Download as ppt, pdf, or txt
You might also like
- Pharmacology UNIT 1 - Lesson 1Document29 pagesPharmacology UNIT 1 - Lesson 1Bea Bianca CruzNo ratings yet
- A Century of Public Health in The PhilippinesDocument23 pagesA Century of Public Health in The PhilippinesCherryl Surigao100% (2)
- IMS Hospital Supply IndexDocument2 pagesIMS Hospital Supply Indexmochkurniawan0% (1)
- 2015 ESC-ERS Gles PH-Web Addenda-Ehv317Document8 pages2015 ESC-ERS Gles PH-Web Addenda-Ehv317Georgiana ArtenieNo ratings yet
- PharmacologyDocument7 pagesPharmacologyscjkyd5cvrNo ratings yet
- AmiodaroneDocument10 pagesAmiodaronesarahhhNo ratings yet
- Drugs Acting On Potassium Channel: Submitted By: Md. Ashikur Rahman ID: 171-021-032Document12 pagesDrugs Acting On Potassium Channel: Submitted By: Md. Ashikur Rahman ID: 171-021-032broken reedNo ratings yet
- Amiodarone Hydrochloride in JDocument18 pagesAmiodarone Hydrochloride in JChrizzna HaryantoNo ratings yet
- Amiodarone Guideline For Use and MonitoringDocument8 pagesAmiodarone Guideline For Use and MonitoringTania NicolaescuNo ratings yet
- Cordarone® and Cordarone® X Tablets - PIDocument11 pagesCordarone® and Cordarone® X Tablets - PIdkjoshiameNo ratings yet
- PASSMEDICINE MCQs-PHARMACOLOGYDocument107 pagesPASSMEDICINE MCQs-PHARMACOLOGYMohammad Saleh100% (1)
- AmiodaroneDocument9 pagesAmiodaroneJonathan Ian ArinsolNo ratings yet
- Anti AritmiaDocument27 pagesAnti AritmiadoraemonmayaNo ratings yet
- Cardiac ArrhythmiaDocument101 pagesCardiac ArrhythmiaYuvraj ChauhanNo ratings yet
- Initial Treatment: Special WarningsDocument10 pagesInitial Treatment: Special Warningsddandan_2No ratings yet
- Antiarrhythmic AgentsDocument45 pagesAntiarrhythmic AgentsSoh Kae SiangNo ratings yet
- Amiodarona - Monitorizare, Reactii Adverse - Ghid American 2003Document8 pagesAmiodarona - Monitorizare, Reactii Adverse - Ghid American 2003Madalina BadeaNo ratings yet
- Amiodarone InjDocument2 pagesAmiodarone InjasdwasdNo ratings yet
- Antiarrhythmic DrugsDocument21 pagesAntiarrhythmic DrugsShoeb Nawaz Khan100% (1)
- Antiarrhythmic DrugsDocument17 pagesAntiarrhythmic DrugsTarek G MustafaNo ratings yet
- Motilium: ® Domperidone DatasheetDocument11 pagesMotilium: ® Domperidone DatasheetAurungzaib BhattiNo ratings yet
- Diskusi Topik Anestesi GamaDocument65 pagesDiskusi Topik Anestesi Gamakusumagama28No ratings yet
- Amiodarone Guidelines For Use and Monitoring - American Family PhysicianDocument1 pageAmiodarone Guidelines For Use and Monitoring - American Family PhysicianAdinda DianNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Treatment of Tachyarrhythmias1Document1 pageTreatment of Tachyarrhythmias1Falaq2No ratings yet
- 2012AGSBeersCriteriaCitations PDFDocument14 pages2012AGSBeersCriteriaCitations PDFnegarayeniNo ratings yet
- Amiodarone Guia Clinica para Su UsoDocument10 pagesAmiodarone Guia Clinica para Su UsoARTURO YOSHIMAR LUQUE MAMANINo ratings yet
- Class III Drugs: Potassium Channel BlockadeDocument3 pagesClass III Drugs: Potassium Channel BlockadeMohammadDheniArdhiNo ratings yet
- Antiarrhythmic Drugs 1Document32 pagesAntiarrhythmic Drugs 1AliImadAlKhasakiNo ratings yet
- AmiodaroneDocument13 pagesAmiodaroneAmy Hoo Hui May100% (1)
- Amiodarone Infusion GuidelineDocument3 pagesAmiodarone Infusion GuidelineNur SusiawantyNo ratings yet
- AF AmiodaronDocument7 pagesAF AmiodaronDita NururiyanieNo ratings yet
- PHARMACOLOGYDocument69 pagesPHARMACOLOGYKiran ShahNo ratings yet
- Drug # 1: Adrenaline: 1. Generic & Trade NameDocument61 pagesDrug # 1: Adrenaline: 1. Generic & Trade NameJawad ShahNo ratings yet
- Pharm Assigment 2Document28 pagesPharm Assigment 2Sarah-kate PatersonNo ratings yet
- Articaine (Septocaine) : Mu-Opioid Receptors Are in A Family of G-Protein Coupled ReceptorsDocument30 pagesArticaine (Septocaine) : Mu-Opioid Receptors Are in A Family of G-Protein Coupled ReceptorsphamnhuchauphuongNo ratings yet
- Adult: PO HTN Initial: 50-100 Mg/day in Single or Divided Doses Increase SlowlyDocument3 pagesAdult: PO HTN Initial: 50-100 Mg/day in Single or Divided Doses Increase SlowlyJoanna Marie Lumbre BalbiranNo ratings yet
- AntiarrhythmiaDocument29 pagesAntiarrhythmiaDRx Raju ChandranNo ratings yet
- Antiarrhythmic Drugs: Dr. Sachana KC 1 Year Resident Department of AnesthesiaDocument67 pagesAntiarrhythmic Drugs: Dr. Sachana KC 1 Year Resident Department of AnesthesiaKshitizma GiriNo ratings yet
- Amiodaron Sebagai Obat Anti Aritmia Dan Pengaruhnya Terhadap Fungsi TiroidDocument11 pagesAmiodaron Sebagai Obat Anti Aritmia Dan Pengaruhnya Terhadap Fungsi TiroidFarah MuthiaNo ratings yet
- Amdocal Final PDFDocument5 pagesAmdocal Final PDFSaifur Rahman SuzonNo ratings yet
- 3rd Year PharmacologyDocument43 pages3rd Year PharmacologyShayeeshan SivapalarajahNo ratings yet
- IvabradineDocument4 pagesIvabradineLamy SNo ratings yet
- National Drug Monograph Dronedarone (Multaq®) January 2010Document16 pagesNational Drug Monograph Dronedarone (Multaq®) January 2010cgc05001No ratings yet
- Anzcor Guideline 12 4 Medications and Fluids Aug16Document7 pagesAnzcor Guideline 12 4 Medications and Fluids Aug16flamur haskukajNo ratings yet
- Amlodipine by HamidDocument21 pagesAmlodipine by HamidShaheen UiiahNo ratings yet
- Mot Ilium TabDocument11 pagesMot Ilium TabChandra FatmaNo ratings yet
- Clinical Pharmacokinetics of Amiodarone: Roberto Latini, Gianni Tognoni Robert KatesDocument21 pagesClinical Pharmacokinetics of Amiodarone: Roberto Latini, Gianni Tognoni Robert KatesNanda apriliantoNo ratings yet
- FDCDocument10 pagesFDCAnkit PandeyNo ratings yet
- Antiarrhythmic Drugs: AmiodaroneDocument32 pagesAntiarrhythmic Drugs: Amiodaroneabd hamzaNo ratings yet
- S 039 LBLDocument45 pagesS 039 LBLAstha BhalodiaNo ratings yet
- Amlodipine-10mg TabletDocument7 pagesAmlodipine-10mg TabletMd. Abdur RahmanNo ratings yet
- AntiarrhythmicsDocument10 pagesAntiarrhythmicslandita683No ratings yet
- Local Anesthesia and Concious SedationDocument43 pagesLocal Anesthesia and Concious Sedationpawi18No ratings yet
- Anti Arrhythmic DrugsDocument91 pagesAnti Arrhythmic DrugsAlex beharuNo ratings yet
- Antiarrhytmic Talk For ResidenDocument90 pagesAntiarrhytmic Talk For ResidenMusa yohanaNo ratings yet
- Treatment & Management: Antithyroid DrugsDocument3 pagesTreatment & Management: Antithyroid DrugsRajDarvelGillNo ratings yet
- Temozolomide Drug MannualDocument51 pagesTemozolomide Drug MannualgubdiaNo ratings yet
- (See Details in DRUGDEX®) : Adult DosingDocument13 pages(See Details in DRUGDEX®) : Adult Dosingkinko6No ratings yet
- Daunorubicin: Drug NameDocument7 pagesDaunorubicin: Drug NameEdgar Ledesma-MartínezNo ratings yet
- Anti Arrhythmic Class TeachingDocument24 pagesAnti Arrhythmic Class TeachingchelvasureshNo ratings yet
- Basic Pharmacology And Drug Calculations [Practice Questions And Answers]From EverandBasic Pharmacology And Drug Calculations [Practice Questions And Answers]Rating: 4 out of 5 stars4/5 (1)
- Portopulmonary HypertensionDocument49 pagesPortopulmonary HypertensionMd FcpsNo ratings yet
- ASH and NASHDocument1 pageASH and NASHMd FcpsNo ratings yet
- Common Symtoms:: 1. Cough 2. Breathlessness 3. Hemoptysis 4. Chest PainDocument4 pagesCommon Symtoms:: 1. Cough 2. Breathlessness 3. Hemoptysis 4. Chest PainMd FcpsNo ratings yet
- Peripheral Arterial Disease PADDocument27 pagesPeripheral Arterial Disease PADMd FcpsNo ratings yet
- CetakDocument140 pagesCetakFuzoh MfzNo ratings yet
- Registration Form: by Phone by Fax On The Web by MailDocument2 pagesRegistration Form: by Phone by Fax On The Web by MailjdrockeyNo ratings yet
- Banchbo AN INITIATIVE FOR THE WELFARE OF SR. CITIZENSDocument61 pagesBanchbo AN INITIATIVE FOR THE WELFARE OF SR. CITIZENSRana BandyopadhyayNo ratings yet
- Skull FractureDocument13 pagesSkull FractureEddie LimNo ratings yet
- Bamboo Spine - X-Ray Findings of Ankylosing Spondylitis RevisitedDocument3 pagesBamboo Spine - X-Ray Findings of Ankylosing Spondylitis RevisitedpanjiNo ratings yet
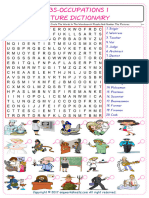
- Jobs-Occupations Find and Circle The Words in The Wordsearch Puzzle and Number The Pictures 7531Document2 pagesJobs-Occupations Find and Circle The Words in The Wordsearch Puzzle and Number The Pictures 7531Raquel NoeliaNo ratings yet
- Ludy Dobrila, PH.D., Phil Coelho, Pablo Rubinstein, M.D. New York Blood Center & Thermogenesis CorpDocument1 pageLudy Dobrila, PH.D., Phil Coelho, Pablo Rubinstein, M.D. New York Blood Center & Thermogenesis CorpCampaign MediaNo ratings yet
- June 2009 Nursing Practice 1Document9 pagesJune 2009 Nursing Practice 1Karl Gabriel BonifacioNo ratings yet
- Operating Room NotesDocument35 pagesOperating Room NotesMagdaraog Gabrielle A.No ratings yet
- PathologyDocument4 pagesPathologyVISHAKHANo ratings yet
- RPOC and Homoeopathy - A Practical StudyDocument4 pagesRPOC and Homoeopathy - A Practical StudyHomoeopathic Pulse100% (2)
- Home MedicineDocument29 pagesHome MedicineBasanthanesh BasanNo ratings yet
- General and Local AnesthesiaDocument1 pageGeneral and Local Anesthesiaahmedhelper300No ratings yet
- Top Dental Schools - Admission RequirementsDocument10 pagesTop Dental Schools - Admission RequirementsDental school admission0% (1)
- Pregnancy and TBDocument24 pagesPregnancy and TBRoza MaulindraNo ratings yet
- Interpretation of ResultDocument2 pagesInterpretation of ResultNatural Science BiologyNo ratings yet
- Racemic DrugsDocument6 pagesRacemic Drugsbub12345678No ratings yet
- Sist. MuscularDocument47 pagesSist. MuscularAlex Grande CancapaNo ratings yet
- Capítulo 10 SerdevDocument19 pagesCapítulo 10 SerdevErik BrooksNo ratings yet
- Veterinary Pharmacy, A Dismissed Necessity PDFDocument3 pagesVeterinary Pharmacy, A Dismissed Necessity PDFKelma TayebaNo ratings yet
- PICU NutritionDocument12 pagesPICU Nutritionmatenten100% (1)
- VOD - SOS in HSCTDocument25 pagesVOD - SOS in HSCTKim-Thinh Nguyen ThiNo ratings yet
- Therapeutic DietsDocument34 pagesTherapeutic DietsBanthracis67% (3)
- Introduction To Natural Products Chemistry: Rensheng Xu Yang Ye Weimin ZhaoDocument4 pagesIntroduction To Natural Products Chemistry: Rensheng Xu Yang Ye Weimin ZhaoWillowNo ratings yet
- Pharmacy Daily For Mon 14 Sep 2015 - ASMI Call To Speed Access, CMA Hails TGA CM Ticks, Hosp Phcy Standards, Weekly Comment and Much MoreDocument3 pagesPharmacy Daily For Mon 14 Sep 2015 - ASMI Call To Speed Access, CMA Hails TGA CM Ticks, Hosp Phcy Standards, Weekly Comment and Much MorepharmacydailyNo ratings yet
- Code BlueDocument18 pagesCode Blueandri100% (1)
- Links To Books and Additional MaterialDocument2 pagesLinks To Books and Additional MaterialCarl FernandesNo ratings yet





























































![Basic Pharmacology And Drug Calculations [Practice Questions And Answers]](https://imgv2-1-f.scribdassets.com/img/word_document/475660044/149x198/2c7fc45015/1691161640?v=1)