Download as pptx, pdf, or txt
You might also like
- A Diet ProblemDocument10 pagesA Diet Problemabdul ghaffarNo ratings yet
- ECG Apib PDFDocument68 pagesECG Apib PDFArthur KakarekoNo ratings yet
- A Little Princess Folan Miller June 2018Document119 pagesA Little Princess Folan Miller June 2018Aiden Condron100% (1)
- In The Following Table We Consider How Alex Tyler andDocument1 pageIn The Following Table We Consider How Alex Tyler andtrilocksp SinghNo ratings yet
- Traction Is A Mechanical Force Applied To TheDocument3 pagesTraction Is A Mechanical Force Applied To TheAshley Franceska CansanayNo ratings yet
- Red Flags: Indications For Urgent ReferralDocument5 pagesRed Flags: Indications For Urgent ReferralEndah Novianti SoenarsinNo ratings yet
- Musculoskeletal Trauma RSIJPKDocument41 pagesMusculoskeletal Trauma RSIJPKPegyNo ratings yet
- 5 - Knee DisordersDocument85 pages5 - Knee Disordersraed faisalNo ratings yet
- Musculoskeletal Trauma FracturesDocument47 pagesMusculoskeletal Trauma FracturesLydia Lopz MsnrncdNo ratings yet
- Musculoskeletal DisordersDocument26 pagesMusculoskeletal DisorderselishaNo ratings yet
- Orthopaedic Emergencies AndreDocument49 pagesOrthopaedic Emergencies AndreLusi MunawarohNo ratings yet
- Orthopedics PDFDocument14 pagesOrthopedics PDFSam christenNo ratings yet
- CARE of ADOLESCENTSDocument15 pagesCARE of ADOLESCENTSaprilkate banagodosNo ratings yet
- Talus FracturesDocument19 pagesTalus Fracturessundar persaudNo ratings yet
- Handout Lat Elbow Pain PDFDocument47 pagesHandout Lat Elbow Pain PDFgemichan26No ratings yet
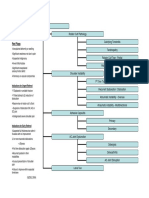
- NHS UK Diagnosis of Shoulder ProblemsDocument1 pageNHS UK Diagnosis of Shoulder ProblemsmertNo ratings yet
- Cad wk9-10 QsDocument10 pagesCad wk9-10 Qsapi-468597987No ratings yet
- College of Health Sciences: Sultan Kudarat State UniversityDocument8 pagesCollege of Health Sciences: Sultan Kudarat State UniversityGeremie Magno Mana-ayNo ratings yet
- MedSurg Chapter 51 OutlineDocument7 pagesMedSurg Chapter 51 OutlineJosephine Navarro100% (1)
- NCM 116 - Musculoskeletal Conditions Part 3Document21 pagesNCM 116 - Musculoskeletal Conditions Part 3Gabrielle Frances FernandezNo ratings yet
- Warning: You May Want To Look Away at Times!: Youtube VideoDocument47 pagesWarning: You May Want To Look Away at Times!: Youtube VideoRaffy B. MabilingNo ratings yet
- Lesson - Elbow Region Examination and EvaluationDocument8 pagesLesson - Elbow Region Examination and EvaluationJULIANE MAE BALANGNo ratings yet
- Hip Disloc and Fem HeadDocument60 pagesHip Disloc and Fem HeadZisuhNo ratings yet
- Proximal BicepsDocument23 pagesProximal BicepsPrabath ChinthakaNo ratings yet
- Medical Rehabilitation in Musculoskeletal Trauma - Prof. Dr. Dr. Angela BM Tulaar SPKFR (K)Document41 pagesMedical Rehabilitation in Musculoskeletal Trauma - Prof. Dr. Dr. Angela BM Tulaar SPKFR (K)YanuarNo ratings yet
- Common Sports Injuries: Ukris Gunadham, MD, FRCOST Department of Orthopaedics Trang HospitalDocument71 pagesCommon Sports Injuries: Ukris Gunadham, MD, FRCOST Department of Orthopaedics Trang HospitalMohammed SaqoorNo ratings yet
- Bone Do PDFDocument41 pagesBone Do PDFROMULO NU�EZ JR.No ratings yet
- Acute Ankle Inversion Injuries: SubjectiveDocument7 pagesAcute Ankle Inversion Injuries: Subjectivegemichan26No ratings yet
- Compartment Syndrome: Rahma Aulia KhairunnisaDocument23 pagesCompartment Syndrome: Rahma Aulia KhairunnisawildaNo ratings yet
- Sprains, Strains, Dislocations & Subluxations, Carpal Tunnel & Other Related InjuriesDocument26 pagesSprains, Strains, Dislocations & Subluxations, Carpal Tunnel & Other Related InjuriesLydia Lopz MsnrncdNo ratings yet
- Radiographic Diagnosis For Canine Hip Dysplasia: 18 August 2021Document85 pagesRadiographic Diagnosis For Canine Hip Dysplasia: 18 August 2021Thirada sosawangNo ratings yet
- Foot and Ankle Injuries and Pain: Indranil Neel' Kushare, MDDocument55 pagesFoot and Ankle Injuries and Pain: Indranil Neel' Kushare, MDrizwan.mughal1997No ratings yet
- Blok Musculoskeletal 2017 Sy Materi KuliahDocument106 pagesBlok Musculoskeletal 2017 Sy Materi KuliahBakingpancakesNo ratings yet
- Shoulder and Hip DislocationDocument40 pagesShoulder and Hip DislocationprestigeuniversaltradingNo ratings yet
- Spinal Cord Injury FinalDocument3 pagesSpinal Cord Injury FinalAa AaNo ratings yet
- Surgery - Dychioco - Musculo Skeletal InjuriesDocument79 pagesSurgery - Dychioco - Musculo Skeletal Injuries3rd yrsNo ratings yet
- Pediatric Fractures QT PDFDocument42 pagesPediatric Fractures QT PDFyanNo ratings yet
- Chapter 18 Vocab: Condyle Articular Cartilage Medial Meniscus Lateral Meniscus Anterior Cruciate Ligament (ACL)Document4 pagesChapter 18 Vocab: Condyle Articular Cartilage Medial Meniscus Lateral Meniscus Anterior Cruciate Ligament (ACL)mph440No ratings yet
- Paediatric OrthopaedicsDocument80 pagesPaediatric OrthopaedicsShimmering MoonNo ratings yet
- Assessment of The Musculoskeletal SystemDocument45 pagesAssessment of The Musculoskeletal Systemstudentme annNo ratings yet
- GP Assessment of The Shoulder: Keith Littlebury MSC Grad Dip Phys Extended Scope Physiotherapist Camden Cats ServiceDocument29 pagesGP Assessment of The Shoulder: Keith Littlebury MSC Grad Dip Phys Extended Scope Physiotherapist Camden Cats ServiceapriliatnaNo ratings yet
- 3.2 Management of Musculoskeltal Disorders PDFDocument2 pages3.2 Management of Musculoskeltal Disorders PDFDiana CalderonNo ratings yet
- Nursing Care of Fracture-1Document18 pagesNursing Care of Fracture-1sutajiNo ratings yet
- Scfe PDFDocument39 pagesScfe PDFMuhammad Tabish SaleemNo ratings yet
- 11 - Fraktur Dan DislokasiDocument47 pages11 - Fraktur Dan DislokasiCarolyn ZhouNo ratings yet
- Knee&Foot Part1Document28 pagesKnee&Foot Part1SarkawtNo ratings yet
- Low Back and SacrumDocument27 pagesLow Back and SacrumdwNo ratings yet
- 2 IntroductionDocument41 pages2 IntroductionRadwa TalaatNo ratings yet
- Betsy Johnson, MSN, CPNP-PCDocument75 pagesBetsy Johnson, MSN, CPNP-PCGelsey Gelsinator JianNo ratings yet
- Dr. Luthfi Hidayat, SP - OTDocument39 pagesDr. Luthfi Hidayat, SP - OTadystiNo ratings yet
- Musculoskeletal Disorders (For Students)Document5 pagesMusculoskeletal Disorders (For Students)Chaina MacaspacNo ratings yet
- Principles of Soft TissueDocument24 pagesPrinciples of Soft TissueEric Carlos YumulNo ratings yet
- Sprains and StrainsDocument23 pagesSprains and StrainsokaciaNo ratings yet
- S T O P: Ports Rauma and Veruse ReventionDocument37 pagesS T O P: Ports Rauma and Veruse ReventionNabiha AjmalNo ratings yet
- Week 8 Category 2Document4 pagesWeek 8 Category 2api-468093714No ratings yet
- Shoulder InjuriesDocument66 pagesShoulder InjuriesNicks KumarNo ratings yet
- Comprehensive SummaryDocument37 pagesComprehensive Summaryhrg79qzwc2No ratings yet
- 4 Shoulder JointDocument50 pages4 Shoulder Jointq77gkyhzs4No ratings yet
- Contusions, Sprains, StrainsDocument14 pagesContusions, Sprains, StrainsKaryn Joy LamisNo ratings yet
- Week 16 - Musculoskeletal Disease in ChildrenDocument51 pagesWeek 16 - Musculoskeletal Disease in ChildrenJaja ManezNo ratings yet
- AnD FT Elbow-1Document26 pagesAnD FT Elbow-1Nazwa KamilatunnisaNo ratings yet
- Sport Injuries: ShoulderDocument67 pagesSport Injuries: ShoulderNabiha AjmalNo ratings yet
- Knee ExaminationDocument14 pagesKnee ExaminationAsimNo ratings yet
- Sprain and Strains, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandSprain and Strains, A Simple Guide to the Condition, Treatment and Related DiseasesNo ratings yet
- Security Guard Training & OSHA Training NY Guardian Group ServicesDocument1 pageSecurity Guard Training & OSHA Training NY Guardian Group ServicesLochard BaptisteNo ratings yet
- Drawing AidsDocument15 pagesDrawing Aidsbra9tee9tiniNo ratings yet
- CXA 1238 DatasheetDocument58 pagesCXA 1238 DatasheetHoan TranNo ratings yet
- MCQon PM PDFDocument11 pagesMCQon PM PDFKathirrveluSubramainanNo ratings yet
- Critical Wear Areas & Vacuum Test Locations: Upper Valve Body - 6F50 ShownDocument4 pagesCritical Wear Areas & Vacuum Test Locations: Upper Valve Body - 6F50 ShownautomaticosbrasilNo ratings yet
- 123Document10 pages123Aryan SanezNo ratings yet
- Pulse in The Stomach - Could It Be An Abdominal Aortic AneurysmDocument3 pagesPulse in The Stomach - Could It Be An Abdominal Aortic AneurysmLazar VučetićNo ratings yet
- B.tech Chem Lab ManualDocument40 pagesB.tech Chem Lab Manualsushil joshiNo ratings yet
- Elena Rodriguez Reflective EssayDocument1 pageElena Rodriguez Reflective EssayElena Rodriguez ZuletaNo ratings yet
- TSX Cusb485Document2 pagesTSX Cusb485AurellioNo ratings yet
- Melon Growing Tips PDFDocument1 pageMelon Growing Tips PDFTaahirah Ben ZinatNo ratings yet
- Non-Circumvention, Non-Disclosure Agreement (Ncnda)Document5 pagesNon-Circumvention, Non-Disclosure Agreement (Ncnda)fabrizio ballesiNo ratings yet
- GH2023 - 5876 Saturin & Minh Enhancing Efficiency of Geotechnical Design For Offshore MonopileDocument7 pagesGH2023 - 5876 Saturin & Minh Enhancing Efficiency of Geotechnical Design For Offshore MonopileMinh Nguyen-AnhNo ratings yet
- FusionServer Tools V2R2 Umate User Guide 21Document340 pagesFusionServer Tools V2R2 Umate User Guide 21Mwenya Scot MusondaNo ratings yet
- Flashcards - Topic 6.1 6.4 - Microbiology - Edexcel IAL Biology A LevelDocument49 pagesFlashcards - Topic 6.1 6.4 - Microbiology - Edexcel IAL Biology A LevelULFANo ratings yet
- Unit II - MCMTDocument50 pagesUnit II - MCMTSai RamNo ratings yet
- Genetics Linkage and Crossing OverDocument94 pagesGenetics Linkage and Crossing OverSurabhiNo ratings yet
- Greymouth Walks BrochureDocument2 pagesGreymouth Walks Brochuremiller999No ratings yet
- Module 5: Building The Teaching Portfolio Related To The Implementation of The ModalitiesDocument2 pagesModule 5: Building The Teaching Portfolio Related To The Implementation of The Modalitiesrom keroNo ratings yet
- Hyponic Full Catalog WEBDocument144 pagesHyponic Full Catalog WEBIsidro Pale CordobaNo ratings yet
- OS Lesson+Plan+and+ObjectivesDocument4 pagesOS Lesson+Plan+and+ObjectivesNikitha Rathnakar0% (2)
- Thar Crde Repair ManualDocument261 pagesThar Crde Repair ManualSugathan AnandanNo ratings yet
- Alkaloid Grupo-1Document6 pagesAlkaloid Grupo-1BRENDA MARYSABEL ESTEBAN HUARINo ratings yet
- Service Manual For L40F3520-MS63F-LA 1Document60 pagesService Manual For L40F3520-MS63F-LA 1AntonioCésarUtrera100% (2)
- Kindergarten Teacher Cover Letter SampleDocument6 pagesKindergarten Teacher Cover Letter Samplektrplormd100% (1)
- Bos 50633Document2 pagesBos 50633Krishna SharmaNo ratings yet