Download as pptx, pdf, or txt
You might also like
- Elizabeth G. Querubin BSN 3E1-9 - Group 195 A Ectopic PregnancyDocument16 pagesElizabeth G. Querubin BSN 3E1-9 - Group 195 A Ectopic PregnancyLizeth Querubin97% (38)
- Abnormal LaborDocument44 pagesAbnormal LaborCamille Espinosa100% (2)
- Cervical DystociaDocument22 pagesCervical DystociaBaldau TiwariNo ratings yet
- Prolonged Labour: Mrs. Shwetha Rani C.MDocument24 pagesProlonged Labour: Mrs. Shwetha Rani C.MSanthosh.S.U100% (1)
- Induction and Augmentation of LaborDocument22 pagesInduction and Augmentation of LaborDagnachew kasaye100% (1)
- Pregnancy Counseling Memorandums Chapter 8Document3 pagesPregnancy Counseling Memorandums Chapter 8Dennisha FeltonNo ratings yet
- Abnormal Labor and Abnormal Uterine Contractions (DystociaDocument31 pagesAbnormal Labor and Abnormal Uterine Contractions (DystociaMochamad RizalNo ratings yet
- Government College of Nursing Jodhpur: Presentation ON Prolonged LabourDocument6 pagesGovernment College of Nursing Jodhpur: Presentation ON Prolonged Labourpriyanka100% (3)
- Problemofthe PowerDocument8 pagesProblemofthe Powerjadeyorong2002No ratings yet
- Chapter 21: The Woman Who Develops A Complication During Labor and BirthDocument52 pagesChapter 21: The Woman Who Develops A Complication During Labor and BirthVincent Maralit MaterialNo ratings yet
- Dysfunctional LaborDocument29 pagesDysfunctional LaborKolimlim, Marienne SD.No ratings yet
- Dystocia: Presenter-Dr Aakriti Bhandari Moderated By-Dr. Ashok KumarDocument60 pagesDystocia: Presenter-Dr Aakriti Bhandari Moderated By-Dr. Ashok KumarAvishkar AgrawalNo ratings yet
- Week 5 NotesDocument12 pagesWeek 5 NotesgherlethrNo ratings yet
- Diagnosis and Mangement of Abnormal LabourDocument55 pagesDiagnosis and Mangement of Abnormal LabourVirda Maharani100% (3)
- Ectopic Pregnancy: Mbiine Ronald Nakiyemba OliviaDocument30 pagesEctopic Pregnancy: Mbiine Ronald Nakiyemba OliviaDIANENo ratings yet
- Abnormal Uterine ActionDocument64 pagesAbnormal Uterine ActionKanimozhi Kasinathan100% (1)
- Obstetri Dan Ginekologi 9a Partus TerlantarDocument20 pagesObstetri Dan Ginekologi 9a Partus Terlantar90Agva Dwi FatikaNo ratings yet
- Prolonged Labor and Labor InductionDocument28 pagesProlonged Labor and Labor InductionNovia RizqiNo ratings yet
- William Reading Abnormal LaborDocument14 pagesWilliam Reading Abnormal LaborLeo SSNo ratings yet
- 5 - DystociaDocument43 pages5 - DystociaMara Medina - BorleoNo ratings yet
- Induction Obstructed PrecipitateDocument38 pagesInduction Obstructed PrecipitateRose NyamburaNo ratings yet
- Intrapartal Complications 2023 PDFDocument8 pagesIntrapartal Complications 2023 PDFBrianna ValerioNo ratings yet
- First Trimester Bleeding ReportDocument35 pagesFirst Trimester Bleeding ReportAnita PrietoNo ratings yet
- Before Starting The Presentation, I Am Requesting You All To Get A HandkerchiefDocument35 pagesBefore Starting The Presentation, I Am Requesting You All To Get A HandkerchiefOng KarlNo ratings yet
- Abnormal Labour and It ManagementDocument27 pagesAbnormal Labour and It ManagementOsama AhmadNo ratings yet
- Dysfunctional Labor and BirthDocument167 pagesDysfunctional Labor and BirthKristel Joy Sarmiento AsuncionNo ratings yet
- Intrapartal Complications: Problems With The PowerDocument10 pagesIntrapartal Complications: Problems With The PowerkeinwayNo ratings yet
- Prolong LabourDocument5 pagesProlong LabourNishaThakuri100% (1)
- Complications of Labor & DeliveryDocument7 pagesComplications of Labor & DeliveryPatricia Anne Nicole CuaresmaNo ratings yet
- Abnormal Uterine ActionDocument110 pagesAbnormal Uterine ActionAnnapurna DangetiNo ratings yet
- 15 Dystocia Noted PDFDocument43 pages15 Dystocia Noted PDFmohammed farajiNo ratings yet
- Obstetric Operations & Procedures2Document98 pagesObstetric Operations & Procedures2mohazemalhotraNo ratings yet
- Abnormal Uterine ActionDocument27 pagesAbnormal Uterine Actiontanmai noolu100% (1)
- Inversion, Retained Placenta, AfeDocument95 pagesInversion, Retained Placenta, Afesushma sharmaNo ratings yet
- ACFrOgB40CYYfaqy K PEr1l2pQYS7J9CKoF1MzNRgUdEeaerp5y-GUUcxhhLpG-m5OUou-0hSVvKydlpjOQw2r0JNNDJa05hIf3kh47Kq6Qb3Lc4EbZZJrZnskvwOSk 94JNpKiPOaPE eXRxjIDocument6 pagesACFrOgB40CYYfaqy K PEr1l2pQYS7J9CKoF1MzNRgUdEeaerp5y-GUUcxhhLpG-m5OUou-0hSVvKydlpjOQw2r0JNNDJa05hIf3kh47Kq6Qb3Lc4EbZZJrZnskvwOSk 94JNpKiPOaPE eXRxjIJomer Levi PortuguezNo ratings yet
- Nursing Care of The High-Risk Labor and Delivery Client and Her FamilyDocument24 pagesNursing Care of The High-Risk Labor and Delivery Client and Her FamilyKenneth GingosaNo ratings yet
- Complication of Labor-Dysfunctional LaborDocument25 pagesComplication of Labor-Dysfunctional Laborcn351073No ratings yet
- Augmentation of LabourDocument45 pagesAugmentation of LabourLamnunnem HaokipNo ratings yet
- ABORTIONDocument22 pagesABORTIONJamie AgbannawagNo ratings yet
- Augmentation of Labour: Nabhan A, Boulvain MDocument8 pagesAugmentation of Labour: Nabhan A, Boulvain MMade SuryaNo ratings yet
- 2.1.3.1 Distosia Dan Prolapsus Tali Pusat SalinanDocument16 pages2.1.3.1 Distosia Dan Prolapsus Tali Pusat SalinanAkbp Mulyadi SHNo ratings yet
- Induction and Augmentation of LaborDocument20 pagesInduction and Augmentation of Laborjssamc prasootitantraNo ratings yet
- Postpartum HemorrhageDocument39 pagesPostpartum HemorrhageMarvin OcampoNo ratings yet
- C-S & VbacDocument54 pagesC-S & VbacDagnachew kasayeNo ratings yet
- Abnormal Uterine ActionDocument69 pagesAbnormal Uterine ActionBharat ThapaNo ratings yet
- Management of Bleeding in Early PregnancyDocument44 pagesManagement of Bleeding in Early PregnancyOyedele OluwaseunNo ratings yet
- Rle FinalsDocument9 pagesRle FinalsMary Florence VelardeNo ratings yet
- Prolonged & Obstructed Labor Rupture UterusDocument30 pagesProlonged & Obstructed Labor Rupture UterusIndri Heni DamanikNo ratings yet
- Bleeding in Early PregnancyDocument40 pagesBleeding in Early PregnancyOmar mohamedNo ratings yet
- Bleeding in Obstetrics طلبة تمريضDocument16 pagesBleeding in Obstetrics طلبة تمريضzeinabelsayed088No ratings yet
- Intrapartal ComplicationsDocument70 pagesIntrapartal ComplicationsRose AnnNo ratings yet
- Chapter 21Document69 pagesChapter 212082194No ratings yet
- Comlplications of Labor and DeliveryDocument73 pagesComlplications of Labor and DeliveryWai Kwong ChiuNo ratings yet
- Abnormal Uterine ActionsDocument31 pagesAbnormal Uterine ActionsPriscilla Sarah PayneNo ratings yet
- By: Dr. Ayman Bukhari House Officer Obstetrics & GynaecologyDocument54 pagesBy: Dr. Ayman Bukhari House Officer Obstetrics & GynaecologyBharat ThapaNo ratings yet
- Abnormal Labor and Dystocia: By: Norliana Binti JaafarDocument50 pagesAbnormal Labor and Dystocia: By: Norliana Binti JaafarNorliana Jaafar0% (1)
- Cervical Insuff-Wps OfficeDocument26 pagesCervical Insuff-Wps OfficewiselynshinyNo ratings yet
- Abnormal Labor: Li Ruzhi Ob&Gy Hospital, Fudan UniversityDocument51 pagesAbnormal Labor: Li Ruzhi Ob&Gy Hospital, Fudan UniversityLegoe Dwipa MahardhikaNo ratings yet
- Complications During Labor and Delivery: I. Dysfunctional Labor A. DystociaDocument16 pagesComplications During Labor and Delivery: I. Dysfunctional Labor A. DystociaEden NatividadNo ratings yet
- Post Partum Hemorrhage: Lunthaporn Puttanavinajarn, MDDocument50 pagesPost Partum Hemorrhage: Lunthaporn Puttanavinajarn, MDRedlamp MilNo ratings yet
- C1 LectureDocument44 pagesC1 LectureNatif BoteNo ratings yet
- AneamiaDocument27 pagesAneamiaNatif BoteNo ratings yet
- ANC For C1Document65 pagesANC For C1Natif BoteNo ratings yet
- AmnioticfluiddisorderDocument44 pagesAmnioticfluiddisorderNatif BoteNo ratings yet
- 1.HTN in Pregnancy by GemedaDocument69 pages1.HTN in Pregnancy by GemedaNatif BoteNo ratings yet
- 2 PidDocument31 pages2 PidNatif BoteNo ratings yet
- Female Reproductive (Ovarian) Cycle Menstrual CycleDocument3 pagesFemale Reproductive (Ovarian) Cycle Menstrual CycleLalit KumarNo ratings yet
- Voice of Quran and HealthDocument4 pagesVoice of Quran and HealthJack Ahmad Khotim MuzakkaNo ratings yet
- Hsslive Xii Zoology Prvs Questions Vers 2022 NavasDocument49 pagesHsslive Xii Zoology Prvs Questions Vers 2022 NavasShukoor CrazyNo ratings yet
- Sample of MRCOG Assessment 2021 - Saeed HasanDocument28 pagesSample of MRCOG Assessment 2021 - Saeed HasanIslam AwniNo ratings yet
- Wisconsin Abortion Lawsuit DecisionDocument21 pagesWisconsin Abortion Lawsuit DecisionTMJ4 NewsNo ratings yet
- Radiological Investigations: UltrasonographyDocument42 pagesRadiological Investigations: UltrasonographyDeeptanu GhoshNo ratings yet
- Surrogacy in IndiaDocument14 pagesSurrogacy in IndiaIshita RaiNo ratings yet
- Maternal Child CareDocument4 pagesMaternal Child Carecialina AlvezSevillaNo ratings yet
- Cezaldo - Asynch ActivityDocument3 pagesCezaldo - Asynch ActivityEva Marielle CezaldoNo ratings yet
- Coding ICD Yossi PDFDocument3 pagesCoding ICD Yossi PDFYossi Agung AriosenoNo ratings yet
- Part I. Public Health, Preventive and Family Medicine Principles & ConceptsDocument10 pagesPart I. Public Health, Preventive and Family Medicine Principles & ConceptsVenkatsai GadiparthiNo ratings yet
- Sapolsky - 3. Behavioral Evolution IIDocument5 pagesSapolsky - 3. Behavioral Evolution IImama doloresNo ratings yet
- Jurnal Skripsi Evita OktaviaDocument10 pagesJurnal Skripsi Evita OktaviaandiniNo ratings yet
- Neonatal PhysiologyDocument65 pagesNeonatal Physiologyunknownsince1986No ratings yet
- Bioethics and Its Application in Various Health SettingsDocument4 pagesBioethics and Its Application in Various Health SettingsXandra BasnilloNo ratings yet
- Child Birth Practices Across Cultures and Their ImplicationsDocument14 pagesChild Birth Practices Across Cultures and Their ImplicationsChintu ZoboloNo ratings yet
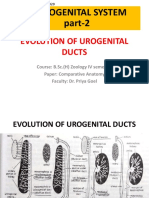
- Evolution of Urogenital Ducts Part-2 27.03.2020Document10 pagesEvolution of Urogenital Ducts Part-2 27.03.2020Sonali SahooNo ratings yet
- Ismat ChugtaiDocument4 pagesIsmat ChugtaiAlaika BansalNo ratings yet
- Breaking Bad News 1 PDFDocument5 pagesBreaking Bad News 1 PDFSaeed HasanNo ratings yet
- Characteristics of The NewbornDocument68 pagesCharacteristics of The Newbornpujitha2002100% (1)
- VPHY 113 - Avian ReproductionDocument73 pagesVPHY 113 - Avian ReproductionBob UrbandubNo ratings yet
- BNAPDocument106 pagesBNAPann29No ratings yet
- U.S. Selected Practice Recommendations For Contraceptive Use, 2016 MMWRDocument60 pagesU.S. Selected Practice Recommendations For Contraceptive Use, 2016 MMWRhectorNo ratings yet
- Research RefDocument18 pagesResearch Refbibibebebaby leeleeNo ratings yet
- Mmeanoba-V KursiDocument91 pagesMmeanoba-V KursinatitukaNo ratings yet
- Answerd FINAL EXAM STUDENT-1Document4 pagesAnswerd FINAL EXAM STUDENT-1Omar H100% (1)
- Amniotic Fluid EmbolismDocument26 pagesAmniotic Fluid EmbolismAnant PachisiaNo ratings yet
- Kel 3 A Midwifery Model of Care ForDocument13 pagesKel 3 A Midwifery Model of Care ForWawa KurniaNo ratings yet
- Science 5Document6 pagesScience 5Reuelyn ValenzuelaNo ratings yet