument25 pagesPeptococcus PeptostreptococcusIon PopescuNo ratings yet
- Dental Caries DefinitionDocument11 pagesDental Caries DefinitioncartoonNo ratings yet
- NIH Project Narrative Template: ContentDocument2 pagesNIH Project Narrative Template: ContentJoedhel Lloyd ObordoNo ratings yet
- Laboratory Diagnosis of Sexually Transmited DiseasesDocument31 pagesLaboratory Diagnosis of Sexually Transmited DiseasesrikarzNo ratings yet
- Potential Use of Probiotics: Ekachai ChukeatiroteDocument8 pagesPotential Use of Probiotics: Ekachai ChukeatiroteDanu EffendiNo ratings yet
- Phage PosterDocument1 pagePhage Posterapi-529961637No ratings yet
- Chapter 6Document69 pagesChapter 6علوم طبية AUG 2020No ratings yet
- Test Bank For Foundations in Microbiology 8th Edition Kathleen P TalaroDocument14 pagesTest Bank For Foundations in Microbiology 8th Edition Kathleen P Talaromisbodensquallyr5g5pNo ratings yet
- Schlossbergs Clinical Infectious Disease Team Ira True 3Rd Edition Cheston B Cunha Editor Online Ebook Texxtbook Full Chapter PDFDocument69 pagesSchlossbergs Clinical Infectious Disease Team Ira True 3Rd Edition Cheston B Cunha Editor Online Ebook Texxtbook Full Chapter PDFjohn.principe668100% (9)
- Topic 1.1 Test (Science 10) : Relevance Extending Proficient Developing EmergingDocument2 pagesTopic 1.1 Test (Science 10) : Relevance Extending Proficient Developing EmergingJeffrey PiggottNo ratings yet
- Staphylococcus EpidermidisDocument4 pagesStaphylococcus Epidermidisemanuel santiago triana rujanaNo ratings yet
- Grand Round: Done By:Dr:Mada Yateem Moderator:Dr: Ibraheem AbaasDocument30 pagesGrand Round: Done By:Dr:Mada Yateem Moderator:Dr: Ibraheem AbaasMada AlhyatNo ratings yet
- Unit 1 Scope of Microbiology BSNDocument7 pagesUnit 1 Scope of Microbiology BSNHannah TotohNo ratings yet
- Hygisoft For FarmsDocument8 pagesHygisoft For FarmsHariprasad ManavalanNo ratings yet
- FatimaDocument2 pagesFatimamstoomeNo ratings yet
- Week 2 Cellular LevelDocument7 pagesWeek 2 Cellular LevelDayledaniel Sorveto100% (1)
- Annex 3: Recommendations To Assure The Quality, Safety and Efficacy of BCG VaccinesDocument50 pagesAnnex 3: Recommendations To Assure The Quality, Safety and Efficacy of BCG VaccinesDemo 1002No ratings yet