Download as pptx, pdf, or txt
You might also like
- Phonetic PunctuationDocument2 pagesPhonetic Punctuationsclord0167% (3)
- Esvot Proceedings 2010Document772 pagesEsvot Proceedings 2010Morales Alejandro100% (1)
- Rle Case Study - Septic ShockDocument2 pagesRle Case Study - Septic Shockhazel sergioNo ratings yet
- The Effects of Changes in Foreign Exchange Rates: BackgroundDocument24 pagesThe Effects of Changes in Foreign Exchange Rates: BackgroundAA100% (1)
- Graphical Representation of Data PDFDocument12 pagesGraphical Representation of Data PDFMatthew RogersNo ratings yet
- II MSC Medical Surgical Nursing, Urology and Renal NursingDocument1 pageII MSC Medical Surgical Nursing, Urology and Renal NursingBiju AntonyNo ratings yet
- PyodermaDocument19 pagesPyodermaFajar Hidayat RamadhanNo ratings yet
- Basics of English Speaking For Workplace RevisedDocument170 pagesBasics of English Speaking For Workplace Revisedravi96100% (4)
- Visceral Leishmaniasis in IndiaDocument27 pagesVisceral Leishmaniasis in IndiaNishant SrivastavaNo ratings yet
- Community Nutrition ProgrammesDocument44 pagesCommunity Nutrition ProgrammesNeethu VincentNo ratings yet
- Unit 1st: Introduction To Microbiology MicrobiologyDocument2 pagesUnit 1st: Introduction To Microbiology MicrobiologySuneel Kumar PrajapatiNo ratings yet
- Tutorial - Calculations-A-LEVEL-CHEMISTRYDocument4 pagesTutorial - Calculations-A-LEVEL-CHEMISTRYWazeela DelawarallyNo ratings yet
- Community Health One LinersDocument30 pagesCommunity Health One LinersRatan YadavNo ratings yet
- Filariasis in NepalDocument41 pagesFilariasis in NepalBinaya100% (1)
- Hap PDFDocument17 pagesHap PDFRishu Rishma100% (1)
- B.SC Nursing - 2014 - 1 - Nutrition and BiochemistryDocument1 pageB.SC Nursing - 2014 - 1 - Nutrition and BiochemistryPRANGYA TIANo ratings yet
- Shift Work Disorder and Associated Health Problems Among Nursing Staffs Working in A Tertiary Health Centre, Chennai, South IndiaDocument4 pagesShift Work Disorder and Associated Health Problems Among Nursing Staffs Working in A Tertiary Health Centre, Chennai, South IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cleaning A Sutured Wound & Changing A Dressing On A Wound With A Drain Procedure ChecklistDocument3 pagesCleaning A Sutured Wound & Changing A Dressing On A Wound With A Drain Procedure ChecklistMonicaElizadePazNo ratings yet
- National Leprosy Eradication Program - PPTX AkilaDocument51 pagesNational Leprosy Eradication Program - PPTX AkilaPadmapriya SrinivasanNo ratings yet
- Elimination NeedsDocument52 pagesElimination NeedsKhadija JaraNo ratings yet
- Knowledge Institute of Nursing: 1st Year G.N.MDocument8 pagesKnowledge Institute of Nursing: 1st Year G.N.MSANANo ratings yet
- Typhoid Fever: Infectious DiseaseDocument18 pagesTyphoid Fever: Infectious DiseaseSoumyadip PradhanNo ratings yet
- A Study To Assess The Effectiveness of Self Instructional Module On Knowledge Regarding Standard Precaution On Prevention of Infection Among Staff Nurses at Selected Hospital in Indore M.P.Document10 pagesA Study To Assess The Effectiveness of Self Instructional Module On Knowledge Regarding Standard Precaution On Prevention of Infection Among Staff Nurses at Selected Hospital in Indore M.P.International Journal of Innovative Science and Research TechnologyNo ratings yet
- Midwifery GNM 3 YearDocument1 pageMidwifery GNM 3 YearSimran GuptaNo ratings yet
- Wound DressingDocument18 pagesWound DressingBabita DhruwNo ratings yet
- 1757 Nursing Foundation Question BankDocument11 pages1757 Nursing Foundation Question BankSovon Samanta100% (1)
- Disease Transmission CycleDocument17 pagesDisease Transmission CycleReeycha ShresthaNo ratings yet
- Paper 1: Concept of Health and DiseaseDocument7 pagesPaper 1: Concept of Health and DiseaseYash LohiyaNo ratings yet
- BPT SyllabusDocument92 pagesBPT SyllabusRohit TalakeriNo ratings yet
- Pioneer Nursing College, Vadodara Master Rotation Plan For M.SC Nursing First YearDocument2 pagesPioneer Nursing College, Vadodara Master Rotation Plan For M.SC Nursing First YearKinjal VasavaNo ratings yet
- Doxovent M MedicalDocument38 pagesDoxovent M MedicalkurutalaNo ratings yet
- BCLSDocument25 pagesBCLSikram ullah khanNo ratings yet
- Third Year Basic B.SC (N) Question Bank: QP 1769 Subject: Child Health Nursing SR. NODocument19 pagesThird Year Basic B.SC (N) Question Bank: QP 1769 Subject: Child Health Nursing SR. NOSanal c SabuNo ratings yet
- PDF Cell Structure and Function Lesson PlanDocument6 pagesPDF Cell Structure and Function Lesson PlanDaniel Okazaki0% (1)
- ANPDocument3 pagesANPAdarsh NairNo ratings yet
- Government of Karnataka: para Medical BoardDocument40 pagesGovernment of Karnataka: para Medical BoardSrikutty DevuNo ratings yet
- BSC & PB BSC - New FormatDocument24 pagesBSC & PB BSC - New FormatNiranjan RajNo ratings yet
- PolioDocument71 pagesPolioMuhammad Ateeb100% (1)
- First Year B.Sc. Nursing Question Paper2010Document14 pagesFirst Year B.Sc. Nursing Question Paper2010Biju Antony90% (10)
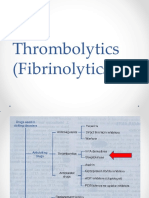
- Thrombolytics (Fibrinolytics)Document14 pagesThrombolytics (Fibrinolytics)J lodhiNo ratings yet
- Golden Point For PediatricsDocument19 pagesGolden Point For PediatricsOmprakash SainiNo ratings yet
- TyphoidDocument26 pagesTyphoidLiya Mary ThomasNo ratings yet
- Subject Plan B.SC Nursing 1 Year: MicrobiologyDocument2 pagesSubject Plan B.SC Nursing 1 Year: MicrobiologySandeep KumarNo ratings yet
- Syllabus Auxiliary Nurse and Midwives: Indian Nursing CouncilDocument76 pagesSyllabus Auxiliary Nurse and Midwives: Indian Nursing CouncilDIVYA PATELNo ratings yet
- ANAMEIA PPT BY SandeepDocument32 pagesANAMEIA PPT BY SandeepSandeep ChakravarthyNo ratings yet
- Renal CancerDocument34 pagesRenal CancerArya100% (1)
- Syllabus For BscnurDocument2 pagesSyllabus For BscnurAnil KumarNo ratings yet
- B.SC Nursing-2018-Question Papers-First Year-Microbiology FR PDFDocument1 pageB.SC Nursing-2018-Question Papers-First Year-Microbiology FR PDFSwapnil satputeNo ratings yet
- PMTCTDocument26 pagesPMTCTMaxwell C Jay KafwaniNo ratings yet
- Dissertation Submitted To The DR - Ram Manohar Lohia Awadh University AyodhyaDocument23 pagesDissertation Submitted To The DR - Ram Manohar Lohia Awadh University AyodhyaavnishNo ratings yet
- Principles of Disease Control and PreventionDocument13 pagesPrinciples of Disease Control and PreventionAYO NELSON0% (1)
- A Descriptive Study To Assess The Level of Anxiety Among B.Sc. Nursing 1st Year Students Regarding Exposure To Hospital Environment in Selected College of Nursing at Varanasi, IndiaDocument3 pagesA Descriptive Study To Assess The Level of Anxiety Among B.Sc. Nursing 1st Year Students Regarding Exposure To Hospital Environment in Selected College of Nursing at Varanasi, IndiaEditor IJTSRDNo ratings yet
- PMDCDocument35 pagesPMDCFarrukh Ali KhanNo ratings yet
- First Year B.Sc. Nursing Question Paper 2006Document8 pagesFirst Year B.Sc. Nursing Question Paper 2006Biju AntonyNo ratings yet
- Diarrhea: ChildrenDocument16 pagesDiarrhea: ChildrenEmmi Valentina PardedeNo ratings yet
- BMW Management - (AMENDMENT) Rules 2018Document19 pagesBMW Management - (AMENDMENT) Rules 2018Aruna ChezhianNo ratings yet
- International Journal of Trend in Scientific Research and Development (IJTSRD)Document4 pagesInternational Journal of Trend in Scientific Research and Development (IJTSRD)Editor IJTSRDNo ratings yet
- Ventilator Associated EventDocument25 pagesVentilator Associated EventAisa Jensen LeeNo ratings yet
- Paediatric 2005 - 2022Document30 pagesPaediatric 2005 - 2022melbha rexNo ratings yet
- Birth AsphyxiaDocument5 pagesBirth Asphyxiacompudoc11No ratings yet
- BioChemistry Syllabus and MQPs 08012018Document33 pagesBioChemistry Syllabus and MQPs 08012018rupaNo ratings yet
- National Vector Borne Disease Control ProgrammeDocument100 pagesNational Vector Borne Disease Control ProgrammeThe ThemerNo ratings yet
- NHP 1Document46 pagesNHP 1A J FathimaNo ratings yet
- National Vector Borne Disease Control Programme Malaria, Dengue, Chikungunya, Kala Azar and JEDocument31 pagesNational Vector Borne Disease Control Programme Malaria, Dengue, Chikungunya, Kala Azar and JEArushiNo ratings yet
- RMNCHDocument50 pagesRMNCHBEISAL BABY PNo ratings yet
- Old AgeDocument58 pagesOld AgeBEISAL BABY P100% (1)
- NCDDocument120 pagesNCDBEISAL BABY PNo ratings yet
- International QuarantineDocument72 pagesInternational QuarantineBEISAL BABY PNo ratings yet
- Lesson 3 Computing The Mean of A Discrete Probability DistributionDocument9 pagesLesson 3 Computing The Mean of A Discrete Probability DistributionYuan Daryle Fate HermosoNo ratings yet
- Ea 4 18 Inf Rev00 June 2010 RevDocument15 pagesEa 4 18 Inf Rev00 June 2010 RevBrandon EricksonNo ratings yet
- Pathmanabhan Al Nalliannen & Ors V Public PDocument38 pagesPathmanabhan Al Nalliannen & Ors V Public PNor Azilawati Muhd Al-AminuddinNo ratings yet
- Chapter 7 Consumer Learning: Consumer Behavior, 10e (Schiffman/Kanuk)Document34 pagesChapter 7 Consumer Learning: Consumer Behavior, 10e (Schiffman/Kanuk)shubham kumarNo ratings yet
- 1 Corinthians Part 2 Lesson #12 Chapter 12:1-11Document5 pages1 Corinthians Part 2 Lesson #12 Chapter 12:1-11A Firm Foundation Bible Studies at Calvary Bible Chruch, Burbank, CANo ratings yet
- RahimDocument3 pagesRahimPalak PathakNo ratings yet
- Production MethodsDocument2 pagesProduction Methodsabrar mahir SahilNo ratings yet
- Module 4D Concepts On Growth and DevelopmentDocument118 pagesModule 4D Concepts On Growth and DevelopmentKristil ChavezNo ratings yet
- Sermon 3Document5 pagesSermon 3Clarry GruyalNo ratings yet
- Flexible DuctDocument6 pagesFlexible DuctKiran patelNo ratings yet
- Lavendia Portfolio PR2 ABM12 4Document28 pagesLavendia Portfolio PR2 ABM12 4PresydenteNo ratings yet
- UntitledDocument1 pageUntitledErwinNo ratings yet
- Brent Kalar - The Demands of Taste in Kant's Aesthetics (Continuum Studies in Philosophy) (2006) PDFDocument189 pagesBrent Kalar - The Demands of Taste in Kant's Aesthetics (Continuum Studies in Philosophy) (2006) PDFPatricia Silveira PenhaNo ratings yet
- HCIA-Transmission Training Material V2.0Document547 pagesHCIA-Transmission Training Material V2.0Ahmed ElseliniNo ratings yet
- Chemistry PG 2015 Admn On05sept2015Document96 pagesChemistry PG 2015 Admn On05sept2015ZiyadNo ratings yet
- Lab 4: Handout Molecular Dynamics.: Recommended That You Read This LinkDocument22 pagesLab 4: Handout Molecular Dynamics.: Recommended That You Read This LinkshadrawsNo ratings yet
- The Renaissance ArchitectureDocument18 pagesThe Renaissance ArchitectureRazvan BataiosuNo ratings yet
- Thesis Proposal - ZelalemDocument43 pagesThesis Proposal - ZelalemMelkamu DemewezNo ratings yet
- Venturi Scrubber PerformanceDocument5 pagesVenturi Scrubber PerformanceJorge Joe Infante Santa CruzNo ratings yet
- Business English Negotiating Phrases Error Correction Pairwork PDFDocument6 pagesBusiness English Negotiating Phrases Error Correction Pairwork PDFEleniDesliNo ratings yet
- Exercise 2.6Document4 pagesExercise 2.6mohitgaba19No ratings yet
- MS07 Combined PDFDocument322 pagesMS07 Combined PDFSarin John SkariaNo ratings yet
- Lte MenaDocument8 pagesLte MenaPrassy PrasNo ratings yet
- 06 08 DCF Quiz Questions Basic PDFDocument22 pages06 08 DCF Quiz Questions Basic PDFVarun AgarwalNo ratings yet
- Motion Modifying The Freeze of AssetsDocument4 pagesMotion Modifying The Freeze of AssetsThe Daily SentinelNo ratings yet