Download as pptx, pdf, or txt
You might also like
- No Gallbladder Diet Cookbook: Discover Flavorful and Nourishing Recipes to Revitalize Your Metabolism After Gallbladder Surgery [COLOR EDITION]From EverandNo Gallbladder Diet Cookbook: Discover Flavorful and Nourishing Recipes to Revitalize Your Metabolism After Gallbladder Surgery [COLOR EDITION]Rating: 5 out of 5 stars5/5 (26)
- Hypoglycemia Treatment ProtocolDocument1 pageHypoglycemia Treatment ProtocolCherryBeeNo ratings yet
- 209-Hematology Review - Case StudiesDocument129 pages209-Hematology Review - Case StudiesKhalid Khalidi100% (2)
- CholeraDocument11 pagesCholeraElaine ZafeNo ratings yet
- CHN Food and WaterDocument4 pagesCHN Food and WatertimmybunsenNo ratings yet
- Report On AmoebiasisDocument36 pagesReport On Amoebiasisrhimineecat71No ratings yet
- CholeraDocument24 pagesCholeraLavanya Sivakumar100% (1)
- Capillaria Philippinensis (Paracapillaria Philippinensis)Document44 pagesCapillaria Philippinensis (Paracapillaria Philippinensis)Madhu MithaNo ratings yet
- Leptospirosis Discussion and CPGDocument66 pagesLeptospirosis Discussion and CPGdoc_geloNo ratings yet
- Cholera Mi Lecture MDocument35 pagesCholera Mi Lecture MJohnson OlawaleNo ratings yet
- Junior Intern Review - Oral Revalida 2016Document170 pagesJunior Intern Review - Oral Revalida 2016Cyrus ZalameaNo ratings yet
- Typhoid Fever: ProfessorDocument48 pagesTyphoid Fever: ProfessormanibharathiNo ratings yet
- Urine Analysis FinalDocument112 pagesUrine Analysis FinalNischita JayarajNo ratings yet
- Vibrio Campy and Hpylori Notes MBCHBDocument35 pagesVibrio Campy and Hpylori Notes MBCHBMuthianiNo ratings yet
- Laboratory Safety: Ann Fatima G. Quindao, RMT, LPT, MPHDocument43 pagesLaboratory Safety: Ann Fatima G. Quindao, RMT, LPT, MPHJanelou PalenNo ratings yet
- AMOEBIASISDocument31 pagesAMOEBIASISpriyagerard100% (1)
- Diagnostic Microbiology: CampylobacterDocument25 pagesDiagnostic Microbiology: Campylobacteranon_914901469No ratings yet
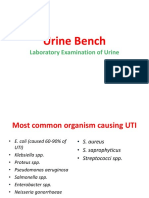
- UTIDocument57 pagesUTIGireesh NagaruruNo ratings yet
- AmoebiasisDocument29 pagesAmoebiasisFatima murtadaNo ratings yet
- Cholera: Alyssa P. BagaporoDocument39 pagesCholera: Alyssa P. BagaporoDimple BagaporoNo ratings yet
- K1. Elektif ParasitDocument34 pagesK1. Elektif ParasitUu'ayu UnyuNo ratings yet
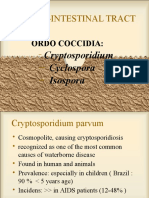
- GIT Coccidia 13Document18 pagesGIT Coccidia 13Annisaa FitrianiNo ratings yet
- Infcetions Intestinal Protozoal InfectionsDocument40 pagesInfcetions Intestinal Protozoal InfectionsDr.P.NatarajanNo ratings yet
- NematodesDocument110 pagesNematodesRussel Bob BorromeoNo ratings yet
- Clinical Microscopy - MTDocument200 pagesClinical Microscopy - MTJihrus Mendoza100% (1)
- 4 - Urine BenchDocument37 pages4 - Urine BenchChiizu iraNo ratings yet
- UrinalysisDocument34 pagesUrinalysischristian gNo ratings yet
- SESSION 13-Diarrhea DiseaseDocument29 pagesSESSION 13-Diarrhea Diseasegbunyara100No ratings yet
- Investigation of AbdomenDocument72 pagesInvestigation of Abdomenreconnaissante28No ratings yet
- Stool ExaminationDocument108 pagesStool ExaminationBig ZeroNo ratings yet
- FECALYSISDocument43 pagesFECALYSISKen LaguiabNo ratings yet
- 3.4 Helicobacter PyloriDocument25 pages3.4 Helicobacter PyloriWong ShuanNo ratings yet
- Intestinal Coccidian ParasitesDocument23 pagesIntestinal Coccidian ParasitesABC100% (1)
- Hepatitis ADocument17 pagesHepatitis Ajosh0797677004No ratings yet
- Ruminal Acidosis/Rumen Overload For Vet. Students /ali SadiekDocument25 pagesRuminal Acidosis/Rumen Overload For Vet. Students /ali SadiekAli H. Sadiek أ.د. علي حسن صديق100% (2)
- Enterobacteriaceae - Non Lactose Fermenters - La 2020Document111 pagesEnterobacteriaceae - Non Lactose Fermenters - La 2020GiselleNo ratings yet
- Diagnostic Approach To Malabsorbtion: Suspecting Presence of Malabsorption-History, Physical ExaminationDocument58 pagesDiagnostic Approach To Malabsorbtion: Suspecting Presence of Malabsorption-History, Physical Examinationsanjay kumarNo ratings yet
- Communicable and Vector Bone Diseases1) - 1Document175 pagesCommunicable and Vector Bone Diseases1) - 1staceyatienoomaNo ratings yet
- LAB 4 - StreptococcusDocument31 pagesLAB 4 - Streptococcussajad abasNo ratings yet
- T HypoidDocument22 pagesT HypoidDeddy ShangrelaNo ratings yet
- Anaerobes of Clinical ImportanceDocument73 pagesAnaerobes of Clinical ImportanceMaria ClaraNo ratings yet
- All Infectious Diseases-2Document67 pagesAll Infectious Diseases-2Samson Oroma OnginjoNo ratings yet
- ShigellosisDocument39 pagesShigellosisWai Kwong ChiuNo ratings yet
- Unit 4 Inflammatory Bowel DiseasesDocument55 pagesUnit 4 Inflammatory Bowel DiseasesdhanashriNo ratings yet
- Chemical TestsDocument51 pagesChemical TestsNicole Jane RobesNo ratings yet
- Parasitos Oportunistas: Catalina Tovar Acero Msc. Infecciones Y Salud en El TropicalDocument22 pagesParasitos Oportunistas: Catalina Tovar Acero Msc. Infecciones Y Salud en El TropicalAndrés ArrietaNo ratings yet
- GIARDIASISDocument32 pagesGIARDIASISDathan EdwardNo ratings yet
- ANAEROBES - Narayan Parajul - MMIHS III RD YearDocument42 pagesANAEROBES - Narayan Parajul - MMIHS III RD YearRajkishor YadavNo ratings yet
- Diarrhea: Dr. Haifa Yagoub OsmanDocument23 pagesDiarrhea: Dr. Haifa Yagoub OsmanAlex SamNo ratings yet
- Dr. Isna Git B Coli 13Document12 pagesDr. Isna Git B Coli 13Elisa Fata Marokeh TedadEspochachaNo ratings yet
- CholeraDocument4 pagesCholeraBeth AvelinoNo ratings yet
- Amphistomiasis, SchistosomiasisDocument15 pagesAmphistomiasis, Schistosomiasisdharmachakra ComNo ratings yet
- Disentri Amoeba TUTORDocument26 pagesDisentri Amoeba TUTORShameer Mohamed AljabarNo ratings yet
- Acute DiarrheaDocument14 pagesAcute DiarrheaSbahat FatimaNo ratings yet
- DiarrheaDocument24 pagesDiarrheaash ashNo ratings yet
- Acute Gastroenteritis in ChildrenDocument39 pagesAcute Gastroenteritis in ChildrenIra Mikkaella GenobisNo ratings yet
- Screening Stools For PathogensDocument14 pagesScreening Stools For PathogensJauharotun NafisahNo ratings yet
- Urinalysis 1: Mr. Arian Ray E. MalintadDocument55 pagesUrinalysis 1: Mr. Arian Ray E. MalintadAbraham DemeterioNo ratings yet
- Microscopic ExaminationDocument72 pagesMicroscopic ExaminationbubblyeivinejNo ratings yet
- Urine Specimen Collection: Ms. Sneha SehrawatDocument36 pagesUrine Specimen Collection: Ms. Sneha SehrawatRajaNo ratings yet
- Pulmonary Diseases-CopdDocument14 pagesPulmonary Diseases-CopdSamyuktha SivakumarNo ratings yet
- Fatty Acid Metabolism Daniel LimDocument4 pagesFatty Acid Metabolism Daniel LimSamyuktha SivakumarNo ratings yet
- FSD EgmoreDocument10 pagesFSD EgmoreSamyuktha SivakumarNo ratings yet
- Microflora of SoilDocument12 pagesMicroflora of SoilSamyuktha SivakumarNo ratings yet
- Industrially Imp OrgDocument13 pagesIndustrially Imp OrgSamyuktha SivakumarNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanRaphael Reyes Enriquez100% (1)
- Laporan Peringkat Diagnosa 19102019-122829 P3273050101Document1 pageLaporan Peringkat Diagnosa 19102019-122829 P3273050101Ferry FirmansyahNo ratings yet
- Fundamentals Exam 2Document8 pagesFundamentals Exam 2Larissa DickersonNo ratings yet
- Bajaj Allianz Silver HealthDocument18 pagesBajaj Allianz Silver Healthvijay.pandey373No ratings yet
- Unusual Presentation of Pancreatic Insulinoma:a Case ReportDocument5 pagesUnusual Presentation of Pancreatic Insulinoma:a Case ReportIJAR JOURNALNo ratings yet
- AntacidDocument6 pagesAntacidtushar devmurarNo ratings yet
- NCLEX NotesDocument11 pagesNCLEX NotesRuth Belflower100% (2)
- Celiacdisease PathfinderDocument8 pagesCeliacdisease Pathfinderapi-446834058No ratings yet
- Lecture 5 CestodesDocument6 pagesLecture 5 CestodesBea SamonteNo ratings yet
- Atresia EsofagusDocument15 pagesAtresia EsofagusAndri Feisal NasutionNo ratings yet
- How Low Is Safe? The Frontier of Very Low ( 30 MG/DL) LDL CholesterolDocument16 pagesHow Low Is Safe? The Frontier of Very Low ( 30 MG/DL) LDL Cholesterolpitiwararom rachtipatNo ratings yet
- AEFI Surveillance and Response Operational Guidelines 2015Document204 pagesAEFI Surveillance and Response Operational Guidelines 2015anunad100% (1)
- Patient Response: Self IntroductionDocument3 pagesPatient Response: Self IntroductionMercy Anne EcatNo ratings yet
- Hematology Nursing Handout PDFDocument12 pagesHematology Nursing Handout PDFShanine Alexia Cordovez100% (1)
- Acute Respiratory Distress Syndrome - PathophysiologyDocument5 pagesAcute Respiratory Distress Syndrome - PathophysiologyJoann67% (3)
- Challenges in Care of Adult CF Patients - The Specialist Cystic Fibrosis TeamDocument4 pagesChallenges in Care of Adult CF Patients - The Specialist Cystic Fibrosis TeamjuniorebindaNo ratings yet
- Seminar 4Document49 pagesSeminar 4Yamuna SubramaniamNo ratings yet
- Interpretation On Pulmonary Function TestDocument105 pagesInterpretation On Pulmonary Function Testsalmamaged7619No ratings yet
- GI System and Its Disorders (Nurses Perspective)Document23 pagesGI System and Its Disorders (Nurses Perspective)aswathykrishnan73100% (3)
- Case Study - Final DraftDocument51 pagesCase Study - Final DraftMaeNo ratings yet
- GetPdf Cgi PDFDocument9 pagesGetPdf Cgi PDFAKNTAI002No ratings yet
- Movement DisordersDocument10 pagesMovement DisordersAli 10No ratings yet
- RDUK-Family-Report.pdfyfulllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllliuggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggDocument37 pagesRDUK-Family-Report.pdfyfulllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllliuggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggSamdarsh NirankariNo ratings yet
- Antibiotics As An Intracanal Medicament in EndodonticsDocument1 pageAntibiotics As An Intracanal Medicament in EndodonticsمعتزعليNo ratings yet
- Case Presentation: EclampsiaDocument44 pagesCase Presentation: Eclampsiamutiara sitepuNo ratings yet
- Ekspresi P40 Dan CK 5/6 Pada Diagnosis Sitologi Efusi Pleura Dengan Gambaran KeganasanDocument6 pagesEkspresi P40 Dan CK 5/6 Pada Diagnosis Sitologi Efusi Pleura Dengan Gambaran KeganasanEvrita Teny A.No ratings yet
- Peritonsillar Abscess (B.ing)Document13 pagesPeritonsillar Abscess (B.ing)oltavia yuniarNo ratings yet
- Fungal Infections: Alma E. Malilong, MD, FPSPDocument33 pagesFungal Infections: Alma E. Malilong, MD, FPSPQurrataini IbanezNo ratings yet
![No Gallbladder Diet Cookbook: Discover Flavorful and Nourishing Recipes to Revitalize Your Metabolism After Gallbladder Surgery [COLOR EDITION]](https://imgv2-2-f.scribdassets.com/img/word_document/591540228/149x198/6ba6cc3b38/1720371770?v=1)