
Neuro Dynamics
Neuro Dynamics
You might also like
- Butler 1991 Mobilisation of The Nervous SystemDocument265 pagesButler 1991 Mobilisation of The Nervous Systemiruizmolina67% (15)
- (David Weinstock) NeuroKinetic Therapy An InnovatDocument151 pages(David Weinstock) NeuroKinetic Therapy An Innovatsitti fatimah azzahra. m100% (2)
- The Neurodynamic TechniquesDocument58 pagesThe Neurodynamic TechniquesJohn Durham100% (44)
- Facilitated Positional Release FPRDocument12 pagesFacilitated Positional Release FPRcoahuiltecoNo ratings yet
- Visceral Manipulation in Osteopathy Eric Hebgen.11867 3pancreasDocument5 pagesVisceral Manipulation in Osteopathy Eric Hebgen.11867 3pancreasIoan Andra50% (4)
- P DTR EngDocument24 pagesP DTR Engkenzaimon80% (5)
- Lossing BerylArbucklesCranial PDFDocument67 pagesLossing BerylArbucklesCranial PDFdeemoney3100% (2)
- Fascial Manipulations For Internal Pain PDFDocument16 pagesFascial Manipulations For Internal Pain PDFdavidzhou0% (2)
- Kinetic ChainsDocument5 pagesKinetic ChainsYermia RashaquatNo ratings yet
- Hip MaitlandDocument14 pagesHip Maitlandakuphysio100% (1)
- Workshop 1 PowerpointDocument10 pagesWorkshop 1 PowerpointCarlos CorreaNo ratings yet
- AAO FDM Indroduction 1994 PDFDocument12 pagesAAO FDM Indroduction 1994 PDFHONGJYNo ratings yet
- Diagnostic Touch Parts I IV by Rollin Becker PDFDocument69 pagesDiagnostic Touch Parts I IV by Rollin Becker PDFCatalin EneNo ratings yet
- Spinal Care and Its Effects On Human Physiology in Sickness and in HealthDocument196 pagesSpinal Care and Its Effects On Human Physiology in Sickness and in HealthMichael Koontz67% (3)
- 2014 SAAO Forum For 10-18-11 Cranial IntroDocument5 pages2014 SAAO Forum For 10-18-11 Cranial IntroRoger NakataNo ratings yet
- Fotocopias Ingles Tema Climate 1º EsoDocument6 pagesFotocopias Ingles Tema Climate 1º EsoMayOrdóñezNo ratings yet
- Aetiology, Pathology and Management of Enterocutaneous FistulaDocument34 pagesAetiology, Pathology and Management of Enterocutaneous Fistularoselinekhadija100% (2)
- Physio Shacklock 95Document8 pagesPhysio Shacklock 95Raihan HabibNo ratings yet
- Length Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesRating: 1 out of 5 stars1/5 (1)
- Length Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesRating: 3.5 out of 5 stars3.5/5 (3)
- Mobilization and Stimulation of Neuromuscular Tissue (MaSoNT)From EverandMobilization and Stimulation of Neuromuscular Tissue (MaSoNT)No ratings yet
- Lossing DiagnosingTreatingDu PDFDocument33 pagesLossing DiagnosingTreatingDu PDFDiana SchlittlerNo ratings yet
- CWK en DemoDocument16 pagesCWK en DemoVishal YogiNo ratings yet
- Movement, Stability & Lumbopelvic Pain: Integration of Research and Therapy - Andry VleemingDocument4 pagesMovement, Stability & Lumbopelvic Pain: Integration of Research and Therapy - Andry VleemingwopegiluNo ratings yet
- Application of Fascial Manipulation Technique in Chronic Shoulder PainDocument9 pagesApplication of Fascial Manipulation Technique in Chronic Shoulder PainIsabelGuijarroMartinezNo ratings yet
- Working With Headaches, Part III: Techniques For Migraines (Myofascial Techniques)Document5 pagesWorking With Headaches, Part III: Techniques For Migraines (Myofascial Techniques)Advanced-Trainings.com100% (5)
- Fascial Distortion Model - Vol.2Document62 pagesFascial Distortion Model - Vol.2Magno FilhoNo ratings yet
- Manual Therapy Techniques For The KneeDocument11 pagesManual Therapy Techniques For The KneeSaumitra Phadke100% (2)
- Myofascial Release: Range of Motion and FlexibilityDocument21 pagesMyofascial Release: Range of Motion and FlexibilityMonika100% (1)
- Fascial Manipulation DescriptionDocument7 pagesFascial Manipulation DescriptionPopescu MariusNo ratings yet
- Toilet Wall Muscle O, I, A, NsDocument34 pagesToilet Wall Muscle O, I, A, Nsiruizmolina100% (1)
- Understanding The Stretch ReflexDocument2 pagesUnderstanding The Stretch ReflexJingyan ZhangNo ratings yet
- Ligamentous Articular Strain - Osteopathic ManipulativeDocument20 pagesLigamentous Articular Strain - Osteopathic Manipulativeisa_martínezNo ratings yet
- L Kalichman PDFDocument28 pagesL Kalichman PDFShahul HameedNo ratings yet
- Counterstrain - Approaches in Osteopathic Manipulative Medicine (Friedman)Document108 pagesCounterstrain - Approaches in Osteopathic Manipulative Medicine (Friedman)Alessandro100% (2)
- Osteopathic Fascial ManipulationDocument9 pagesOsteopathic Fascial ManipulationnunoNo ratings yet
- Clinical Neurodynamics and Sports Medicine: Origins and DevelopmentDocument8 pagesClinical Neurodynamics and Sports Medicine: Origins and DevelopmentWahid NasrudinNo ratings yet
- Fascial Strain Counter Strain 2013Document8 pagesFascial Strain Counter Strain 2013Rui Pedro Pereira100% (1)
- An Osteopathic Approach To Torticollis Plagiocephaly and Otitis Media 2014-15Document24 pagesAn Osteopathic Approach To Torticollis Plagiocephaly and Otitis Media 2014-15johnNo ratings yet
- Mulligan Therapy: What Is It and How Does It WorkDocument33 pagesMulligan Therapy: What Is It and How Does It WorkAgus SantosoNo ratings yet
- 1400 - Still Technique For OOADocument17 pages1400 - Still Technique For OOAFinish Your WorkNo ratings yet
- Working With Whiplash, Part II (Myofascial Techniques)Document5 pagesWorking With Whiplash, Part II (Myofascial Techniques)Advanced-Trainings.com100% (2)
- An Osteopathic Approach To Children - Jane Elizabeth Carreiro DODocument4 pagesAn Osteopathic Approach To Children - Jane Elizabeth Carreiro DOdekeguryNo ratings yet
- Chiropractic Line AnalysisDocument10 pagesChiropractic Line AnalysisD N BidNo ratings yet
- VojitaDocument19 pagesVojitaShemjaz ArakkalNo ratings yet
- Chapter 3 - Fundamentals of Applied KinesiologyDocument60 pagesChapter 3 - Fundamentals of Applied KinesiologySam100% (1)
- Course Material - Manual TherapyDocument196 pagesCourse Material - Manual Therapypuntocom111100% (1)
- Shoulder Assessment: Ayesha RazzaqDocument47 pagesShoulder Assessment: Ayesha Razzaqayesha100% (1)
- MVT 2019Document65 pagesMVT 2019Rizal100% (10)
- Manual Therapy: DR - DharmavatiDocument78 pagesManual Therapy: DR - DharmavatiHitesh RohitNo ratings yet
- Benefits and Limitations of Vojta ApproachDocument50 pagesBenefits and Limitations of Vojta ApproachAlice Teodorescu100% (3)
- Maitland ShoulderDocument91 pagesMaitland ShoulderAyesha Sameen100% (1)
- Effectiveness of Mulligan's Mobilization Technique Versus Eccentric Exercises On Pain, Hand Grip Strength and Function in Subjects With Lateral EpicondylitisDocument8 pagesEffectiveness of Mulligan's Mobilization Technique Versus Eccentric Exercises On Pain, Hand Grip Strength and Function in Subjects With Lateral EpicondylitisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Practical Guide For Therapists Acrobat7 PDFDocument40 pagesA Practical Guide For Therapists Acrobat7 PDFmitroisergiu100% (1)
- Visceral OsteopathyDocument72 pagesVisceral Osteopathykhorrami492% (13)
- Introduction To Osteopathy in The Cranial Field - American Academy (PDFDrive)Document53 pagesIntroduction To Osteopathy in The Cranial Field - American Academy (PDFDrive)RukaphuongNo ratings yet
- Strain Counter-Strain PDFDocument7 pagesStrain Counter-Strain PDFCarlosCarpinteroRubioNo ratings yet
- BobathDocument150 pagesBobathramesh natrayan100% (1)
- Manual Trigger Point Therapy and Dry Needling Top 30 MusclesDocument84 pagesManual Trigger Point Therapy and Dry Needling Top 30 MusclesManuela CormioNo ratings yet
- The Mulligan Concept of Manual Therapy: Textbook of Techniques - Wayne HingDocument5 pagesThe Mulligan Concept of Manual Therapy: Textbook of Techniques - Wayne Hingzaladiry50% (4)
- KINETO 1 Myofascial Release and Met Presentation SlidesDocument90 pagesKINETO 1 Myofascial Release and Met Presentation Slidesdavidescu5costinNo ratings yet
- Manual Therapy Techniques For The ShoulderDocument12 pagesManual Therapy Techniques For The Shoulderubiktrash1492100% (1)
- Myofascial ReleaseDocument30 pagesMyofascial ReleaseRahul ChhatlaniNo ratings yet
- Manual Muscle Test (MMT) : Prepared By: DR - Rahul Chhatlani MPT (Neuro)Document80 pagesManual Muscle Test (MMT) : Prepared By: DR - Rahul Chhatlani MPT (Neuro)Rahul ChhatlaniNo ratings yet
- Joint Mobilization LectureDocument58 pagesJoint Mobilization LectureRahul ChhatlaniNo ratings yet
- Aquatic TherapyDocument29 pagesAquatic TherapyRahul Chhatlani100% (1)
- Ancient Egyptian Agriculture - WikipediaDocument39 pagesAncient Egyptian Agriculture - WikipediaDiawara HawkeyeNo ratings yet
- Manual Spray GunDocument6 pagesManual Spray GunSyazwan KhairulNo ratings yet
- NeuroVascular (NV) Holding PointsDocument2 pagesNeuroVascular (NV) Holding PointsHatem Farouk100% (2)
- BRS TestDocument2 pagesBRS TestMuhammad Ibrahim KhanNo ratings yet
- Cylone - Lab Report - FinalizeDocument19 pagesCylone - Lab Report - FinalizeSiti Khairunnur LaderlahNo ratings yet
- TN-4620190912122 Form21B Signed PDFDocument1 pageTN-4620190912122 Form21B Signed PDFDHEEN MEDICALSNo ratings yet
- Physician'S Order/Progress Notes: 23 S. Avila Male JhonDocument2 pagesPhysician'S Order/Progress Notes: 23 S. Avila Male JhonKrizha Angela Nicolas100% (1)
- Long Quiz Earth Sci 11Document2 pagesLong Quiz Earth Sci 11Jesha mae MagnoNo ratings yet
- Material Sub Group Item CodeDocument2,818 pagesMaterial Sub Group Item Codegouri gouriNo ratings yet
- Neon NagaramDocument235 pagesNeon NagaramShammeer0% (1)
- Over The Counter MedicinesDocument3 pagesOver The Counter MedicinesJhun Echipare100% (3)
- Ebook Chemistry For Today General Organic and Biochemistry PDF Full Chapter PDFDocument67 pagesEbook Chemistry For Today General Organic and Biochemistry PDF Full Chapter PDFrobert.davidson233100% (31)
- Electrical and Electronic Troubleshooting For Industrial EnginesDocument25 pagesElectrical and Electronic Troubleshooting For Industrial EnginespanddyanNo ratings yet
- A Country Boy Quits SchoolDocument4 pagesA Country Boy Quits SchoolJamaica Bianca Baynosa AnguloNo ratings yet
- Model ETR-9200 Automatic Tuning Smarter Logic ControllerDocument26 pagesModel ETR-9200 Automatic Tuning Smarter Logic ControllervhelectronicaNo ratings yet
- PhilRice - Fertilizer CalculationDocument21 pagesPhilRice - Fertilizer CalculationMichelle Ann SoledadNo ratings yet
- Maternal Adaptation To Pregnancy1Document27 pagesMaternal Adaptation To Pregnancy1Indra MahyulNo ratings yet
- Lecture 4Document22 pagesLecture 4SUNDAS FATIMANo ratings yet
- ALI2 P Data SheetDocument4 pagesALI2 P Data SheetFlorent YIBOKOUNo ratings yet
- Distribution Network of Coca-ColaDocument16 pagesDistribution Network of Coca-ColaRahul panditaNo ratings yet
- Fiberdyne G.652.D Single Mode Fiber SpecificationsDocument1 pageFiberdyne G.652.D Single Mode Fiber SpecificationsjunedNo ratings yet
- Final LIST OF IMPORTANT GRID ELEMENTS Updated On May 2020 PDFDocument74 pagesFinal LIST OF IMPORTANT GRID ELEMENTS Updated On May 2020 PDFbhargavNo ratings yet
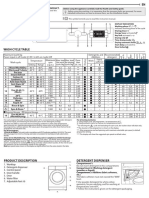
- Whirlpool BIWDWG861484uk enDocument4 pagesWhirlpool BIWDWG861484uk ennadaljoachim77No ratings yet
- Exploded View & Parts Listing Air Operated Double Diaphragm PumpDocument3 pagesExploded View & Parts Listing Air Operated Double Diaphragm PumpEdgar NercarNo ratings yet
- Ocean Aerosols Climate ImpactDocument14 pagesOcean Aerosols Climate ImpactSustainability ManagementNo ratings yet
- Case Study On A Highway Project: Environmental Impact AssesmentDocument10 pagesCase Study On A Highway Project: Environmental Impact AssesmentSRUTHI FRANCIS M.Tech Environmental Engineering 2020-2022No ratings yet
- Stilboestrol Tablets MSDSDocument6 pagesStilboestrol Tablets MSDSIsaac lauricNo ratings yet
- Vikas BhagwanDocument13 pagesVikas BhagwanhappysinNo ratings yet



























































































Download as pptx, pdf, or txt
You might also like
- Butler 1991 Mobilisation of The Nervous SystemDocument265 pagesButler 1991 Mobilisation of The Nervous Systemiruizmolina67% (15)
- (David Weinstock) NeuroKinetic Therapy An InnovatDocument151 pages(David Weinstock) NeuroKinetic Therapy An Innovatsitti fatimah azzahra. m100% (2)
- The Neurodynamic TechniquesDocument58 pagesThe Neurodynamic TechniquesJohn Durham100% (44)
- Facilitated Positional Release FPRDocument12 pagesFacilitated Positional Release FPRcoahuiltecoNo ratings yet
- Visceral Manipulation in Osteopathy Eric Hebgen.11867 3pancreasDocument5 pagesVisceral Manipulation in Osteopathy Eric Hebgen.11867 3pancreasIoan Andra50% (4)
- P DTR EngDocument24 pagesP DTR Engkenzaimon80% (5)
- Lossing BerylArbucklesCranial PDFDocument67 pagesLossing BerylArbucklesCranial PDFdeemoney3100% (2)
- Fascial Manipulations For Internal Pain PDFDocument16 pagesFascial Manipulations For Internal Pain PDFdavidzhou0% (2)
- Kinetic ChainsDocument5 pagesKinetic ChainsYermia RashaquatNo ratings yet
- Hip MaitlandDocument14 pagesHip Maitlandakuphysio100% (1)
- Workshop 1 PowerpointDocument10 pagesWorkshop 1 PowerpointCarlos CorreaNo ratings yet
- AAO FDM Indroduction 1994 PDFDocument12 pagesAAO FDM Indroduction 1994 PDFHONGJYNo ratings yet
- Diagnostic Touch Parts I IV by Rollin Becker PDFDocument69 pagesDiagnostic Touch Parts I IV by Rollin Becker PDFCatalin EneNo ratings yet
- Spinal Care and Its Effects On Human Physiology in Sickness and in HealthDocument196 pagesSpinal Care and Its Effects On Human Physiology in Sickness and in HealthMichael Koontz67% (3)
- 2014 SAAO Forum For 10-18-11 Cranial IntroDocument5 pages2014 SAAO Forum For 10-18-11 Cranial IntroRoger NakataNo ratings yet
- Fotocopias Ingles Tema Climate 1º EsoDocument6 pagesFotocopias Ingles Tema Climate 1º EsoMayOrdóñezNo ratings yet
- Aetiology, Pathology and Management of Enterocutaneous FistulaDocument34 pagesAetiology, Pathology and Management of Enterocutaneous Fistularoselinekhadija100% (2)
- Physio Shacklock 95Document8 pagesPhysio Shacklock 95Raihan HabibNo ratings yet
- Length Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesRating: 1 out of 5 stars1/5 (1)
- Length Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesRating: 3.5 out of 5 stars3.5/5 (3)
- Mobilization and Stimulation of Neuromuscular Tissue (MaSoNT)From EverandMobilization and Stimulation of Neuromuscular Tissue (MaSoNT)No ratings yet
- Lossing DiagnosingTreatingDu PDFDocument33 pagesLossing DiagnosingTreatingDu PDFDiana SchlittlerNo ratings yet
- CWK en DemoDocument16 pagesCWK en DemoVishal YogiNo ratings yet
- Movement, Stability & Lumbopelvic Pain: Integration of Research and Therapy - Andry VleemingDocument4 pagesMovement, Stability & Lumbopelvic Pain: Integration of Research and Therapy - Andry VleemingwopegiluNo ratings yet
- Application of Fascial Manipulation Technique in Chronic Shoulder PainDocument9 pagesApplication of Fascial Manipulation Technique in Chronic Shoulder PainIsabelGuijarroMartinezNo ratings yet
- Working With Headaches, Part III: Techniques For Migraines (Myofascial Techniques)Document5 pagesWorking With Headaches, Part III: Techniques For Migraines (Myofascial Techniques)Advanced-Trainings.com100% (5)
- Fascial Distortion Model - Vol.2Document62 pagesFascial Distortion Model - Vol.2Magno FilhoNo ratings yet
- Manual Therapy Techniques For The KneeDocument11 pagesManual Therapy Techniques For The KneeSaumitra Phadke100% (2)
- Myofascial Release: Range of Motion and FlexibilityDocument21 pagesMyofascial Release: Range of Motion and FlexibilityMonika100% (1)
- Fascial Manipulation DescriptionDocument7 pagesFascial Manipulation DescriptionPopescu MariusNo ratings yet
- Toilet Wall Muscle O, I, A, NsDocument34 pagesToilet Wall Muscle O, I, A, Nsiruizmolina100% (1)
- Understanding The Stretch ReflexDocument2 pagesUnderstanding The Stretch ReflexJingyan ZhangNo ratings yet
- Ligamentous Articular Strain - Osteopathic ManipulativeDocument20 pagesLigamentous Articular Strain - Osteopathic Manipulativeisa_martínezNo ratings yet
- L Kalichman PDFDocument28 pagesL Kalichman PDFShahul HameedNo ratings yet
- Counterstrain - Approaches in Osteopathic Manipulative Medicine (Friedman)Document108 pagesCounterstrain - Approaches in Osteopathic Manipulative Medicine (Friedman)Alessandro100% (2)
- Osteopathic Fascial ManipulationDocument9 pagesOsteopathic Fascial ManipulationnunoNo ratings yet
- Clinical Neurodynamics and Sports Medicine: Origins and DevelopmentDocument8 pagesClinical Neurodynamics and Sports Medicine: Origins and DevelopmentWahid NasrudinNo ratings yet
- Fascial Strain Counter Strain 2013Document8 pagesFascial Strain Counter Strain 2013Rui Pedro Pereira100% (1)
- An Osteopathic Approach To Torticollis Plagiocephaly and Otitis Media 2014-15Document24 pagesAn Osteopathic Approach To Torticollis Plagiocephaly and Otitis Media 2014-15johnNo ratings yet
- Mulligan Therapy: What Is It and How Does It WorkDocument33 pagesMulligan Therapy: What Is It and How Does It WorkAgus SantosoNo ratings yet
- 1400 - Still Technique For OOADocument17 pages1400 - Still Technique For OOAFinish Your WorkNo ratings yet
- Working With Whiplash, Part II (Myofascial Techniques)Document5 pagesWorking With Whiplash, Part II (Myofascial Techniques)Advanced-Trainings.com100% (2)
- An Osteopathic Approach To Children - Jane Elizabeth Carreiro DODocument4 pagesAn Osteopathic Approach To Children - Jane Elizabeth Carreiro DOdekeguryNo ratings yet
- Chiropractic Line AnalysisDocument10 pagesChiropractic Line AnalysisD N BidNo ratings yet
- VojitaDocument19 pagesVojitaShemjaz ArakkalNo ratings yet
- Chapter 3 - Fundamentals of Applied KinesiologyDocument60 pagesChapter 3 - Fundamentals of Applied KinesiologySam100% (1)
- Course Material - Manual TherapyDocument196 pagesCourse Material - Manual Therapypuntocom111100% (1)
- Shoulder Assessment: Ayesha RazzaqDocument47 pagesShoulder Assessment: Ayesha Razzaqayesha100% (1)
- MVT 2019Document65 pagesMVT 2019Rizal100% (10)
- Manual Therapy: DR - DharmavatiDocument78 pagesManual Therapy: DR - DharmavatiHitesh RohitNo ratings yet
- Benefits and Limitations of Vojta ApproachDocument50 pagesBenefits and Limitations of Vojta ApproachAlice Teodorescu100% (3)
- Maitland ShoulderDocument91 pagesMaitland ShoulderAyesha Sameen100% (1)
- Effectiveness of Mulligan's Mobilization Technique Versus Eccentric Exercises On Pain, Hand Grip Strength and Function in Subjects With Lateral EpicondylitisDocument8 pagesEffectiveness of Mulligan's Mobilization Technique Versus Eccentric Exercises On Pain, Hand Grip Strength and Function in Subjects With Lateral EpicondylitisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Practical Guide For Therapists Acrobat7 PDFDocument40 pagesA Practical Guide For Therapists Acrobat7 PDFmitroisergiu100% (1)
- Visceral OsteopathyDocument72 pagesVisceral Osteopathykhorrami492% (13)
- Introduction To Osteopathy in The Cranial Field - American Academy (PDFDrive)Document53 pagesIntroduction To Osteopathy in The Cranial Field - American Academy (PDFDrive)RukaphuongNo ratings yet
- Strain Counter-Strain PDFDocument7 pagesStrain Counter-Strain PDFCarlosCarpinteroRubioNo ratings yet
- BobathDocument150 pagesBobathramesh natrayan100% (1)
- Manual Trigger Point Therapy and Dry Needling Top 30 MusclesDocument84 pagesManual Trigger Point Therapy and Dry Needling Top 30 MusclesManuela CormioNo ratings yet
- The Mulligan Concept of Manual Therapy: Textbook of Techniques - Wayne HingDocument5 pagesThe Mulligan Concept of Manual Therapy: Textbook of Techniques - Wayne Hingzaladiry50% (4)
- KINETO 1 Myofascial Release and Met Presentation SlidesDocument90 pagesKINETO 1 Myofascial Release and Met Presentation Slidesdavidescu5costinNo ratings yet
- Manual Therapy Techniques For The ShoulderDocument12 pagesManual Therapy Techniques For The Shoulderubiktrash1492100% (1)
- Myofascial ReleaseDocument30 pagesMyofascial ReleaseRahul ChhatlaniNo ratings yet
- Manual Muscle Test (MMT) : Prepared By: DR - Rahul Chhatlani MPT (Neuro)Document80 pagesManual Muscle Test (MMT) : Prepared By: DR - Rahul Chhatlani MPT (Neuro)Rahul ChhatlaniNo ratings yet
- Joint Mobilization LectureDocument58 pagesJoint Mobilization LectureRahul ChhatlaniNo ratings yet
- Aquatic TherapyDocument29 pagesAquatic TherapyRahul Chhatlani100% (1)
- Ancient Egyptian Agriculture - WikipediaDocument39 pagesAncient Egyptian Agriculture - WikipediaDiawara HawkeyeNo ratings yet
- Manual Spray GunDocument6 pagesManual Spray GunSyazwan KhairulNo ratings yet
- NeuroVascular (NV) Holding PointsDocument2 pagesNeuroVascular (NV) Holding PointsHatem Farouk100% (2)
- BRS TestDocument2 pagesBRS TestMuhammad Ibrahim KhanNo ratings yet
- Cylone - Lab Report - FinalizeDocument19 pagesCylone - Lab Report - FinalizeSiti Khairunnur LaderlahNo ratings yet
- TN-4620190912122 Form21B Signed PDFDocument1 pageTN-4620190912122 Form21B Signed PDFDHEEN MEDICALSNo ratings yet
- Physician'S Order/Progress Notes: 23 S. Avila Male JhonDocument2 pagesPhysician'S Order/Progress Notes: 23 S. Avila Male JhonKrizha Angela Nicolas100% (1)
- Long Quiz Earth Sci 11Document2 pagesLong Quiz Earth Sci 11Jesha mae MagnoNo ratings yet
- Material Sub Group Item CodeDocument2,818 pagesMaterial Sub Group Item Codegouri gouriNo ratings yet
- Neon NagaramDocument235 pagesNeon NagaramShammeer0% (1)
- Over The Counter MedicinesDocument3 pagesOver The Counter MedicinesJhun Echipare100% (3)
- Ebook Chemistry For Today General Organic and Biochemistry PDF Full Chapter PDFDocument67 pagesEbook Chemistry For Today General Organic and Biochemistry PDF Full Chapter PDFrobert.davidson233100% (31)
- Electrical and Electronic Troubleshooting For Industrial EnginesDocument25 pagesElectrical and Electronic Troubleshooting For Industrial EnginespanddyanNo ratings yet
- A Country Boy Quits SchoolDocument4 pagesA Country Boy Quits SchoolJamaica Bianca Baynosa AnguloNo ratings yet
- Model ETR-9200 Automatic Tuning Smarter Logic ControllerDocument26 pagesModel ETR-9200 Automatic Tuning Smarter Logic ControllervhelectronicaNo ratings yet
- PhilRice - Fertilizer CalculationDocument21 pagesPhilRice - Fertilizer CalculationMichelle Ann SoledadNo ratings yet
- Maternal Adaptation To Pregnancy1Document27 pagesMaternal Adaptation To Pregnancy1Indra MahyulNo ratings yet
- Lecture 4Document22 pagesLecture 4SUNDAS FATIMANo ratings yet
- ALI2 P Data SheetDocument4 pagesALI2 P Data SheetFlorent YIBOKOUNo ratings yet
- Distribution Network of Coca-ColaDocument16 pagesDistribution Network of Coca-ColaRahul panditaNo ratings yet
- Fiberdyne G.652.D Single Mode Fiber SpecificationsDocument1 pageFiberdyne G.652.D Single Mode Fiber SpecificationsjunedNo ratings yet
- Final LIST OF IMPORTANT GRID ELEMENTS Updated On May 2020 PDFDocument74 pagesFinal LIST OF IMPORTANT GRID ELEMENTS Updated On May 2020 PDFbhargavNo ratings yet
- Whirlpool BIWDWG861484uk enDocument4 pagesWhirlpool BIWDWG861484uk ennadaljoachim77No ratings yet
- Exploded View & Parts Listing Air Operated Double Diaphragm PumpDocument3 pagesExploded View & Parts Listing Air Operated Double Diaphragm PumpEdgar NercarNo ratings yet
- Ocean Aerosols Climate ImpactDocument14 pagesOcean Aerosols Climate ImpactSustainability ManagementNo ratings yet
- Case Study On A Highway Project: Environmental Impact AssesmentDocument10 pagesCase Study On A Highway Project: Environmental Impact AssesmentSRUTHI FRANCIS M.Tech Environmental Engineering 2020-2022No ratings yet
- Stilboestrol Tablets MSDSDocument6 pagesStilboestrol Tablets MSDSIsaac lauricNo ratings yet
- Vikas BhagwanDocument13 pagesVikas BhagwanhappysinNo ratings yet