Download as pptx, pdf, or txt
You might also like
- Baseline Discrimagon User ManualDocument2 pagesBaseline Discrimagon User ManualphcproductsNo ratings yet
- Clinical Face Sheet: G3P2, Pregnancy Uterine (PU), 37 Weeks and 5 Days AOG, Previous CS IIDocument14 pagesClinical Face Sheet: G3P2, Pregnancy Uterine (PU), 37 Weeks and 5 Days AOG, Previous CS IICezanne CruzNo ratings yet
- Antiplateletdrugs 150203231404 Conversion Gate01 PDFDocument67 pagesAntiplateletdrugs 150203231404 Conversion Gate01 PDFAndrie WigunaNo ratings yet
- Principles of An-Tiplatelet Therapy: DR Htet Htet Htethtet@Imu - Edu.MyDocument36 pagesPrinciples of An-Tiplatelet Therapy: DR Htet Htet Htethtet@Imu - Edu.MyAbby LiewNo ratings yet
- Principles of Antiplatelet Therapy: DR Htet Htet Htethtet@Imu - Edu.MyDocument36 pagesPrinciples of Antiplatelet Therapy: DR Htet Htet Htethtet@Imu - Edu.MyAbby Liew100% (1)
- Anticlotting DrugsDocument70 pagesAnticlotting DrugsZaina Masri100% (1)
- DR - Hussam Lec 3 Drugs Affecting Blood 2023 4Document13 pagesDR - Hussam Lec 3 Drugs Affecting Blood 2023 4ManWol JangNo ratings yet
- 9 - Anti-Platelet DrugsDocument12 pages9 - Anti-Platelet DrugsGoodone OneNo ratings yet
- Contraindications To Thrombolytic Therapy: Aminocaproic AcidDocument3 pagesContraindications To Thrombolytic Therapy: Aminocaproic AcidTia Siti RoilaNo ratings yet
- Antiplatelet Drugs: Dr. Chandane R. DDocument34 pagesAntiplatelet Drugs: Dr. Chandane R. Dabdul razakNo ratings yet
- Antiplatelet, Anticoagulant and Thrombolytic Agents: Basic Pharmacology Block Pdnt/Pmed - PMSC/PPHR - 213Document30 pagesAntiplatelet, Anticoagulant and Thrombolytic Agents: Basic Pharmacology Block Pdnt/Pmed - PMSC/PPHR - 213JedoNo ratings yet
- Drug Used in Coagulation-Bleeding Disorders Updated (2) RegnerDocument92 pagesDrug Used in Coagulation-Bleeding Disorders Updated (2) RegnerDR. MUSICNo ratings yet
- Fibrinolytic and Antiplatelet Drugs 2020 BDS BSCN Online (Compatibility Mode)Document7 pagesFibrinolytic and Antiplatelet Drugs 2020 BDS BSCN Online (Compatibility Mode)ireneNo ratings yet
- Anticoagulacion 2Document9 pagesAnticoagulacion 2Annette ChavezNo ratings yet
- 9 Anti PlateletDocument15 pages9 Anti PlateletHely PatelNo ratings yet
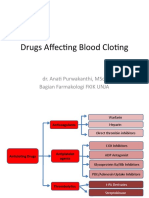
- Drugs Affecting Blood Cloting 2019Document39 pagesDrugs Affecting Blood Cloting 2019Mutiara RizkiNo ratings yet
- Drug InteractionsDocument16 pagesDrug InteractionsYvetal GardeNo ratings yet
- Anticoagulants DrugsDocument6 pagesAnticoagulants DrugsHusam Al-OdatNo ratings yet
- PAIN ControllersDocument39 pagesPAIN ControllersAyro Business CenterNo ratings yet
- Antiplatelet DrugsDocument15 pagesAntiplatelet Drugsngan321100% (1)
- AnticoagulantsDocument47 pagesAnticoagulantsKeerthana KNo ratings yet
- Hematology Unit: Dr. Furqan HashmiDocument32 pagesHematology Unit: Dr. Furqan HashmiabubakarNo ratings yet
- Coagulation DisorderDocument38 pagesCoagulation DisorderTsegaye HailuNo ratings yet
- Cardiovascular PharmacologyDocument61 pagesCardiovascular PharmacologyTeeOne920% (1)
- Pertemuan 7 LiyanaDocument36 pagesPertemuan 7 LiyanaLiyana SafitriNo ratings yet
- 14 BloodDocument32 pages14 Bloodنور الإسلامNo ratings yet
- Drugs: 1-The Mechanism of Action of ASADocument11 pagesDrugs: 1-The Mechanism of Action of ASAVgdgNo ratings yet
- Anticoagulants, Thrombolytics and AntiplateletDocument57 pagesAnticoagulants, Thrombolytics and AntiplateletEsther Agustin100% (1)
- Inotropes, Excellent Article, With DosingDocument47 pagesInotropes, Excellent Article, With DosingNavojit ChowdhuryNo ratings yet
- 18.fibrinolytic (Thrombolytic) AgentsDocument42 pages18.fibrinolytic (Thrombolytic) AgentsAstha ShresthaNo ratings yet
- Pharma DR - Hussein Drugs Effecting Hemostasis Lec 1Document31 pagesPharma DR - Hussein Drugs Effecting Hemostasis Lec 1rkh647m7szNo ratings yet
- Lecture 6 Pharma DR N AlhasaniDocument9 pagesLecture 6 Pharma DR N Alhasanialialahmedy24No ratings yet
- Antiplatelet, Thrombolitik, Antikoagulan, Vasodilator Referat VaskularDocument23 pagesAntiplatelet, Thrombolitik, Antikoagulan, Vasodilator Referat Vaskularmonyet65No ratings yet
- Drugs FinalDocument5 pagesDrugs FinalmekeeeNo ratings yet
- Katzung 11th - Antiagregantes PlaquetáriosDocument2 pagesKatzung 11th - Antiagregantes PlaquetáriosJoana NunesNo ratings yet
- Antianginal DrugsDocument36 pagesAntianginal DrugscreativejoburgNo ratings yet
- Anticoagulation Module 2Document13 pagesAnticoagulation Module 2angelmedurNo ratings yet
- Fibrinolytics, Anti Fibrinolytics and Anti Platelets: Dr. B.K.Bezbaruah Professor Pharmacology Gauhati Medical CollegeDocument46 pagesFibrinolytics, Anti Fibrinolytics and Anti Platelets: Dr. B.K.Bezbaruah Professor Pharmacology Gauhati Medical CollegeBidyut BanerjeeNo ratings yet
- Antipatelet Drug TherapyDocument6 pagesAntipatelet Drug TherapySayali KhandaleNo ratings yet
- Antiplatelet DrugsDocument31 pagesAntiplatelet DrugsSyed Usama Rashid100% (2)
- Immuno-Suppressants: Dr. PrasadDocument21 pagesImmuno-Suppressants: Dr. PrasadMuskaan ZaharaNo ratings yet
- Genetic Implications Pregnancy CategoryDocument4 pagesGenetic Implications Pregnancy CategoryElizabeth LevitskyNo ratings yet
- Blood Drugs-WPS OfficeDocument15 pagesBlood Drugs-WPS OfficeRubabNo ratings yet
- Anticoagulants, Fibrinolytics, AntiplateletsDocument88 pagesAnticoagulants, Fibrinolytics, Antiplateletspmuawiyah25No ratings yet
- Neuropharma AntidementiaDocument29 pagesNeuropharma AntidementiaKeanne Paula AmamanglonNo ratings yet
- #06-Cholinoceptor-Activating-Cholinesterase-Inh-Drugs - v2Document66 pages#06-Cholinoceptor-Activating-Cholinesterase-Inh-Drugs - v2tasnemaldaherNo ratings yet
- Vasodil - Ischemic Heart DiseaseDocument52 pagesVasodil - Ischemic Heart DiseaseNorms YoramNo ratings yet
- Anticoagulant Powerpoint PresentationsDocument60 pagesAnticoagulant Powerpoint PresentationsREETHUNo ratings yet
- AnticoagulantDocument34 pagesAnticoagulantTasya FakhiraNo ratings yet
- منار كمDocument61 pagesمنار كمFemale calmNo ratings yet
- AntitrombolitikDocument7 pagesAntitrombolitikadityaNo ratings yet
- DRUG STUDY - Rosalinda FerrerDocument6 pagesDRUG STUDY - Rosalinda Ferrer40-GALOLO ANDREA PAULINENo ratings yet
- Cardiovasculr PGX StudentsDocument55 pagesCardiovasculr PGX StudentsHashem KarakyNo ratings yet
- Obat Sistem HematologiDocument21 pagesObat Sistem HematologiSuryana AdityaNo ratings yet
- Anti PlateletsDocument49 pagesAnti Plateletsrsharifa00No ratings yet
- New Drugs and Technologies: PrasugrelDocument10 pagesNew Drugs and Technologies: PrasugrelDewi FitrianaNo ratings yet
- Coagulation Related DrugsDocument20 pagesCoagulation Related DrugsshehranNo ratings yet
- John Hommer E. Dy, MD.: Diplomate in Internal MedicineDocument56 pagesJohn Hommer E. Dy, MD.: Diplomate in Internal MedicinehommercuteNo ratings yet
- Topic HemostasisDocument10 pagesTopic HemostasisFatemeh EshaghizadehNo ratings yet
- Drug - Nephrotoxicity - Dec - 2013.ppt FinalDocument27 pagesDrug - Nephrotoxicity - Dec - 2013.ppt FinalMaydhista PoetriNo ratings yet
- BloodDocument32 pagesBloodYohannes MeridNo ratings yet
- Plasma ProteinsDocument51 pagesPlasma ProteinsYohannes MeridNo ratings yet
- RBC Disorders 2019 - 190619134512Document217 pagesRBC Disorders 2019 - 190619134512Yohannes MeridNo ratings yet
- CH - 4 Mix and Yield Variance Ahmed FinalDocument8 pagesCH - 4 Mix and Yield Variance Ahmed FinalYohannes MeridNo ratings yet
- Anti-Anemic Drugs - 210619200800Document40 pagesAnti-Anemic Drugs - 210619200800Yohannes MeridNo ratings yet
- CH - 2 Master Budget - Ahmed With Illustration and SolutionDocument15 pagesCH - 2 Master Budget - Ahmed With Illustration and SolutionYohannes MeridNo ratings yet
- CH - 1 CVP Analysis - AhmedDocument8 pagesCH - 1 CVP Analysis - AhmedYohannes MeridNo ratings yet
- A Study On Impact of Acne Vulgaris On Quality of LifeDocument7 pagesA Study On Impact of Acne Vulgaris On Quality of LifeIJAR JOURNALNo ratings yet
- Cochlear-Implants Brochure 2Document2 pagesCochlear-Implants Brochure 2roroNo ratings yet
- Tuberculin Skin TestDocument2 pagesTuberculin Skin Testcalmira3653No ratings yet
- Hadpsar List Corentine 25.03.20Document10 pagesHadpsar List Corentine 25.03.20snagoorNo ratings yet
- NCP Self Care DeficitDocument15 pagesNCP Self Care DeficitSkye M. PetersNo ratings yet
- Tyrosinemia Type 1Document8 pagesTyrosinemia Type 1Muhammad LawalNo ratings yet
- Antibiotic Selection GuideDocument37 pagesAntibiotic Selection GuideAbanoub Nabil100% (1)
- Obat UperioDocument5 pagesObat UperioAnonymous Aa6VAStNo ratings yet
- Case Study On: Importance of Mission IndradhanushDocument9 pagesCase Study On: Importance of Mission IndradhanushRohit RaneNo ratings yet
- ElectrocardiographyDocument29 pagesElectrocardiographyJhevey ValdezNo ratings yet
- Andi Muh. Octavian Pratama Et Anwar Lewa-1Document9 pagesAndi Muh. Octavian Pratama Et Anwar Lewa-1octavian pratamaNo ratings yet
- Duodenal Perforation During Intubation For Small Bowel Enema Study'Document3 pagesDuodenal Perforation During Intubation For Small Bowel Enema Study'manishbabuNo ratings yet
- General AnesthesiaDocument58 pagesGeneral AnesthesiaAli Mohamed100% (1)
- Example Health Promotion ProjectDocument10 pagesExample Health Promotion ProjectLibbyNo ratings yet
- Rifaximin Therapy For Patients With IrritableDocument18 pagesRifaximin Therapy For Patients With IrritableSalman AjaNo ratings yet
- Bachelor of Science in Nursing: Care of Mother and Child and AdolescentDocument12 pagesBachelor of Science in Nursing: Care of Mother and Child and AdolescentJaja ManezNo ratings yet
- Solanum - Zombiepedia - FandomDocument5 pagesSolanum - Zombiepedia - FandomJohn SutphinNo ratings yet
- Enrichment Activities C1: Grade Level: Six Quarter: First Subject: MAPEH-HealthDocument11 pagesEnrichment Activities C1: Grade Level: Six Quarter: First Subject: MAPEH-HealthARLENE MARASIGAN100% (1)
- Reading 5 Blood and Body DefensesDocument18 pagesReading 5 Blood and Body Defenseslephuongvy1406No ratings yet
- Hipoxemia RefratariaDocument4 pagesHipoxemia RefratariaThiago LacerdaNo ratings yet
- GROUP F Compilation PsychiaFinalDocument20 pagesGROUP F Compilation PsychiaFinalFrancis Raphael PitogoNo ratings yet
- History of Present IllnessDocument4 pagesHistory of Present Illnessegabe386No ratings yet
- The Bigger The Bulge The Better - Rayner & Smale PDFDocument4 pagesThe Bigger The Bulge The Better - Rayner & Smale PDFItai IzhakNo ratings yet
- Duttons Introductory Skills and Procedures For The Physical Therapist Assistant 1St Edition Mark Dutton Full ChapterDocument51 pagesDuttons Introductory Skills and Procedures For The Physical Therapist Assistant 1St Edition Mark Dutton Full Chaptersusie.blankenship630100% (6)
- Management TB MOH Singapore PDFDocument123 pagesManagement TB MOH Singapore PDFLindsley GruvyNo ratings yet
- Chapter 5: Radiological Anatomy: General AspectsDocument7 pagesChapter 5: Radiological Anatomy: General AspectsYel YuriNo ratings yet
- RX - Citicoline, Kalium, Ketosteril, Methycobal, Myonal, Lipolin GelDocument6 pagesRX - Citicoline, Kalium, Ketosteril, Methycobal, Myonal, Lipolin GelntootNo ratings yet
- Circulatory System: DR Rita Chávez Puente Cie-MgaDocument22 pagesCirculatory System: DR Rita Chávez Puente Cie-Mgarchavez0522No ratings yet