
Ild Final
Ild Final
You might also like
- Chicken Nutrition - A Guide For Nutritionists and Poultry ProfessionalsDocument23 pagesChicken Nutrition - A Guide For Nutritionists and Poultry Professionalsronx0% (1)
- Psychiatric Case StudyDocument32 pagesPsychiatric Case Studyrachael86% (35)
- Provide Support To People Living With DementiaDocument9 pagesProvide Support To People Living With DementiaGurpreet Singh WirringNo ratings yet
- 9.interstitial Lung DiseasesDocument4 pages9.interstitial Lung DiseasesLankeshwaraNo ratings yet
- (2018) - Flujo Inspiratorio Máximo Como Predictor de Traqueotomía.Document4 pages(2018) - Flujo Inspiratorio Máximo Como Predictor de Traqueotomía.luribe662No ratings yet
- 1 s2.0 S0899707122000298 MainDocument12 pages1 s2.0 S0899707122000298 Mainrivai anwarNo ratings yet
- Rosette Forming Glioneuronal Tumor (RFGNT) Extremely Rare Entity - CopieDocument16 pagesRosette Forming Glioneuronal Tumor (RFGNT) Extremely Rare Entity - CopieCalin M.No ratings yet
- Difficulties Diagnosing Ipf - Simon WalshDocument95 pagesDifficulties Diagnosing Ipf - Simon WalshcuvinhNo ratings yet
- Idiopathic Pulmonary Fibrosis NEWDocument34 pagesIdiopathic Pulmonary Fibrosis NEWrahayuNo ratings yet
- Lung Lobe Torsion in 15 Dogs - Peripheral Band Sign On UltrasoundDocument10 pagesLung Lobe Torsion in 15 Dogs - Peripheral Band Sign On UltrasoundAdan Camilo Ramirez CarranzaNo ratings yet
- 920 FullDocument17 pages920 FullHeru SigitNo ratings yet
- Postgraduate Course 3 Radiological-Pathological Correlation of Tumoural and Non-Tumoural Pathology: An Interdisciplinary ApproachDocument31 pagesPostgraduate Course 3 Radiological-Pathological Correlation of Tumoural and Non-Tumoural Pathology: An Interdisciplinary ApproachBulborea MihaelaNo ratings yet
- 2015 Chest - Blue & Falls ProtocolsDocument12 pages2015 Chest - Blue & Falls ProtocolsWilmer Yanquen VillarrealNo ratings yet
- BLUE-Protocol and FALLS-Protocol: Two Applications of Lung Ultrasound in The Critically IllDocument12 pagesBLUE-Protocol and FALLS-Protocol: Two Applications of Lung Ultrasound in The Critically IllChristiaan CordovaNo ratings yet
- BLUE & FALLS Protocol LichensteinDocument12 pagesBLUE & FALLS Protocol LichensteinCarlos MoncayoNo ratings yet
- Ipf UipDocument39 pagesIpf UipSai Nandan ReddyNo ratings yet
- Ipaf 2019 CCM - 230215 - 064414Document9 pagesIpaf 2019 CCM - 230215 - 064414Robert Arana NarváezNo ratings yet
- Edoskopi FleksibelDocument4 pagesEdoskopi FleksibelDex RayNo ratings yet
- DR Oea KhairsyafDocument30 pagesDR Oea KhairsyafErdyNo ratings yet
- Cherian2019 PDFDocument23 pagesCherian2019 PDFnugra raturandangNo ratings yet
- CT Features of Community-Acquired Pneumonia at The Emergency DepartmentDocument8 pagesCT Features of Community-Acquired Pneumonia at The Emergency DepartmentpachomdNo ratings yet
- WCS 015 - Shortness of Breath in A Construction Site Worker - Occupational Lung Diseases - Pulmonary Fibrosis - Workman's Compensation by DR DCL LamDocument60 pagesWCS 015 - Shortness of Breath in A Construction Site Worker - Occupational Lung Diseases - Pulmonary Fibrosis - Workman's Compensation by DR DCL LamJenniferFooNo ratings yet
- Bronquiolite DiagnosticoDocument14 pagesBronquiolite DiagnosticoFrederico PóvoaNo ratings yet
- CPC Interventional RadiologyDocument138 pagesCPC Interventional RadiologyEbrahim Adel Ali AhmedNo ratings yet
- 65364a4a96254 IJAR-44785Document6 pages65364a4a96254 IJAR-44785asrindustriesisavailableNo ratings yet
- Jrcollphyslond146949 0029bDocument7 pagesJrcollphyslond146949 0029bArun JadhavNo ratings yet
- Hypersensitivity Pneumonitis: Diagnostic and Therapeutic ChallengesDocument51 pagesHypersensitivity Pneumonitis: Diagnostic and Therapeutic ChallengesskchhabraNo ratings yet
- Hypersensitivity Pneumonitis: Diagnostic and Therapeutic ChallengesDocument51 pagesHypersensitivity Pneumonitis: Diagnostic and Therapeutic ChallengesskchhabraNo ratings yet
- Routine Use of Point-of-Care Lung Ultrasound During The COVID-19 PandemicDocument4 pagesRoutine Use of Point-of-Care Lung Ultrasound During The COVID-19 PandemicOswaldo MontesNo ratings yet
- Uip and NsipDocument38 pagesUip and NsipReem AbbasNo ratings yet
- Wang 2017Document9 pagesWang 2017juanrangoneNo ratings yet
- BSTI COVID-19 Radiology Guidance Version 2 16.03.20 PDFDocument28 pagesBSTI COVID-19 Radiology Guidance Version 2 16.03.20 PDFAlejandro RojasNo ratings yet
- Interventional Radiology: A Manual For Surgeons and RadiologistsDocument24 pagesInterventional Radiology: A Manual For Surgeons and RadiologistsMaria KristinaNo ratings yet
- ENT Lecture FinalDocument65 pagesENT Lecture FinalNejib M/AminNo ratings yet
- BLUE-Protocol and FALLS-ProtocolDocument12 pagesBLUE-Protocol and FALLS-ProtocolChris Vam SanchezNo ratings yet
- Ijcmr 2324 v1 1Document6 pagesIjcmr 2324 v1 1ahsaanillahi9No ratings yet
- Organizing Pneumonia: Chest HRCT Findings : Pneumonia em Organização: Achados Da TCAR de TóraxDocument7 pagesOrganizing Pneumonia: Chest HRCT Findings : Pneumonia em Organização: Achados Da TCAR de TóraxPutra PratamaNo ratings yet
- Arya - Usefulness and Safety of Transbronchial Biopsy With Large Forceps During Flexible BronchosDocument5 pagesArya - Usefulness and Safety of Transbronchial Biopsy With Large Forceps During Flexible BronchosXaralyn XaviereNo ratings yet
- Andronik Ou 2013Document16 pagesAndronik Ou 2013MayNo ratings yet
- 2008 Chest - The Blue ProtocolDocument9 pages2008 Chest - The Blue Protocoleduardo0% (1)
- Ryct 2021200279Document19 pagesRyct 2021200279Andiie ResminNo ratings yet
- Radiology RoundsDocument30 pagesRadiology RoundsKelum BuddhikaNo ratings yet
- 2.significance of Fuchs Flecks in Patients With Pterygium Loght DamageDocument4 pages2.significance of Fuchs Flecks in Patients With Pterygium Loght DamagedelaNo ratings yet
- Focus: NeurosurgicalDocument7 pagesFocus: NeurosurgicalGaetano De BiaseNo ratings yet
- Ild Cme SlidesDocument93 pagesIld Cme SlidesJagbir Singh KanetNo ratings yet
- Can Malignant and Benign Pulmonary Nodules Be Differentiated With Diffusion-Weighted MRI?Document7 pagesCan Malignant and Benign Pulmonary Nodules Be Differentiated With Diffusion-Weighted MRI?Patta DaengNo ratings yet
- Thoracic Ultrasonography A Narrative ReviewDocument12 pagesThoracic Ultrasonography A Narrative ReviewJHONATAN MATA ARANDANo ratings yet
- Final PFT Day 1Document11 pagesFinal PFT Day 1Quevee CondezNo ratings yet
- Anesthesia Considerations in Microlaryngoscopy or Direct LaryngosDocument6 pagesAnesthesia Considerations in Microlaryngoscopy or Direct LaryngosRubén Darío HerediaNo ratings yet
- Clinical Practice GuidelinesDocument3 pagesClinical Practice GuidelinessigitNo ratings yet
- Respirology - 2011 - KOEGELENBERG - Pleural Controversy Closed Needle Pleural Biopsy or Thoracoscopy Which FirstDocument9 pagesRespirology - 2011 - KOEGELENBERG - Pleural Controversy Closed Needle Pleural Biopsy or Thoracoscopy Which Firstdalozpa23No ratings yet
- Lipoma of The Parotid Gland Extending From The Superficial To The Deep Lobe Case ReportDocument4 pagesLipoma of The Parotid Gland Extending From The Superficial To The Deep Lobe Case ReportHerald Scholarly Open AccessNo ratings yet
- 865 FullDocument16 pages865 Fullaieyha hamkaNo ratings yet
- Jurnal Radio Inggris TalDocument17 pagesJurnal Radio Inggris TalimamattamamiNo ratings yet
- Plain Film and HRCT Diagnosis of Interstitial Lung Disease: Sujal R. Desai, Helmut Prosch, and Jeffrey R. GalvinDocument9 pagesPlain Film and HRCT Diagnosis of Interstitial Lung Disease: Sujal R. Desai, Helmut Prosch, and Jeffrey R. GalvinVictor ChiabaiNo ratings yet
- Idiopathic Pulmonary Fibrosis: Diagnosis, Epidemiology and Natural HistoryDocument11 pagesIdiopathic Pulmonary Fibrosis: Diagnosis, Epidemiology and Natural HistorySuwandi AlghozyNo ratings yet
- Boonsarngsuk - Factors Affecting The Diagnostic Yield of Flexible Bronchoscopy Without Guidance in Pulmonary Nodules or MassesDocument6 pagesBoonsarngsuk - Factors Affecting The Diagnostic Yield of Flexible Bronchoscopy Without Guidance in Pulmonary Nodules or MassesXaralyn XaviereNo ratings yet
- Ecografia Toracica PDFDocument12 pagesEcografia Toracica PDFCristinaLucanNo ratings yet
- Transsphenoidal Hypophysectomy:: Postsurgical CT FindingsDocument6 pagesTranssphenoidal Hypophysectomy:: Postsurgical CT FindingsnurNo ratings yet
- The Alung Pointo An Ultrasound Sign Specific To PneumothoraxDocument7 pagesThe Alung Pointo An Ultrasound Sign Specific To PneumothoraxnuelitopNo ratings yet
- Value of Lung Biopsy Lung: Tru-Cut in Focal and DiffuseDocument4 pagesValue of Lung Biopsy Lung: Tru-Cut in Focal and DiffuseGargNo ratings yet
- Fluorescence Lifetime Imaging OphthalmoscopyFrom EverandFluorescence Lifetime Imaging OphthalmoscopyMartin ZinkernagelNo ratings yet
- Nejmoa 1912035Document11 pagesNejmoa 1912035Subhashini KNo ratings yet
- Dipsi 2022 Sci Pro 1Document2 pagesDipsi 2022 Sci Pro 1Subhashini KNo ratings yet
- Trichy Hotel LinkDocument1 pageTrichy Hotel LinkSubhashini KNo ratings yet
- JAPI0073 p84-88Document5 pagesJAPI0073 p84-88Subhashini KNo ratings yet
- Tri Fascicular BlockDocument28 pagesTri Fascicular BlockSubhashini KNo ratings yet
- LabRepo ShareDocument4 pagesLabRepo ShareSubhashini KNo ratings yet
- Endovascular Therapy For Acute Stroke With A Large Ischemic Region NEJMDocument21 pagesEndovascular Therapy For Acute Stroke With A Large Ischemic Region NEJMSubhashini KNo ratings yet
- Invitation New-2Document2 pagesInvitation New-2Subhashini KNo ratings yet
- Med Cme InviteDocument2 pagesMed Cme InviteSubhashini KNo ratings yet
- SEX DifferencesDocument12 pagesSEX DifferencesSubhashini KNo ratings yet
- Nuestra Healthcare ProductsDocument16 pagesNuestra Healthcare ProductsNuestra HealthcareNo ratings yet
- Different Field of Nursing: Geronimo C. Burce JRDocument44 pagesDifferent Field of Nursing: Geronimo C. Burce JRBiway RegalaNo ratings yet
- Punitive, Restorative, and Transformative JusticeDocument4 pagesPunitive, Restorative, and Transformative JusticeMonkey DLuffyyyNo ratings yet
- Hernandez Et Al 2016Document23 pagesHernandez Et Al 2016Carolina JiménezNo ratings yet
- University of Nebraska Press The Settler SeaDocument29 pagesUniversity of Nebraska Press The Settler SeaCalibán CatrileoNo ratings yet
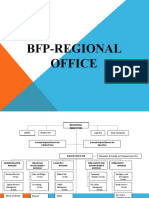
- OS For BFP Regional OfficeDocument23 pagesOS For BFP Regional OfficeJustine Paulo ManuelNo ratings yet
- Khalil Ur Rehman: Carrier Objective Accomplishment/StrengthDocument5 pagesKhalil Ur Rehman: Carrier Objective Accomplishment/StrengthHabib ur rahmanNo ratings yet
- WWW BarcaiDocument9 pagesWWW BarcaiOlena BaevaNo ratings yet
- Guava Tea Leaves: July 2020Document8 pagesGuava Tea Leaves: July 2020Indra D KristionoNo ratings yet
- Pacific Cross - 2020-10 (October 01)Document12 pagesPacific Cross - 2020-10 (October 01)Eeza OrtileNo ratings yet
- Patient Monitoring Systems: Suneetha.G Synergy Business SchoolDocument23 pagesPatient Monitoring Systems: Suneetha.G Synergy Business SchoolUsman NaeemNo ratings yet
- Latest Additions - Books June, 2018: SL - No Sub Code Author Title Ed Year 1Document1 pageLatest Additions - Books June, 2018: SL - No Sub Code Author Title Ed Year 1pavans25No ratings yet
- Vit D DeficiencyDocument6 pagesVit D DeficiencySimplicia Maria AnggrahiniNo ratings yet
- Cleaning The Delivery Room - EquipmentsDocument7 pagesCleaning The Delivery Room - EquipmentsAnne BasilesNo ratings yet
- IA1 - Mock AssessmentDocument3 pagesIA1 - Mock AssessmentMohammad Mokhtarul HaqueNo ratings yet
- PPH CasestudyDocument45 pagesPPH CasestudyRona Mae PangilinanNo ratings yet
- Challenges/: EpistemeDocument28 pagesChallenges/: EpistemeKádár BiancaNo ratings yet
- Safety Plan: An Instruction ManualDocument3 pagesSafety Plan: An Instruction ManualJNo ratings yet
- Tubing Installation ProcedureDocument4 pagesTubing Installation ProcedurePutraArifWardhanaNo ratings yet
- كتالوج الأجهزة الطبيةDocument8 pagesكتالوج الأجهزة الطبيةIslam HosniNo ratings yet
- Organic Pharmaceutical ChemistryDocument25 pagesOrganic Pharmaceutical Chemistryiamarrhinne100% (1)
- Vereena Bishoy Second Draft ScriptDocument2 pagesVereena Bishoy Second Draft Scriptapi-532074601No ratings yet
- Cebu City Medical Center-College of NursingDocument18 pagesCebu City Medical Center-College of NursingRogerQuxNo ratings yet
- Hazard and Risk Identification Competency Quiz 2.0Document6 pagesHazard and Risk Identification Competency Quiz 2.0Edgardo AmadorNo ratings yet
- Boiler Inspection PDFDocument2 pagesBoiler Inspection PDFsajuhereNo ratings yet
- Classification Essay Thesis StatementDocument8 pagesClassification Essay Thesis Statementezmbzw42100% (2)
































































































Download as pptx, pdf, or txt
You might also like
- Chicken Nutrition - A Guide For Nutritionists and Poultry ProfessionalsDocument23 pagesChicken Nutrition - A Guide For Nutritionists and Poultry Professionalsronx0% (1)
- Psychiatric Case StudyDocument32 pagesPsychiatric Case Studyrachael86% (35)
- Provide Support To People Living With DementiaDocument9 pagesProvide Support To People Living With DementiaGurpreet Singh WirringNo ratings yet
- 9.interstitial Lung DiseasesDocument4 pages9.interstitial Lung DiseasesLankeshwaraNo ratings yet
- (2018) - Flujo Inspiratorio Máximo Como Predictor de Traqueotomía.Document4 pages(2018) - Flujo Inspiratorio Máximo Como Predictor de Traqueotomía.luribe662No ratings yet
- 1 s2.0 S0899707122000298 MainDocument12 pages1 s2.0 S0899707122000298 Mainrivai anwarNo ratings yet
- Rosette Forming Glioneuronal Tumor (RFGNT) Extremely Rare Entity - CopieDocument16 pagesRosette Forming Glioneuronal Tumor (RFGNT) Extremely Rare Entity - CopieCalin M.No ratings yet
- Difficulties Diagnosing Ipf - Simon WalshDocument95 pagesDifficulties Diagnosing Ipf - Simon WalshcuvinhNo ratings yet
- Idiopathic Pulmonary Fibrosis NEWDocument34 pagesIdiopathic Pulmonary Fibrosis NEWrahayuNo ratings yet
- Lung Lobe Torsion in 15 Dogs - Peripheral Band Sign On UltrasoundDocument10 pagesLung Lobe Torsion in 15 Dogs - Peripheral Band Sign On UltrasoundAdan Camilo Ramirez CarranzaNo ratings yet
- 920 FullDocument17 pages920 FullHeru SigitNo ratings yet
- Postgraduate Course 3 Radiological-Pathological Correlation of Tumoural and Non-Tumoural Pathology: An Interdisciplinary ApproachDocument31 pagesPostgraduate Course 3 Radiological-Pathological Correlation of Tumoural and Non-Tumoural Pathology: An Interdisciplinary ApproachBulborea MihaelaNo ratings yet
- 2015 Chest - Blue & Falls ProtocolsDocument12 pages2015 Chest - Blue & Falls ProtocolsWilmer Yanquen VillarrealNo ratings yet
- BLUE-Protocol and FALLS-Protocol: Two Applications of Lung Ultrasound in The Critically IllDocument12 pagesBLUE-Protocol and FALLS-Protocol: Two Applications of Lung Ultrasound in The Critically IllChristiaan CordovaNo ratings yet
- BLUE & FALLS Protocol LichensteinDocument12 pagesBLUE & FALLS Protocol LichensteinCarlos MoncayoNo ratings yet
- Ipf UipDocument39 pagesIpf UipSai Nandan ReddyNo ratings yet
- Ipaf 2019 CCM - 230215 - 064414Document9 pagesIpaf 2019 CCM - 230215 - 064414Robert Arana NarváezNo ratings yet
- Edoskopi FleksibelDocument4 pagesEdoskopi FleksibelDex RayNo ratings yet
- DR Oea KhairsyafDocument30 pagesDR Oea KhairsyafErdyNo ratings yet
- Cherian2019 PDFDocument23 pagesCherian2019 PDFnugra raturandangNo ratings yet
- CT Features of Community-Acquired Pneumonia at The Emergency DepartmentDocument8 pagesCT Features of Community-Acquired Pneumonia at The Emergency DepartmentpachomdNo ratings yet
- WCS 015 - Shortness of Breath in A Construction Site Worker - Occupational Lung Diseases - Pulmonary Fibrosis - Workman's Compensation by DR DCL LamDocument60 pagesWCS 015 - Shortness of Breath in A Construction Site Worker - Occupational Lung Diseases - Pulmonary Fibrosis - Workman's Compensation by DR DCL LamJenniferFooNo ratings yet
- Bronquiolite DiagnosticoDocument14 pagesBronquiolite DiagnosticoFrederico PóvoaNo ratings yet
- CPC Interventional RadiologyDocument138 pagesCPC Interventional RadiologyEbrahim Adel Ali AhmedNo ratings yet
- 65364a4a96254 IJAR-44785Document6 pages65364a4a96254 IJAR-44785asrindustriesisavailableNo ratings yet
- Jrcollphyslond146949 0029bDocument7 pagesJrcollphyslond146949 0029bArun JadhavNo ratings yet
- Hypersensitivity Pneumonitis: Diagnostic and Therapeutic ChallengesDocument51 pagesHypersensitivity Pneumonitis: Diagnostic and Therapeutic ChallengesskchhabraNo ratings yet
- Hypersensitivity Pneumonitis: Diagnostic and Therapeutic ChallengesDocument51 pagesHypersensitivity Pneumonitis: Diagnostic and Therapeutic ChallengesskchhabraNo ratings yet
- Routine Use of Point-of-Care Lung Ultrasound During The COVID-19 PandemicDocument4 pagesRoutine Use of Point-of-Care Lung Ultrasound During The COVID-19 PandemicOswaldo MontesNo ratings yet
- Uip and NsipDocument38 pagesUip and NsipReem AbbasNo ratings yet
- Wang 2017Document9 pagesWang 2017juanrangoneNo ratings yet
- BSTI COVID-19 Radiology Guidance Version 2 16.03.20 PDFDocument28 pagesBSTI COVID-19 Radiology Guidance Version 2 16.03.20 PDFAlejandro RojasNo ratings yet
- Interventional Radiology: A Manual For Surgeons and RadiologistsDocument24 pagesInterventional Radiology: A Manual For Surgeons and RadiologistsMaria KristinaNo ratings yet
- ENT Lecture FinalDocument65 pagesENT Lecture FinalNejib M/AminNo ratings yet
- BLUE-Protocol and FALLS-ProtocolDocument12 pagesBLUE-Protocol and FALLS-ProtocolChris Vam SanchezNo ratings yet
- Ijcmr 2324 v1 1Document6 pagesIjcmr 2324 v1 1ahsaanillahi9No ratings yet
- Organizing Pneumonia: Chest HRCT Findings : Pneumonia em Organização: Achados Da TCAR de TóraxDocument7 pagesOrganizing Pneumonia: Chest HRCT Findings : Pneumonia em Organização: Achados Da TCAR de TóraxPutra PratamaNo ratings yet
- Arya - Usefulness and Safety of Transbronchial Biopsy With Large Forceps During Flexible BronchosDocument5 pagesArya - Usefulness and Safety of Transbronchial Biopsy With Large Forceps During Flexible BronchosXaralyn XaviereNo ratings yet
- Andronik Ou 2013Document16 pagesAndronik Ou 2013MayNo ratings yet
- 2008 Chest - The Blue ProtocolDocument9 pages2008 Chest - The Blue Protocoleduardo0% (1)
- Ryct 2021200279Document19 pagesRyct 2021200279Andiie ResminNo ratings yet
- Radiology RoundsDocument30 pagesRadiology RoundsKelum BuddhikaNo ratings yet
- 2.significance of Fuchs Flecks in Patients With Pterygium Loght DamageDocument4 pages2.significance of Fuchs Flecks in Patients With Pterygium Loght DamagedelaNo ratings yet
- Focus: NeurosurgicalDocument7 pagesFocus: NeurosurgicalGaetano De BiaseNo ratings yet
- Ild Cme SlidesDocument93 pagesIld Cme SlidesJagbir Singh KanetNo ratings yet
- Can Malignant and Benign Pulmonary Nodules Be Differentiated With Diffusion-Weighted MRI?Document7 pagesCan Malignant and Benign Pulmonary Nodules Be Differentiated With Diffusion-Weighted MRI?Patta DaengNo ratings yet
- Thoracic Ultrasonography A Narrative ReviewDocument12 pagesThoracic Ultrasonography A Narrative ReviewJHONATAN MATA ARANDANo ratings yet
- Final PFT Day 1Document11 pagesFinal PFT Day 1Quevee CondezNo ratings yet
- Anesthesia Considerations in Microlaryngoscopy or Direct LaryngosDocument6 pagesAnesthesia Considerations in Microlaryngoscopy or Direct LaryngosRubén Darío HerediaNo ratings yet
- Clinical Practice GuidelinesDocument3 pagesClinical Practice GuidelinessigitNo ratings yet
- Respirology - 2011 - KOEGELENBERG - Pleural Controversy Closed Needle Pleural Biopsy or Thoracoscopy Which FirstDocument9 pagesRespirology - 2011 - KOEGELENBERG - Pleural Controversy Closed Needle Pleural Biopsy or Thoracoscopy Which Firstdalozpa23No ratings yet
- Lipoma of The Parotid Gland Extending From The Superficial To The Deep Lobe Case ReportDocument4 pagesLipoma of The Parotid Gland Extending From The Superficial To The Deep Lobe Case ReportHerald Scholarly Open AccessNo ratings yet
- 865 FullDocument16 pages865 Fullaieyha hamkaNo ratings yet
- Jurnal Radio Inggris TalDocument17 pagesJurnal Radio Inggris TalimamattamamiNo ratings yet
- Plain Film and HRCT Diagnosis of Interstitial Lung Disease: Sujal R. Desai, Helmut Prosch, and Jeffrey R. GalvinDocument9 pagesPlain Film and HRCT Diagnosis of Interstitial Lung Disease: Sujal R. Desai, Helmut Prosch, and Jeffrey R. GalvinVictor ChiabaiNo ratings yet
- Idiopathic Pulmonary Fibrosis: Diagnosis, Epidemiology and Natural HistoryDocument11 pagesIdiopathic Pulmonary Fibrosis: Diagnosis, Epidemiology and Natural HistorySuwandi AlghozyNo ratings yet
- Boonsarngsuk - Factors Affecting The Diagnostic Yield of Flexible Bronchoscopy Without Guidance in Pulmonary Nodules or MassesDocument6 pagesBoonsarngsuk - Factors Affecting The Diagnostic Yield of Flexible Bronchoscopy Without Guidance in Pulmonary Nodules or MassesXaralyn XaviereNo ratings yet
- Ecografia Toracica PDFDocument12 pagesEcografia Toracica PDFCristinaLucanNo ratings yet
- Transsphenoidal Hypophysectomy:: Postsurgical CT FindingsDocument6 pagesTranssphenoidal Hypophysectomy:: Postsurgical CT FindingsnurNo ratings yet
- The Alung Pointo An Ultrasound Sign Specific To PneumothoraxDocument7 pagesThe Alung Pointo An Ultrasound Sign Specific To PneumothoraxnuelitopNo ratings yet
- Value of Lung Biopsy Lung: Tru-Cut in Focal and DiffuseDocument4 pagesValue of Lung Biopsy Lung: Tru-Cut in Focal and DiffuseGargNo ratings yet
- Fluorescence Lifetime Imaging OphthalmoscopyFrom EverandFluorescence Lifetime Imaging OphthalmoscopyMartin ZinkernagelNo ratings yet
- Nejmoa 1912035Document11 pagesNejmoa 1912035Subhashini KNo ratings yet
- Dipsi 2022 Sci Pro 1Document2 pagesDipsi 2022 Sci Pro 1Subhashini KNo ratings yet
- Trichy Hotel LinkDocument1 pageTrichy Hotel LinkSubhashini KNo ratings yet
- JAPI0073 p84-88Document5 pagesJAPI0073 p84-88Subhashini KNo ratings yet
- Tri Fascicular BlockDocument28 pagesTri Fascicular BlockSubhashini KNo ratings yet
- LabRepo ShareDocument4 pagesLabRepo ShareSubhashini KNo ratings yet
- Endovascular Therapy For Acute Stroke With A Large Ischemic Region NEJMDocument21 pagesEndovascular Therapy For Acute Stroke With A Large Ischemic Region NEJMSubhashini KNo ratings yet
- Invitation New-2Document2 pagesInvitation New-2Subhashini KNo ratings yet
- Med Cme InviteDocument2 pagesMed Cme InviteSubhashini KNo ratings yet
- SEX DifferencesDocument12 pagesSEX DifferencesSubhashini KNo ratings yet
- Nuestra Healthcare ProductsDocument16 pagesNuestra Healthcare ProductsNuestra HealthcareNo ratings yet
- Different Field of Nursing: Geronimo C. Burce JRDocument44 pagesDifferent Field of Nursing: Geronimo C. Burce JRBiway RegalaNo ratings yet
- Punitive, Restorative, and Transformative JusticeDocument4 pagesPunitive, Restorative, and Transformative JusticeMonkey DLuffyyyNo ratings yet
- Hernandez Et Al 2016Document23 pagesHernandez Et Al 2016Carolina JiménezNo ratings yet
- University of Nebraska Press The Settler SeaDocument29 pagesUniversity of Nebraska Press The Settler SeaCalibán CatrileoNo ratings yet
- OS For BFP Regional OfficeDocument23 pagesOS For BFP Regional OfficeJustine Paulo ManuelNo ratings yet
- Khalil Ur Rehman: Carrier Objective Accomplishment/StrengthDocument5 pagesKhalil Ur Rehman: Carrier Objective Accomplishment/StrengthHabib ur rahmanNo ratings yet
- WWW BarcaiDocument9 pagesWWW BarcaiOlena BaevaNo ratings yet
- Guava Tea Leaves: July 2020Document8 pagesGuava Tea Leaves: July 2020Indra D KristionoNo ratings yet
- Pacific Cross - 2020-10 (October 01)Document12 pagesPacific Cross - 2020-10 (October 01)Eeza OrtileNo ratings yet
- Patient Monitoring Systems: Suneetha.G Synergy Business SchoolDocument23 pagesPatient Monitoring Systems: Suneetha.G Synergy Business SchoolUsman NaeemNo ratings yet
- Latest Additions - Books June, 2018: SL - No Sub Code Author Title Ed Year 1Document1 pageLatest Additions - Books June, 2018: SL - No Sub Code Author Title Ed Year 1pavans25No ratings yet
- Vit D DeficiencyDocument6 pagesVit D DeficiencySimplicia Maria AnggrahiniNo ratings yet
- Cleaning The Delivery Room - EquipmentsDocument7 pagesCleaning The Delivery Room - EquipmentsAnne BasilesNo ratings yet
- IA1 - Mock AssessmentDocument3 pagesIA1 - Mock AssessmentMohammad Mokhtarul HaqueNo ratings yet
- PPH CasestudyDocument45 pagesPPH CasestudyRona Mae PangilinanNo ratings yet
- Challenges/: EpistemeDocument28 pagesChallenges/: EpistemeKádár BiancaNo ratings yet
- Safety Plan: An Instruction ManualDocument3 pagesSafety Plan: An Instruction ManualJNo ratings yet
- Tubing Installation ProcedureDocument4 pagesTubing Installation ProcedurePutraArifWardhanaNo ratings yet
- كتالوج الأجهزة الطبيةDocument8 pagesكتالوج الأجهزة الطبيةIslam HosniNo ratings yet
- Organic Pharmaceutical ChemistryDocument25 pagesOrganic Pharmaceutical Chemistryiamarrhinne100% (1)
- Vereena Bishoy Second Draft ScriptDocument2 pagesVereena Bishoy Second Draft Scriptapi-532074601No ratings yet
- Cebu City Medical Center-College of NursingDocument18 pagesCebu City Medical Center-College of NursingRogerQuxNo ratings yet
- Hazard and Risk Identification Competency Quiz 2.0Document6 pagesHazard and Risk Identification Competency Quiz 2.0Edgardo AmadorNo ratings yet
- Boiler Inspection PDFDocument2 pagesBoiler Inspection PDFsajuhereNo ratings yet
- Classification Essay Thesis StatementDocument8 pagesClassification Essay Thesis Statementezmbzw42100% (2)