Download as pptx, pdf, or txt
You might also like
- Caraka-Samhita - Eng. Vol. 1Document582 pagesCaraka-Samhita - Eng. Vol. 1calatorulfaradrum84% (70)
- Republican Challenge Against Mail Ballot LawDocument18 pagesRepublican Challenge Against Mail Ballot LawJessica HillNo ratings yet
- 02 - CONFERO Service Manuals PDFDocument1,719 pages02 - CONFERO Service Manuals PDFLamro TambaNo ratings yet
- GonorrheaDocument22 pagesGonorrheaSharah Londonio100% (1)
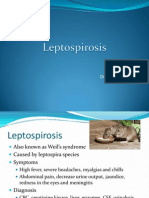
- LeptospirosisDocument9 pagesLeptospirosisDeepu VijayaBhanuNo ratings yet
- Behaviorally Anchored Rating ScalesDocument5 pagesBehaviorally Anchored Rating ScalesAarti Bhoria100% (2)
- QCVN 08-2008 BTNMT National Technical Regulation On Surface Water QualityDocument9 pagesQCVN 08-2008 BTNMT National Technical Regulation On Surface Water QualityvxzvzxvzvNo ratings yet
- Infectious DiseasesDocument65 pagesInfectious DiseasesFathimah UswahNo ratings yet
- Common Communicable DiseasesDocument213 pagesCommon Communicable Diseasesɹǝʍdןnos100% (25)
- Lecture Parasites in Immunocompromised PatientDocument50 pagesLecture Parasites in Immunocompromised PatientalgutNo ratings yet
- SchistosomiasisDocument5 pagesSchistosomiasisArifin AyobNo ratings yet
- Echinococcosis AsiyaDocument20 pagesEchinococcosis AsiyaBiswadeepan AcharyaNo ratings yet
- Systemic Infections From GiDocument10 pagesSystemic Infections From GiJake MillerNo ratings yet
- Communicable DiseasesDocument162 pagesCommunicable DiseasesCarlo VigoNo ratings yet
- 03 AmoebiasisDocument42 pages03 AmoebiasisKing IvyNo ratings yet
- Leptospirosis: Nurul Hidayu - Nashriq Aiman - Audi AdibahDocument28 pagesLeptospirosis: Nurul Hidayu - Nashriq Aiman - Audi AdibahAkshay D'souzaNo ratings yet
- Clinical ManifestationDocument6 pagesClinical ManifestationKrystal Jane SalinasNo ratings yet
- Enterotoxemia, Anaerobic Dysentery, Bradsot, Botulism and NecrobacteriosisDocument17 pagesEnterotoxemia, Anaerobic Dysentery, Bradsot, Botulism and NecrobacteriosisNajafova SuadaNo ratings yet
- Flagellates-2 by DR Gallardo: - MetronidazoleDocument7 pagesFlagellates-2 by DR Gallardo: - MetronidazoleJayricDepalobosNo ratings yet
- Typhoid Fever,-WPS OfficeDocument5 pagesTyphoid Fever,-WPS OfficeElvisNo ratings yet
- Project IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Document36 pagesProject IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Catherine MetraNo ratings yet
- Communicable DiseasesDocument161 pagesCommunicable DiseasesNader Smadi95% (20)
- Commmon Communcable Diseases Affecting The Gastointestinal System Final-1Document113 pagesCommmon Communcable Diseases Affecting The Gastointestinal System Final-1fulolorenzNo ratings yet
- Project IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Document38 pagesProject IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Catherine MetraNo ratings yet
- Alteration in Inflammatory and Immunologic Response 2012Document22 pagesAlteration in Inflammatory and Immunologic Response 2012Pamela BagabaldoNo ratings yet
- ASCARSISDocument39 pagesASCARSISkajal thakurNo ratings yet
- OtopDocument96 pagesOtopJayzle SaguisiNo ratings yet
- Communicable DiseasesDocument101 pagesCommunicable DiseasesKira100% (4)
- Oral and Intestinal FlagellatesDocument3 pagesOral and Intestinal FlagellatesChristine BuenNo ratings yet
- Enteric FeverDocument7 pagesEnteric FeverkudzaimuregidubeNo ratings yet
- Schistosomiasis, Group B Presentation-1Document22 pagesSchistosomiasis, Group B Presentation-1Princewill SeiyefaNo ratings yet
- BY:-Shalini Joshi M.SC NURSING Ist Year S.C.O.N. DehradunDocument52 pagesBY:-Shalini Joshi M.SC NURSING Ist Year S.C.O.N. DehradunshravaniNo ratings yet
- General Parasitology L4Document12 pagesGeneral Parasitology L4kayse abtidoonNo ratings yet
- SchistosomiasisDocument5 pagesSchistosomiasisBryan TarrobalNo ratings yet
- Purperal InfectionsDocument69 pagesPurperal InfectionsBeulah DasariNo ratings yet
- +ascariasisDocument16 pages+ascariasisDr. SAMNo ratings yet
- SchistosomiasisDocument5 pagesSchistosomiasisJane GarciaNo ratings yet
- Large Ruminant DiseasesDocument96 pagesLarge Ruminant DiseasesJayson BasiagNo ratings yet
- Division of Infectious and Tropical Diseases, Department of Internal Medicine, University of Sumatera Utara/ Adam Malik Hospital, Medan, IndonesiaDocument18 pagesDivision of Infectious and Tropical Diseases, Department of Internal Medicine, University of Sumatera Utara/ Adam Malik Hospital, Medan, IndonesiaIndah PutriNo ratings yet
- Gastroenteritis: Saima Alam AfridiDocument23 pagesGastroenteritis: Saima Alam AfridiMahnoor ParvezNo ratings yet
- Catarrhal Stage: 1-2 Weeks Coryza, FeverDocument45 pagesCatarrhal Stage: 1-2 Weeks Coryza, FeverAbigail BrillantesNo ratings yet
- STDDocument49 pagesSTDArnzz AgbulosNo ratings yet
- Enterobacteriaceae: Dr. BetsyDocument36 pagesEnterobacteriaceae: Dr. BetsySoham BanikNo ratings yet
- Synonyms Causative Agents Incubatiob Period Mode of Transmission Signs and Symptoms Period of Communicability Diagnostic Test Medical Management Nursing Management ComplicationsDocument13 pagesSynonyms Causative Agents Incubatiob Period Mode of Transmission Signs and Symptoms Period of Communicability Diagnostic Test Medical Management Nursing Management ComplicationsYnah DominiqueNo ratings yet
- Kuliah Cestode & Trematode (Hand-Out)Document13 pagesKuliah Cestode & Trematode (Hand-Out)made yogaNo ratings yet
- Exercise 7 ParasitDocument6 pagesExercise 7 ParasitIvanNo ratings yet
- Communicable DiseasesDocument6 pagesCommunicable DiseasesLory LynNo ratings yet
- Diphtheria HandoutsDocument8 pagesDiphtheria HandoutsRachelle Mae DimayugaNo ratings yet
- Foot and Mouth DiseasesDocument9 pagesFoot and Mouth Diseaseseutamène ramziNo ratings yet
- Hookworm Diseases: (Ancylostomiasis /Miner'S Disease/Egyptian Chlorisis)Document21 pagesHookworm Diseases: (Ancylostomiasis /Miner'S Disease/Egyptian Chlorisis)Mel Izhra N. Margate100% (1)
- Microbology of Urinary Track Infection Kel 1Document29 pagesMicrobology of Urinary Track Infection Kel 1Alfred L ToruanNo ratings yet
- Animal DiseasesDocument27 pagesAnimal DiseasessandraespinosaNo ratings yet
- Typhoid FeverDocument46 pagesTyphoid Feverdeskichinta50% (2)
- Mikroorganisme Penyebab Infeksi Pada Sistem Reproduksi2003Document132 pagesMikroorganisme Penyebab Infeksi Pada Sistem Reproduksi2003anitacharisNo ratings yet
- Case Presentation: Ascariasis: Mrs. Lailanie Evangelista DotimasDocument10 pagesCase Presentation: Ascariasis: Mrs. Lailanie Evangelista DotimasRodelen MarañoNo ratings yet
- Co, Kenneth Cua, Irene de Leon, TimothyDocument10 pagesCo, Kenneth Cua, Irene de Leon, TimothyIrene Bodegon CuaNo ratings yet
- Typhoid Fever-WPS OfficeDocument1 pageTyphoid Fever-WPS OfficecimdesadesuNo ratings yet
- Puerperal SepsisDocument34 pagesPuerperal SepsisSanthosh.S.UNo ratings yet
- Leptospirosis: Divisi Penyakit Tropik Dan Infeksi Departemen Penyakit Dalam FK USU/RSU HAMDocument20 pagesLeptospirosis: Divisi Penyakit Tropik Dan Infeksi Departemen Penyakit Dalam FK USU/RSU HAMJoice RumondangNo ratings yet
- Health Management PracticesDocument15 pagesHealth Management PracticesJessa Mae Paste AlzagaNo ratings yet
- GI Protozoal & Infections Caused by HelminthsDocument39 pagesGI Protozoal & Infections Caused by HelminthsSHIHAB UDDIN KAZINo ratings yet
- Communicable Disease Review MaterialDocument43 pagesCommunicable Disease Review Materialrceponelas1127No ratings yet
- 911 Pigeon Disease & Treatment Protocols!From Everand911 Pigeon Disease & Treatment Protocols!Rating: 4 out of 5 stars4/5 (1)
- Fascination of Diet TrendsDocument1 pageFascination of Diet Trendsyuuki konnoNo ratings yet
- Cardiac Arrest: April B. Perez, RN, Man, PHD, FpchaDocument50 pagesCardiac Arrest: April B. Perez, RN, Man, PHD, Fpchayuuki konnoNo ratings yet
- Understanding The Importance of A Mother's Role in A Child's LifeDocument1 pageUnderstanding The Importance of A Mother's Role in A Child's Lifeyuuki konnoNo ratings yet
- Antibiotic Inefficacy Against Viral InfectionDocument1 pageAntibiotic Inefficacy Against Viral Infectionyuuki konnoNo ratings yet
- 7ethical Decision Making - StudsDocument26 pages7ethical Decision Making - Studsyuuki konnoNo ratings yet
- Most Impactful Scientific Breakthrough of The Last 300 YearsDocument1 pageMost Impactful Scientific Breakthrough of The Last 300 Yearsyuuki konnoNo ratings yet
- 100 Important Terminologies in Medical Surgical NursingDocument4 pages100 Important Terminologies in Medical Surgical Nursingyuuki konnoNo ratings yet
- Effects of Global Warming in The Past 10 YearsDocument1 pageEffects of Global Warming in The Past 10 Yearsyuuki konnoNo ratings yet
- #1 Way Social Media MarketingDocument1 page#1 Way Social Media Marketingyuuki konnoNo ratings yet
- Antibiotic MisuseDocument1 pageAntibiotic Misuseyuuki konnoNo ratings yet
- NCM 119 Module (1) - 1Document134 pagesNCM 119 Module (1) - 1yuuki konnoNo ratings yet
- Blood TransfusionDocument1 pageBlood Transfusionyuuki konnoNo ratings yet
- 7.2 PlanningDocument44 pages7.2 Planningyuuki konnoNo ratings yet
- 2chain of DiseaseDocument43 pages2chain of Diseaseyuuki konno100% (1)
- Family NCP FormDocument2 pagesFamily NCP Formyuuki konnoNo ratings yet
- Elements and Priciples of The ArtsDocument79 pagesElements and Priciples of The Artsyuuki konnoNo ratings yet
- Chapter - 008 PHARMA PABDocument19 pagesChapter - 008 PHARMA PAByuuki konnoNo ratings yet
- Chapter - 005 PEDIATRIC COSIDERATIONS With Video PresentatioDocument15 pagesChapter - 005 PEDIATRIC COSIDERATIONS With Video Presentatioyuuki konnoNo ratings yet
- Nutrition Care Process: Maria Sheila A. Clanor RN, MANDocument75 pagesNutrition Care Process: Maria Sheila A. Clanor RN, MANyuuki konnoNo ratings yet
- NCM 120 Week 12 Transcultural22Document37 pagesNCM 120 Week 12 Transcultural22yuuki konnoNo ratings yet
- NCM-107-Perineal Care Prior and AfterDocument24 pagesNCM-107-Perineal Care Prior and Afteryuuki konnoNo ratings yet
- Postpartum - Physiology and NSG Care 15Document33 pagesPostpartum - Physiology and NSG Care 15yuuki konnoNo ratings yet
- NCM 107 Growth and Development NEW20 1Document100 pagesNCM 107 Growth and Development NEW20 1yuuki konnoNo ratings yet
- 8food - Borne Diseases - For StudsDocument30 pages8food - Borne Diseases - For Studsyuuki konnoNo ratings yet
- NCM 107 Apgar, Ballard20Document50 pagesNCM 107 Apgar, Ballard20yuuki konnoNo ratings yet
- NCM-107-Medication Adm - SF20Document27 pagesNCM-107-Medication Adm - SF20yuuki konnoNo ratings yet
- Breast Feeding Autosaved SDocument48 pagesBreast Feeding Autosaved Syuuki konnoNo ratings yet
- Module 2 CHNDocument20 pagesModule 2 CHNyuuki konnoNo ratings yet
- 4oral-Fecal DsesDocument153 pages4oral-Fecal Dsesyuuki konnoNo ratings yet
- Basic Swimming Lecture 1Document34 pagesBasic Swimming Lecture 1yuuki konnoNo ratings yet
- Maur MeyerDocument488 pagesMaur MeyerItachi KunNo ratings yet
- Victorian Compromise and Literary Movements PDFDocument2 pagesVictorian Compromise and Literary Movements PDFChuii MuiiNo ratings yet
- Parent'S/Guardian Consent and Waiver Form: Batangas State UniversityDocument1 pageParent'S/Guardian Consent and Waiver Form: Batangas State UniversityGillian Lei Carandang SacisNo ratings yet
- Janet Museveni School Reopening StatementDocument21 pagesJanet Museveni School Reopening StatementThe Independent MagazineNo ratings yet
- Shiva RatriDocument14 pagesShiva RatriTaoshobuddha100% (1)
- Cover Letter Health Care Assistant No ExperienceDocument6 pagesCover Letter Health Care Assistant No Experiencewisaj0jat0l3100% (2)
- Jozef KronerDocument2 pagesJozef KronerAryan KhannaNo ratings yet
- Life Vision Int Plus Comm Worksheet U5Document1 pageLife Vision Int Plus Comm Worksheet U5Bert VannNo ratings yet
- Steel Wire Ropes For Traction Elevators: Part Three: Continuing Education: TechnologyDocument14 pagesSteel Wire Ropes For Traction Elevators: Part Three: Continuing Education: TechnologyHakim BgNo ratings yet
- Importance of IqDocument4 pagesImportance of Iqmark ignacioNo ratings yet
- Thirumurai 2Document188 pagesThirumurai 2thegodkannanNo ratings yet
- Electromagnatic InductionDocument1 pageElectromagnatic InductionMahes JeyNo ratings yet
- The Earth and Life ScienceDocument4 pagesThe Earth and Life ScienceJaycee AlfaroNo ratings yet
- Peru - July20.16.m PonenciasDocument230 pagesPeru - July20.16.m PonenciasedisonNo ratings yet
- Crim 01Document88 pagesCrim 01Marian Jewel VillanuevaNo ratings yet
- Mechanics of Deformable Bodies: Mapúa Institute of TechnologyDocument16 pagesMechanics of Deformable Bodies: Mapúa Institute of TechnologyAhsan AliNo ratings yet
- Occupational Therapy's Role in Post Concussion Management: Aimil Parmelee, MOT, OTR/L Marlaina Montgomery, MOT, OTR/LDocument27 pagesOccupational Therapy's Role in Post Concussion Management: Aimil Parmelee, MOT, OTR/L Marlaina Montgomery, MOT, OTR/Lsidney drecotteNo ratings yet
- Geisum Oil Field: Structure of Geisum ConcessionDocument1 pageGeisum Oil Field: Structure of Geisum ConcessionAhmed FoudaNo ratings yet
- 1Document14 pages1netsa_marNo ratings yet
- Fungal NutritionDocument3 pagesFungal NutritionArtemishaMtzNo ratings yet
- 6DVH 3190ubDocument55 pages6DVH 3190ubakshayjauhari100% (1)
- Foreign Direct Investment in Nepal: Social Inquiry: Journal of Social Science ResearchDocument20 pagesForeign Direct Investment in Nepal: Social Inquiry: Journal of Social Science Researchjames smithNo ratings yet
- Lexical Concepts, Cognitive Models and Meaning-Construction: Vyvyan EvansDocument44 pagesLexical Concepts, Cognitive Models and Meaning-Construction: Vyvyan EvansДарья БелокрыльцеваNo ratings yet
- (Download PDF) Fundamentals of Cost Accounting 7Th Edition William Lanen Full Chapter PDFDocument69 pages(Download PDF) Fundamentals of Cost Accounting 7Th Edition William Lanen Full Chapter PDFkqirajbelqis100% (7)
- Historein11 (2011)Document242 pagesHistorein11 (2011)Dimitris Plantzos100% (1)