
Covid19 Infection Prevention and Control
Covid19 Infection Prevention and Control
You might also like
- Guidance For Routine Immunization Services During COVID-19: - PageDocument14 pagesGuidance For Routine Immunization Services During COVID-19: - PagePrisma CahyaNo ratings yet
- Coronavirus Covid 19 Guidance On Use of Personal Protective Equipment Ppe in Non Inpatient Health Care Settings During The Covid 19 OutbreakDocument6 pagesCoronavirus Covid 19 Guidance On Use of Personal Protective Equipment Ppe in Non Inpatient Health Care Settings During The Covid 19 OutbreakGerlan Madrid MingoNo ratings yet
- Mask Use in The Context of COVID-19: Interim Guidance 1 December 2020Document22 pagesMask Use in The Context of COVID-19: Interim Guidance 1 December 2020ShahabNo ratings yet
- WHO 2019 Ncov IPC - Masks 2020.5 EngDocument22 pagesWHO 2019 Ncov IPC - Masks 2020.5 EngsilviaNo ratings yet
- Issues Related To Kidney Disease and HypertensionDocument12 pagesIssues Related To Kidney Disease and HypertensionCarlos Huaman ZevallosNo ratings yet
- EPP. Am. College, Surgeons.20.Document3 pagesEPP. Am. College, Surgeons.20.Mary RodriguezNo ratings yet
- Triage, Source Control and Additional Control Measures: IPC IPCDocument33 pagesTriage, Source Control and Additional Control Measures: IPC IPCPriya RanjanNo ratings yet
- 02a - PPE - Summary and Rationale For RecommendationsDocument2 pages02a - PPE - Summary and Rationale For RecommendationsMohammedNo ratings yet
- Coronavirus Covid 19 Guidelines For Infection Prevention and Control in Residential Care Facilities - 0Document11 pagesCoronavirus Covid 19 Guidelines For Infection Prevention and Control in Residential Care Facilities - 0Shenelle NashNo ratings yet
- Mask Use in The Context of COVID-19: Interim Guidance 1 December 2020Document25 pagesMask Use in The Context of COVID-19: Interim Guidance 1 December 2020Ziyad BaraNo ratings yet
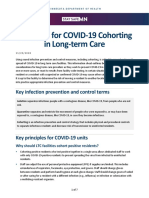
- Principles For COVID-19 Cohorting in Long-Term Care: Key Infection Prevention and Control TermsDocument7 pagesPrinciples For COVID-19 Cohorting in Long-Term Care: Key Infection Prevention and Control TermssimplyrosalynNo ratings yet
- Group 3 - NCM 119 Case Scenario - Bartolata-4ADocument6 pagesGroup 3 - NCM 119 Case Scenario - Bartolata-4AKeisha BartolataNo ratings yet
- IPC Guidelines For COVID 19Document15 pagesIPC Guidelines For COVID 19Henry OseiNo ratings yet
- IPC in HD ServicesDocument28 pagesIPC in HD ServicesseptianyganescyaNo ratings yet
- IPC GUIDELINE Version 2Document20 pagesIPC GUIDELINE Version 2Nrs KhalidNo ratings yet
- ASA Staff Safety For COVID-19: StatementDocument8 pagesASA Staff Safety For COVID-19: StatementAbidi HichemNo ratings yet
- COVID-19 Preparedness 14apr2020Document13 pagesCOVID-19 Preparedness 14apr2020Andre3893No ratings yet
- Guidance On The Use of Personal Protective Equipment Ppe in Hospitals During The Covid 19 OutbreakDocument9 pagesGuidance On The Use of Personal Protective Equipment Ppe in Hospitals During The Covid 19 OutbreakGerlan Madrid MingoNo ratings yet
- RevisedGuidelinesforDialysisofCOVID19Patients PDFDocument8 pagesRevisedGuidelinesforDialysisofCOVID19Patients PDFAmjadali ChoudhariNo ratings yet
- RevisedGuidelinesforDialysisofCOVID19Patients PDFDocument8 pagesRevisedGuidelinesforDialysisofCOVID19Patients PDFSaurav KumarNo ratings yet
- Presentation COVID-19 WHO enDocument12 pagesPresentation COVID-19 WHO enEtaferawNo ratings yet
- Suraj Clinical Management of COVID 19Document23 pagesSuraj Clinical Management of COVID 19H.M RathodNo ratings yet
- COVID 19 Outpatient DialysisDocument5 pagesCOVID 19 Outpatient DialysisTheala RadistaNo ratings yet
- Dr. Hendri - Early Warning System & PPEDocument106 pagesDr. Hendri - Early Warning System & PPEViniFortunataNo ratings yet
- Guideline Managing Critically IllDocument8 pagesGuideline Managing Critically Illmisfatrianoor10No ratings yet
- Tanzania - SOPs For Case Management and Infection Prevention and ControlDocument115 pagesTanzania - SOPs For Case Management and Infection Prevention and ControlXuan Nguyen100% (1)
- Guideline For Conservation of Respiratory Protection ResourcesDocument14 pagesGuideline For Conservation of Respiratory Protection ResourcesAMEU URGENCIASNo ratings yet
- ADA Managing COVID 19 Guide 25 March 2020Document6 pagesADA Managing COVID 19 Guide 25 March 2020Pepo BelovedNo ratings yet
- Update Who Recommendation On Covid-19 For Hospital: Setiawan Jati Laksono 10 April 2020Document34 pagesUpdate Who Recommendation On Covid-19 For Hospital: Setiawan Jati Laksono 10 April 2020Nadya FaradibaNo ratings yet
- COVID-19 PPE Training Presentation - Without Video - 6 MayDocument29 pagesCOVID-19 PPE Training Presentation - Without Video - 6 Maymeherul hasanNo ratings yet
- Phase 1 Tasks and QuestionsDocument8 pagesPhase 1 Tasks and QuestionsEmmanuel RumbaoaNo ratings yet
- Dr. Suraya's PPT - IPC COVID MX in Private Healthcare PDFDocument40 pagesDr. Suraya's PPT - IPC COVID MX in Private Healthcare PDFFrostz WongNo ratings yet
- Standard Operating ProcedureDocument15 pagesStandard Operating ProcedureAyman AliNo ratings yet
- Infection Control and Covid SafetyDocument41 pagesInfection Control and Covid SafetyAdeuga ADEKUOYENo ratings yet
- UHMS Guidelines - COVID-19 V4Document3 pagesUHMS Guidelines - COVID-19 V4Juan CruzNo ratings yet
- Australia Covid PpeDocument5 pagesAustralia Covid PpeAbidi HichemNo ratings yet
- Coronavirus Disease 2019 (COVID-19) - Infection Control in Health Care and Home Settings - UpToDateDocument40 pagesCoronavirus Disease 2019 (COVID-19) - Infection Control in Health Care and Home Settings - UpToDateFlorin StanciuNo ratings yet
- Assessment TechniquesDocument12 pagesAssessment TechniquesAeshel TabuzoNo ratings yet
- Approaches To The Management of Patients in Oral and Maxillofacial Surgery During COVID-19 PandemicDocument21 pagesApproaches To The Management of Patients in Oral and Maxillofacial Surgery During COVID-19 PandemicYahul MazfarNo ratings yet
- Annex 40 INTERIM GUIDELINES ON RESUSCITATION DURING COVID19 PANDEMICDocument15 pagesAnnex 40 INTERIM GUIDELINES ON RESUSCITATION DURING COVID19 PANDEMICAzran Shariman HasshimNo ratings yet
- Standard Operating Procedure For Handling of Corona Virus Disease (Covid-19) PatientsDocument6 pagesStandard Operating Procedure For Handling of Corona Virus Disease (Covid-19) PatientsHiJackNo ratings yet
- Infection Prevention CourseDocument73 pagesInfection Prevention Coursedakejay292No ratings yet
- Who 2019 Ncov Ipc Ppe Use 2020.3 EngDocument28 pagesWho 2019 Ncov Ipc Ppe Use 2020.3 EngKumanan1304No ratings yet
- Perioperative Considerstions in Urgent Surgical Care of Suspected and Confirmed COVID-19 Orthopaedic PatientsDocument23 pagesPerioperative Considerstions in Urgent Surgical Care of Suspected and Confirmed COVID-19 Orthopaedic PatientsDoctor's BettaNo ratings yet
- Handling Trauma and Burn PatientsDocument19 pagesHandling Trauma and Burn PatientsWhisky MiloNo ratings yet
- Interim Guidance Pediatric Patients March 27 2020Document4 pagesInterim Guidance Pediatric Patients March 27 2020Luis Alberto Anco CórdovaNo ratings yet
- dm2020 0202 PDFDocument6 pagesdm2020 0202 PDFcode4saleNo ratings yet
- SOP Triage Suspected CovidDocument29 pagesSOP Triage Suspected CovidRoy Tanda Anugrah SihotangNo ratings yet
- Universal Precautions Transmission Based PrecautionsDocument61 pagesUniversal Precautions Transmission Based PrecautionsShalamNo ratings yet
- COVID-19 Office Prep ChecklistDocument4 pagesCOVID-19 Office Prep ChecklistMohammad SahyouniNo ratings yet
- Clinical Management of COVID-19 Patients - v1Document18 pagesClinical Management of COVID-19 Patients - v1rohitNo ratings yet
- Document Can Be Found At:: /hcp/non-Us-Settings/overview/index - HTMLDocument25 pagesDocument Can Be Found At:: /hcp/non-Us-Settings/overview/index - HTMLMaqbool AlizaiNo ratings yet
- Lecture 13 IC Precautions and IsolationsDocument10 pagesLecture 13 IC Precautions and IsolationsTariq AzizNo ratings yet
- Respiratory Physiotherapy Guidelines For Managing Patients With Covid or of Unknown Covid Status 15nov21 - 0Document4 pagesRespiratory Physiotherapy Guidelines For Managing Patients With Covid or of Unknown Covid Status 15nov21 - 0Gl VgNo ratings yet
- Coronavirus RCOphth Update March 18th 1Document8 pagesCoronavirus RCOphth Update March 18th 1charoiteNo ratings yet
- Guidance For Fully Vaccinated PeopleDocument6 pagesGuidance For Fully Vaccinated PeopleJim Hoft0% (1)
- COVID19-Overview PresentationDocument25 pagesCOVID19-Overview PresentationAmany AymanNo ratings yet
- Case - Management 2019 - nCoV - RRT - TOT - Training - Materia - Module - V1 - 07 - Feb - 2020Document38 pagesCase - Management 2019 - nCoV - RRT - TOT - Training - Materia - Module - V1 - 07 - Feb - 2020Usman MohammedNo ratings yet
- Kis and MegDocument31 pagesKis and MegkisNo ratings yet
- QI - CM - Module 1Document42 pagesQI - CM - Module 1Adeuga ADEKUOYENo ratings yet
- Healthcare Quality Account 2021-22Document98 pagesHealthcare Quality Account 2021-22Adeuga ADEKUOYENo ratings yet
- Perf Report Attachment 4 Trust Qual DashboardDocument3 pagesPerf Report Attachment 4 Trust Qual DashboardAdeuga ADEKUOYENo ratings yet
- Health+Advisory+leaflet Dec+2018+finalDocument4 pagesHealth+Advisory+leaflet Dec+2018+finalAdeuga ADEKUOYENo ratings yet
- Nursing Quality Plan TemplateDocument1 pageNursing Quality Plan TemplateAdeuga ADEKUOYENo ratings yet
- 4 Qlty Msur ImprvDocument16 pages4 Qlty Msur ImprvAdeuga ADEKUOYENo ratings yet
- Nursing Quality Action Plan TemplateDocument34 pagesNursing Quality Action Plan TemplateAdeuga ADEKUOYENo ratings yet
- Hospital Quality Assurance DashboardDocument10 pagesHospital Quality Assurance DashboardAdeuga ADEKUOYENo ratings yet

































































Download as pptx, pdf, or txt
You might also like
- Guidance For Routine Immunization Services During COVID-19: - PageDocument14 pagesGuidance For Routine Immunization Services During COVID-19: - PagePrisma CahyaNo ratings yet
- Coronavirus Covid 19 Guidance On Use of Personal Protective Equipment Ppe in Non Inpatient Health Care Settings During The Covid 19 OutbreakDocument6 pagesCoronavirus Covid 19 Guidance On Use of Personal Protective Equipment Ppe in Non Inpatient Health Care Settings During The Covid 19 OutbreakGerlan Madrid MingoNo ratings yet
- Mask Use in The Context of COVID-19: Interim Guidance 1 December 2020Document22 pagesMask Use in The Context of COVID-19: Interim Guidance 1 December 2020ShahabNo ratings yet
- WHO 2019 Ncov IPC - Masks 2020.5 EngDocument22 pagesWHO 2019 Ncov IPC - Masks 2020.5 EngsilviaNo ratings yet
- Issues Related To Kidney Disease and HypertensionDocument12 pagesIssues Related To Kidney Disease and HypertensionCarlos Huaman ZevallosNo ratings yet
- EPP. Am. College, Surgeons.20.Document3 pagesEPP. Am. College, Surgeons.20.Mary RodriguezNo ratings yet
- Triage, Source Control and Additional Control Measures: IPC IPCDocument33 pagesTriage, Source Control and Additional Control Measures: IPC IPCPriya RanjanNo ratings yet
- 02a - PPE - Summary and Rationale For RecommendationsDocument2 pages02a - PPE - Summary and Rationale For RecommendationsMohammedNo ratings yet
- Coronavirus Covid 19 Guidelines For Infection Prevention and Control in Residential Care Facilities - 0Document11 pagesCoronavirus Covid 19 Guidelines For Infection Prevention and Control in Residential Care Facilities - 0Shenelle NashNo ratings yet
- Mask Use in The Context of COVID-19: Interim Guidance 1 December 2020Document25 pagesMask Use in The Context of COVID-19: Interim Guidance 1 December 2020Ziyad BaraNo ratings yet
- Principles For COVID-19 Cohorting in Long-Term Care: Key Infection Prevention and Control TermsDocument7 pagesPrinciples For COVID-19 Cohorting in Long-Term Care: Key Infection Prevention and Control TermssimplyrosalynNo ratings yet
- Group 3 - NCM 119 Case Scenario - Bartolata-4ADocument6 pagesGroup 3 - NCM 119 Case Scenario - Bartolata-4AKeisha BartolataNo ratings yet
- IPC Guidelines For COVID 19Document15 pagesIPC Guidelines For COVID 19Henry OseiNo ratings yet
- IPC in HD ServicesDocument28 pagesIPC in HD ServicesseptianyganescyaNo ratings yet
- IPC GUIDELINE Version 2Document20 pagesIPC GUIDELINE Version 2Nrs KhalidNo ratings yet
- ASA Staff Safety For COVID-19: StatementDocument8 pagesASA Staff Safety For COVID-19: StatementAbidi HichemNo ratings yet
- COVID-19 Preparedness 14apr2020Document13 pagesCOVID-19 Preparedness 14apr2020Andre3893No ratings yet
- Guidance On The Use of Personal Protective Equipment Ppe in Hospitals During The Covid 19 OutbreakDocument9 pagesGuidance On The Use of Personal Protective Equipment Ppe in Hospitals During The Covid 19 OutbreakGerlan Madrid MingoNo ratings yet
- RevisedGuidelinesforDialysisofCOVID19Patients PDFDocument8 pagesRevisedGuidelinesforDialysisofCOVID19Patients PDFAmjadali ChoudhariNo ratings yet
- RevisedGuidelinesforDialysisofCOVID19Patients PDFDocument8 pagesRevisedGuidelinesforDialysisofCOVID19Patients PDFSaurav KumarNo ratings yet
- Presentation COVID-19 WHO enDocument12 pagesPresentation COVID-19 WHO enEtaferawNo ratings yet
- Suraj Clinical Management of COVID 19Document23 pagesSuraj Clinical Management of COVID 19H.M RathodNo ratings yet
- COVID 19 Outpatient DialysisDocument5 pagesCOVID 19 Outpatient DialysisTheala RadistaNo ratings yet
- Dr. Hendri - Early Warning System & PPEDocument106 pagesDr. Hendri - Early Warning System & PPEViniFortunataNo ratings yet
- Guideline Managing Critically IllDocument8 pagesGuideline Managing Critically Illmisfatrianoor10No ratings yet
- Tanzania - SOPs For Case Management and Infection Prevention and ControlDocument115 pagesTanzania - SOPs For Case Management and Infection Prevention and ControlXuan Nguyen100% (1)
- Guideline For Conservation of Respiratory Protection ResourcesDocument14 pagesGuideline For Conservation of Respiratory Protection ResourcesAMEU URGENCIASNo ratings yet
- ADA Managing COVID 19 Guide 25 March 2020Document6 pagesADA Managing COVID 19 Guide 25 March 2020Pepo BelovedNo ratings yet
- Update Who Recommendation On Covid-19 For Hospital: Setiawan Jati Laksono 10 April 2020Document34 pagesUpdate Who Recommendation On Covid-19 For Hospital: Setiawan Jati Laksono 10 April 2020Nadya FaradibaNo ratings yet
- COVID-19 PPE Training Presentation - Without Video - 6 MayDocument29 pagesCOVID-19 PPE Training Presentation - Without Video - 6 Maymeherul hasanNo ratings yet
- Phase 1 Tasks and QuestionsDocument8 pagesPhase 1 Tasks and QuestionsEmmanuel RumbaoaNo ratings yet
- Dr. Suraya's PPT - IPC COVID MX in Private Healthcare PDFDocument40 pagesDr. Suraya's PPT - IPC COVID MX in Private Healthcare PDFFrostz WongNo ratings yet
- Standard Operating ProcedureDocument15 pagesStandard Operating ProcedureAyman AliNo ratings yet
- Infection Control and Covid SafetyDocument41 pagesInfection Control and Covid SafetyAdeuga ADEKUOYENo ratings yet
- UHMS Guidelines - COVID-19 V4Document3 pagesUHMS Guidelines - COVID-19 V4Juan CruzNo ratings yet
- Australia Covid PpeDocument5 pagesAustralia Covid PpeAbidi HichemNo ratings yet
- Coronavirus Disease 2019 (COVID-19) - Infection Control in Health Care and Home Settings - UpToDateDocument40 pagesCoronavirus Disease 2019 (COVID-19) - Infection Control in Health Care and Home Settings - UpToDateFlorin StanciuNo ratings yet
- Assessment TechniquesDocument12 pagesAssessment TechniquesAeshel TabuzoNo ratings yet
- Approaches To The Management of Patients in Oral and Maxillofacial Surgery During COVID-19 PandemicDocument21 pagesApproaches To The Management of Patients in Oral and Maxillofacial Surgery During COVID-19 PandemicYahul MazfarNo ratings yet
- Annex 40 INTERIM GUIDELINES ON RESUSCITATION DURING COVID19 PANDEMICDocument15 pagesAnnex 40 INTERIM GUIDELINES ON RESUSCITATION DURING COVID19 PANDEMICAzran Shariman HasshimNo ratings yet
- Standard Operating Procedure For Handling of Corona Virus Disease (Covid-19) PatientsDocument6 pagesStandard Operating Procedure For Handling of Corona Virus Disease (Covid-19) PatientsHiJackNo ratings yet
- Infection Prevention CourseDocument73 pagesInfection Prevention Coursedakejay292No ratings yet
- Who 2019 Ncov Ipc Ppe Use 2020.3 EngDocument28 pagesWho 2019 Ncov Ipc Ppe Use 2020.3 EngKumanan1304No ratings yet
- Perioperative Considerstions in Urgent Surgical Care of Suspected and Confirmed COVID-19 Orthopaedic PatientsDocument23 pagesPerioperative Considerstions in Urgent Surgical Care of Suspected and Confirmed COVID-19 Orthopaedic PatientsDoctor's BettaNo ratings yet
- Handling Trauma and Burn PatientsDocument19 pagesHandling Trauma and Burn PatientsWhisky MiloNo ratings yet
- Interim Guidance Pediatric Patients March 27 2020Document4 pagesInterim Guidance Pediatric Patients March 27 2020Luis Alberto Anco CórdovaNo ratings yet
- dm2020 0202 PDFDocument6 pagesdm2020 0202 PDFcode4saleNo ratings yet
- SOP Triage Suspected CovidDocument29 pagesSOP Triage Suspected CovidRoy Tanda Anugrah SihotangNo ratings yet
- Universal Precautions Transmission Based PrecautionsDocument61 pagesUniversal Precautions Transmission Based PrecautionsShalamNo ratings yet
- COVID-19 Office Prep ChecklistDocument4 pagesCOVID-19 Office Prep ChecklistMohammad SahyouniNo ratings yet
- Clinical Management of COVID-19 Patients - v1Document18 pagesClinical Management of COVID-19 Patients - v1rohitNo ratings yet
- Document Can Be Found At:: /hcp/non-Us-Settings/overview/index - HTMLDocument25 pagesDocument Can Be Found At:: /hcp/non-Us-Settings/overview/index - HTMLMaqbool AlizaiNo ratings yet
- Lecture 13 IC Precautions and IsolationsDocument10 pagesLecture 13 IC Precautions and IsolationsTariq AzizNo ratings yet
- Respiratory Physiotherapy Guidelines For Managing Patients With Covid or of Unknown Covid Status 15nov21 - 0Document4 pagesRespiratory Physiotherapy Guidelines For Managing Patients With Covid or of Unknown Covid Status 15nov21 - 0Gl VgNo ratings yet
- Coronavirus RCOphth Update March 18th 1Document8 pagesCoronavirus RCOphth Update March 18th 1charoiteNo ratings yet
- Guidance For Fully Vaccinated PeopleDocument6 pagesGuidance For Fully Vaccinated PeopleJim Hoft0% (1)
- COVID19-Overview PresentationDocument25 pagesCOVID19-Overview PresentationAmany AymanNo ratings yet
- Case - Management 2019 - nCoV - RRT - TOT - Training - Materia - Module - V1 - 07 - Feb - 2020Document38 pagesCase - Management 2019 - nCoV - RRT - TOT - Training - Materia - Module - V1 - 07 - Feb - 2020Usman MohammedNo ratings yet
- Kis and MegDocument31 pagesKis and MegkisNo ratings yet
- QI - CM - Module 1Document42 pagesQI - CM - Module 1Adeuga ADEKUOYENo ratings yet
- Healthcare Quality Account 2021-22Document98 pagesHealthcare Quality Account 2021-22Adeuga ADEKUOYENo ratings yet
- Perf Report Attachment 4 Trust Qual DashboardDocument3 pagesPerf Report Attachment 4 Trust Qual DashboardAdeuga ADEKUOYENo ratings yet
- Health+Advisory+leaflet Dec+2018+finalDocument4 pagesHealth+Advisory+leaflet Dec+2018+finalAdeuga ADEKUOYENo ratings yet
- Nursing Quality Plan TemplateDocument1 pageNursing Quality Plan TemplateAdeuga ADEKUOYENo ratings yet
- 4 Qlty Msur ImprvDocument16 pages4 Qlty Msur ImprvAdeuga ADEKUOYENo ratings yet
- Nursing Quality Action Plan TemplateDocument34 pagesNursing Quality Action Plan TemplateAdeuga ADEKUOYENo ratings yet
- Hospital Quality Assurance DashboardDocument10 pagesHospital Quality Assurance DashboardAdeuga ADEKUOYENo ratings yet