Download as pptx, pdf, or txt
You might also like
- 2012 BRAKES VSA System Components - TL PDFDocument114 pages2012 BRAKES VSA System Components - TL PDFsoftallNo ratings yet
- BioconstructivismsDocument12 pagesBioconstructivismsweareyoung5833No ratings yet
- TBL - CNS InfectionDocument32 pagesTBL - CNS InfectionAzizul Halid100% (1)
- Pt6a Engine Training OverwiewDocument20 pagesPt6a Engine Training OverwiewRafael Alves Dos Santos100% (1)
- Uhone Broker GuideDocument28 pagesUhone Broker Guidestech137No ratings yet
- Strut BucklingDocument9 pagesStrut BucklingWai Sheng75% (4)
- 13 Meningitis Beyond Neonatal AgeDocument57 pages13 Meningitis Beyond Neonatal AgeABDELA DAFO IJARONo ratings yet
- Dr. AR - Cns Infection Utk RPSDocument57 pagesDr. AR - Cns Infection Utk RPSKevin KarimNo ratings yet
- 20 Bacterial MeningitisDocument35 pages20 Bacterial MeningitisBhakti WashilkarNo ratings yet
- Ali - CNS InfectionsDocument129 pagesAli - CNS InfectionsMichael BortzNo ratings yet
- Tuberculous MeningitisDocument11 pagesTuberculous MeningitiszuhriNo ratings yet
- Menigitis EncephalitisDocument63 pagesMenigitis EncephalitisHussain Azhar100% (1)
- DR Prakash Nag MD Medicine NGMCDocument61 pagesDR Prakash Nag MD Medicine NGMCSamjhana NeupaneNo ratings yet
- CNS Bacterial Infections: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaDocument47 pagesCNS Bacterial Infections: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaJanPaulaDelaPenaNo ratings yet
- Meningitis Beyond The Neonatal AgeDocument51 pagesMeningitis Beyond The Neonatal AgeBeamlak Getachew WoldeselassieNo ratings yet
- Cns Infection 3rd Year MBBSDocument66 pagesCns Infection 3rd Year MBBSKritick BhandariNo ratings yet
- 2011 CNS Bacterial InfectionDocument47 pages2011 CNS Bacterial InfectionZEMENAY TRUNEHNo ratings yet
- Neuro SepsisDocument18 pagesNeuro SepsisRed DevilNo ratings yet
- Meningococcal Meningitis - DR Ooi Phaik YeeDocument66 pagesMeningococcal Meningitis - DR Ooi Phaik YeeNg Chee KeongNo ratings yet
- Acutemeningoencephalitis 170309112245Document41 pagesAcutemeningoencephalitis 170309112245jinsi georgeNo ratings yet
- Meningitis LectureDocument20 pagesMeningitis LectureIDIOVWA PRINCENo ratings yet
- Central Nervous System InfectionsDocument49 pagesCentral Nervous System InfectionsYogi SanjayaNo ratings yet
- Diseases of The Nervous System: Nester 5th. EdDocument165 pagesDiseases of The Nervous System: Nester 5th. EdREBECCA IMPLICANo ratings yet
- MeningitisDocument46 pagesMeningitisKural ArasanNo ratings yet
- CNS Infections: Rashmi KumarDocument32 pagesCNS Infections: Rashmi Kumarfasil tadesseNo ratings yet
- Brain InfectionDocument61 pagesBrain Infectionmanisha paikarayNo ratings yet
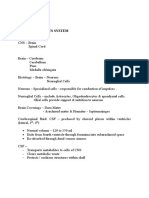
- Pathology of The CNS: Presented by Associated Professor/ Rehab KamalDocument25 pagesPathology of The CNS: Presented by Associated Professor/ Rehab KamalAhmed TarekNo ratings yet
- Meningococcal Infection (Lec4)Document8 pagesMeningococcal Infection (Lec4)Ali Al.JuffairiNo ratings yet
- Acute Bacterial MeningitisDocument40 pagesAcute Bacterial Meningitissinte beyuNo ratings yet
- Meningitis: Presented By:dr. Alaa Nugud ABH-Medical DepartmentDocument23 pagesMeningitis: Presented By:dr. Alaa Nugud ABH-Medical DepartmentALaa NugudNo ratings yet
- Meningitis PLUS: Goetz: Textbook of Clinical Neurology, 1st EdDocument1 pageMeningitis PLUS: Goetz: Textbook of Clinical Neurology, 1st Edintrovoyz041No ratings yet
- 2020 11 20 CNS Infections MitsiasDocument75 pages2020 11 20 CNS Infections MitsiasΖέτα ΤσίρκαNo ratings yet
- Acute Rheumatic Fever: Stephanie Grace C. Lucero Clinical ClerkDocument65 pagesAcute Rheumatic Fever: Stephanie Grace C. Lucero Clinical ClerkStacy LuceroNo ratings yet
- Meningitis 2006Document34 pagesMeningitis 2006Laura DavisNo ratings yet
- Central Nervous SystemDocument16 pagesCentral Nervous SystemMalarameshNo ratings yet
- MeningitisDocument42 pagesMeningitisRajesh YadavNo ratings yet
- Viral MeningitisDocument19 pagesViral MeningitisUneebNo ratings yet
- Mening Enceph Old PatDocument64 pagesMening Enceph Old PatmutiaNo ratings yet
- Infections of The Eyes and The Central Nervous System - Dr. CerradaDocument68 pagesInfections of The Eyes and The Central Nervous System - Dr. CerradaMonique BorresNo ratings yet
- Meningitis AND Encephalitis: by DR .. Magdi Elbaloola Ahmed Physcian & GastrohepatologistDocument51 pagesMeningitis AND Encephalitis: by DR .. Magdi Elbaloola Ahmed Physcian & GastrohepatologistÅbübâkêř Äbd-ëřhēēm BãřřîNo ratings yet
- W2D3 DR - Yasa-Bacteremia Dan SepsisDocument54 pagesW2D3 DR - Yasa-Bacteremia Dan SepsisJaka BawaviNo ratings yet
- Clinical Infectious Disease Nplex ReviewDocument64 pagesClinical Infectious Disease Nplex ReviewValeria AcevedoNo ratings yet
- Kuliah Infeksi SSP 2021Document85 pagesKuliah Infeksi SSP 2021clarissaNo ratings yet
- Acute Bacterial Meningitis in ChildrenDocument48 pagesAcute Bacterial Meningitis in ChildrenRadhika BatraNo ratings yet
- Infections of The Eyes and The Central Nervous System by Dr. Joan E. CerradaDocument68 pagesInfections of The Eyes and The Central Nervous System by Dr. Joan E. CerradaMonique BorresNo ratings yet
- Biological Warfare: Renaat A. A. M. Peleman, MD, PHD Dept Internal Med, Div Infect Dis University Hospital GhentDocument63 pagesBiological Warfare: Renaat A. A. M. Peleman, MD, PHD Dept Internal Med, Div Infect Dis University Hospital GhentAbdullah Al-RashedNo ratings yet
- Meningitis AskepDocument44 pagesMeningitis AskepNizZa TakaricoNo ratings yet
- Infeksi Susunan Saraf Pusat, Cerebral Palsy DanDocument64 pagesInfeksi Susunan Saraf Pusat, Cerebral Palsy DanRizky KurniawanNo ratings yet
- Rheumatic Fever: DR: Yousif Adam AliDocument20 pagesRheumatic Fever: DR: Yousif Adam AliÅbübâkêř Äbd-ëřhēēm BãřřîNo ratings yet
- CNS Infection 11Document75 pagesCNS Infection 11Paulo Josue SabladNo ratings yet
- FEVER - FUO - RASH Into To Medicine - First YearDocument93 pagesFEVER - FUO - RASH Into To Medicine - First YearJoseph De JoyaNo ratings yet
- Tuberculous MeningitisDocument32 pagesTuberculous MeningitisRadhika BatraNo ratings yet
- Sepsis and Septic ShockDocument70 pagesSepsis and Septic ShockLily SolNo ratings yet
- Anak 3.1 Infective Endocarditis DRTLTDocument21 pagesAnak 3.1 Infective Endocarditis DRTLTAnastasia PinkyNo ratings yet
- Meningitis - Practice Essentials, Background, PathophysiologyDocument26 pagesMeningitis - Practice Essentials, Background, PathophysiologydilaNo ratings yet
- 2 - RH Fev, Inf EndoDocument37 pages2 - RH Fev, Inf EndoLobna ElkilanyNo ratings yet
- Asuhan Keperawatan Pada Klien Dengan Meningitis: Retno LestariDocument57 pagesAsuhan Keperawatan Pada Klien Dengan Meningitis: Retno Lestariaha ehe ohoNo ratings yet
- Fever and SepsisDocument24 pagesFever and Sepsis180045No ratings yet
- Fuo, Sepsis and Septic Shock: Clinical Clerk Mary Christine S. IlangaDocument62 pagesFuo, Sepsis and Septic Shock: Clinical Clerk Mary Christine S. IlangaPraise BechaydaNo ratings yet
- Lect MeningitisDocument33 pagesLect Meningitisnwogu.kamsiyoNo ratings yet
- TBMDocument47 pagesTBMstephen X-SILVERNo ratings yet
- Infection 2 1Document91 pagesInfection 2 1saeedassaf97No ratings yet
- Rheumatic Heart DiseaseDocument97 pagesRheumatic Heart DiseaseShubham gaurNo ratings yet
- UCCN2003 TCP/IP Internetworking UCCN2243 Internetworking Principles & PracticesDocument10 pagesUCCN2003 TCP/IP Internetworking UCCN2243 Internetworking Principles & PracticesKahtheresh MuruganNo ratings yet
- CMP002Document98 pagesCMP002Black kosmosNo ratings yet
- Honeywell DPR 2300 and 3000Document338 pagesHoneywell DPR 2300 and 3000kmpoulosNo ratings yet
- Something ImpossibleDocument21 pagesSomething ImpossibleRegina BerengoltsNo ratings yet
- 2000 Series Design TablesDocument36 pages2000 Series Design Tablesjunhe898No ratings yet
- E E E E: For Installation/s IndustrialDocument1 pageE E E E: For Installation/s IndustrialRJ Padilla0% (1)
- BeamDocument23 pagesBeamMohammad YusufNo ratings yet
- UntitledDocument136 pagesUntitledjhon rodriguezNo ratings yet
- 2014 BGCSE Biology Paper 4Document8 pages2014 BGCSE Biology Paper 4cleohambiraNo ratings yet
- 0 1 NO. Ga. of Vibrating Screen Bs 5' X 12' TD 53-270610-5XX 7Document4 pages0 1 NO. Ga. of Vibrating Screen Bs 5' X 12' TD 53-270610-5XX 7Benjamin MurphyNo ratings yet
- Thesis Statements: The Bad and The BetterDocument2 pagesThesis Statements: The Bad and The BetterKiraNo ratings yet
- Lesson 3 English For Specific PurposesDocument14 pagesLesson 3 English For Specific PurposesJudith CastilloNo ratings yet
- Cairnhill Nine FactsheetDocument7 pagesCairnhill Nine Factsheetapi-276519044No ratings yet
- Brochure-Gever-2020 ASTM B819Document2 pagesBrochure-Gever-2020 ASTM B819sahriNo ratings yet
- The Real Green Revolution Organic and Agroecological FarmingDocument151 pagesThe Real Green Revolution Organic and Agroecological FarmingKlausEllegaard11No ratings yet
- Educ. 2 The Teaching Profession: Lesson 2Document7 pagesEduc. 2 The Teaching Profession: Lesson 2Cristy Ramos BitorNo ratings yet
- Motion in Electric Fields: SACE Stage 2 PhysicsDocument43 pagesMotion in Electric Fields: SACE Stage 2 Physicsrampravesh kumarNo ratings yet
- Design of Screw FasteningDocument37 pagesDesign of Screw FasteningDhayane RedoquerioNo ratings yet
- DLTO WhitePaperDocument6 pagesDLTO WhitePaperNoven da LopezNo ratings yet
- History of Civil EngineerDocument3 pagesHistory of Civil EngineerErnest 1TNo ratings yet
- Toxic Substances and Hazardous and Nuclear Wastes Control Act of 1990Document20 pagesToxic Substances and Hazardous and Nuclear Wastes Control Act of 1990Jeong100% (1)
- Genphysics q2 Mod5Document28 pagesGenphysics q2 Mod5Mhasie Joy PondevidaNo ratings yet
- Quadra - 001Document1 pageQuadra - 001Prasetya PamungkasNo ratings yet
- Chef Danielle Peita Graham InterviewDocument2 pagesChef Danielle Peita Graham InterviewSeah Pei JunNo ratings yet
- Graphing Quadratic Functions in Standard Form Lesson PlanDocument2 pagesGraphing Quadratic Functions in Standard Form Lesson Planapi-401400552100% (1)