Download as ppt, pdf, or txt
You might also like
- COSHH Risk Assessment For RoundUPDocument2 pagesCOSHH Risk Assessment For RoundUPRonnie Murphy Knotweed Surveyor50% (2)
- Newborn ScreeningDocument20 pagesNewborn ScreeningAlec AnonNo ratings yet
- PV EXCEL 2019 20 A PDFDocument11 pagesPV EXCEL 2019 20 A PDFYash Raj Sisodiya50% (2)
- Endocrine DisordersDocument33 pagesEndocrine DisordersTinaNo ratings yet
- PHENYLKETONURIADocument22 pagesPHENYLKETONURIAIvy Ann AguirreNo ratings yet
- Nufd 255 Midterm Paper - No ReferencesDocument7 pagesNufd 255 Midterm Paper - No Referencesapi-305349012No ratings yet
- What Is Phenylketonuria ?: SymptomsDocument4 pagesWhat Is Phenylketonuria ?: Symptomsaaliya saaheenNo ratings yet
- Inborn Errors of MetabolismDocument40 pagesInborn Errors of MetabolismajjaNo ratings yet
- NCMA219Document11 pagesNCMA219Angelina Mei BenitezNo ratings yet
- PhenylketonuriaDocument7 pagesPhenylketonuriaAnny AlvrzNo ratings yet
- Phenylketonuria: Katrice Shorter, Steven Williams, Rodrigo Hallais, April Mcclendon "The Juice"Document24 pagesPhenylketonuria: Katrice Shorter, Steven Williams, Rodrigo Hallais, April Mcclendon "The Juice"Kimber ManiulitNo ratings yet
- PhenylketonuriaDocument7 pagesPhenylketonuriaReham QueNo ratings yet
- PhenylketonuriaDocument10 pagesPhenylketonuriaMalathy Ravendran100% (1)
- What Is Phenylketonuria?Document4 pagesWhat Is Phenylketonuria?Erica Joy Algire VillalunaNo ratings yet
- Symptoms: Disorder of Amino Acid MetabolismDocument2 pagesSymptoms: Disorder of Amino Acid Metabolismflex gyNo ratings yet
- PkuDocument6 pagesPkuAlbertEscanoNo ratings yet
- PhenylketonuriaDocument8 pagesPhenylketonuriaAmberlee PetiNo ratings yet
- PhenylketonuriaDocument1 pagePhenylketonuriaHolly SevillanoNo ratings yet
- Disorders of Amino Acid MetabolismDocument11 pagesDisorders of Amino Acid MetabolismDiyar AhmadNo ratings yet
- PhenylketonuriaDocument17 pagesPhenylketonuriamovies villa hit hai broNo ratings yet
- PhenylketonuriaDocument14 pagesPhenylketonuriaMonica MoralesNo ratings yet
- Biology PkuDocument15 pagesBiology Pkuapi-301088307No ratings yet
- PkubrochureDocument2 pagesPkubrochureapi-278063444No ratings yet
- The Child With An Endocrine or Metabolic Alteration: University of Maryland School of NursingDocument54 pagesThe Child With An Endocrine or Metabolic Alteration: University of Maryland School of NursingGelsey Gelsinator JianNo ratings yet
- Pediatrics ReviewDocument275 pagesPediatrics ReviewHaslinNo ratings yet
- Group 4 - Pku (BSN 1-A)Document11 pagesGroup 4 - Pku (BSN 1-A)oluanah13No ratings yet
- Phenyl Keto NuriaDocument3 pagesPhenyl Keto NuriawawawawaNo ratings yet
- Compilation of Research On PhenylketonuriaDocument12 pagesCompilation of Research On PhenylketonuriajudssalangsangNo ratings yet
- PHENYLKETONURIADocument4 pagesPHENYLKETONURIAmarsiel03No ratings yet
- Disorder LyonsDocument1 pageDisorder Lyonsapi-280441285No ratings yet
- Inborn Error of MetabolismDocument38 pagesInborn Error of MetabolismRubinaNo ratings yet
- PKUDocument8 pagesPKUNader Smadi100% (1)
- What Is PKU?: That Humans Obtain From Their Diet and Cannot Produce On Their Own.)Document2 pagesWhat Is PKU?: That Humans Obtain From Their Diet and Cannot Produce On Their Own.)SelliEfridaSiahaanNo ratings yet
- Inherited Metabolic DisorderDocument12 pagesInherited Metabolic DisorderTrisha Dianne RaquenioNo ratings yet
- DR Kumar Ponnusamy Biochemistry Genetics USMLE Preparatory Course BIOGEN Reusable On Line Resources For Large Group Teaching Learning in Relatively SHDocument2 pagesDR Kumar Ponnusamy Biochemistry Genetics USMLE Preparatory Course BIOGEN Reusable On Line Resources For Large Group Teaching Learning in Relatively SHPonnusamy KumarNo ratings yet
- Common IEM Solaf M Elsayed 2021Document13 pagesCommon IEM Solaf M Elsayed 2021anas barakahNo ratings yet
- Inborn Errors of Metabolism: Albinism, Cystinuria, Pentosuria And, of Course, AlkaptonuriaDocument19 pagesInborn Errors of Metabolism: Albinism, Cystinuria, Pentosuria And, of Course, AlkaptonuriaSubhi MishraNo ratings yet
- PhenyketonuriaDocument12 pagesPhenyketonuriamaryannejkiemNo ratings yet
- Quiz Blessings #6Document7 pagesQuiz Blessings #6Rachel LiuNo ratings yet
- Phenylketonuria (PKU) : (Metabolic Condition: Amino Acid Disorder)Document1 pagePhenylketonuria (PKU) : (Metabolic Condition: Amino Acid Disorder)reriti2008No ratings yet
- Munyame 2018Document6 pagesMunyame 2018kemoNo ratings yet
- Rare Disease DatabaseDocument7 pagesRare Disease DatabaseMudassar SattarNo ratings yet
- Fenilketonuria: Devi WuysangDocument23 pagesFenilketonuria: Devi WuysangChristantina Pradescha AssaNo ratings yet
- Biochemistry - METABOLISM OF PROTEINDocument44 pagesBiochemistry - METABOLISM OF PROTEINrebeccaNo ratings yet
- PHENYLKETONURIADocument3 pagesPHENYLKETONURIAMiwa IshiiNo ratings yet
- Phenylketonuria (Pku) : What Is It?Document3 pagesPhenylketonuria (Pku) : What Is It?Unnat ShresthaNo ratings yet
- American Academy of Pediatrics Metabolic Disorders 2014 Practice TestDocument43 pagesAmerican Academy of Pediatrics Metabolic Disorders 2014 Practice TestPrabu KumarNo ratings yet
- Case 9: Phenylketonuria: Group 1C: Obligado, Ervin Panibon, Lindsy Que, Reham Remitar, Jaira Dizza Salang, Marie NicholeDocument12 pagesCase 9: Phenylketonuria: Group 1C: Obligado, Ervin Panibon, Lindsy Que, Reham Remitar, Jaira Dizza Salang, Marie NicholeReham QueNo ratings yet
- Newborn ScreeningDocument15 pagesNewborn ScreeningYzel Vasquez AdavanNo ratings yet
- Phenylketonuria: Newborn Screening FACT SheetDocument1 pagePhenylketonuria: Newborn Screening FACT Sheetreriti2008No ratings yet
- Phenylketonuria ReviewDocument3 pagesPhenylketonuria Reviewapi-334247133No ratings yet
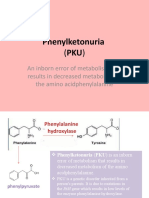
- Phenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino AcidphenylalanineDocument8 pagesPhenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino Acidphenylalanineელენე ბუჩუკურიNo ratings yet
- Phenylketonuria PkuDocument8 pagesPhenylketonuria Pkuapi-426734065No ratings yet
- MCH Group 8Document12 pagesMCH Group 8nafisatmuhammed452No ratings yet
- RA 9288 Newborn Screening ActDocument40 pagesRA 9288 Newborn Screening ActAkasha Frostmourne100% (2)
- Phenylketonuria (PKU) : Diagnosis and ManagementDocument2 pagesPhenylketonuria (PKU) : Diagnosis and ManagementFerdianaNo ratings yet
- Phenylketonuri A: Often Called PKUDocument10 pagesPhenylketonuri A: Often Called PKUgogogogoogogNo ratings yet
- Final Theoretical Exam in Pediatrics " Set A ": Choose The Most Appropriate ResponseDocument54 pagesFinal Theoretical Exam in Pediatrics " Set A ": Choose The Most Appropriate ResponseYousif AlaaNo ratings yet
- Phenyl Keto NuriaDocument1 pagePhenyl Keto NuriamucwcburdwanNo ratings yet
- How to Beat PCOS Naturally & Regain a Healthy & Fertile Life Now ( A Simple Guide on PCOS Diet & Exercises to Conquer PCOS Permanently Today)From EverandHow to Beat PCOS Naturally & Regain a Healthy & Fertile Life Now ( A Simple Guide on PCOS Diet & Exercises to Conquer PCOS Permanently Today)Rating: 3.5 out of 5 stars3.5/5 (6)
- OGL 482 Pro-Seminar II Module 6 Assignment: Career Plan TemplateDocument14 pagesOGL 482 Pro-Seminar II Module 6 Assignment: Career Plan Templateapi-561877895No ratings yet
- Diet, Drugs and DiseasesDocument39 pagesDiet, Drugs and DiseasesSolomon Royle UwumagbeNo ratings yet
- Mapeh (Health 10) Healthcare Providers and Healthcare PlanDocument7 pagesMapeh (Health 10) Healthcare Providers and Healthcare PlanKimberly Camacho CatubigNo ratings yet
- Human Resource MBA Interim Assessment On Strategic Workforce Planning On Coca Cola CompanyDocument11 pagesHuman Resource MBA Interim Assessment On Strategic Workforce Planning On Coca Cola Companyyash agarwalNo ratings yet
- The Arthritis Impact Measurement ScalesDocument3 pagesThe Arthritis Impact Measurement ScalesDon KaitoNo ratings yet
- Position PaperDocument2 pagesPosition PaperDonna Mae Icabandi TeñosoNo ratings yet
- HypertensionDocument29 pagesHypertensionمبدر حامدNo ratings yet
- Agriculture Unit Test ReviewDocument3 pagesAgriculture Unit Test ReviewEmily511No ratings yet
- Guideline For Registration of Low Risk MedicinesDocument23 pagesGuideline For Registration of Low Risk Medicinesmelaku yazieNo ratings yet
- Introduction To NutritionDocument206 pagesIntroduction To NutritionMompati LetsweletseNo ratings yet
- Post Term PregnancyDocument12 pagesPost Term PregnancyNicyela Jillien0% (1)
- Report On Patient Satisfaction and Waiting TimeDocument35 pagesReport On Patient Satisfaction and Waiting TimeRohit SharmaNo ratings yet
- Medical Missionary: TrainingDocument59 pagesMedical Missionary: TrainingRedz TagalaNo ratings yet
- 10x3 For Fat Loss by Chad WaterburyDocument1 page10x3 For Fat Loss by Chad WaterburyTim Donahey100% (5)
- Movie Review - Reign Over MeDocument2 pagesMovie Review - Reign Over Meabida.syeda.718No ratings yet
- Potassium Chloride - Drug Information - UpToDateDocument22 pagesPotassium Chloride - Drug Information - UpToDateJorge Luis German BecerraNo ratings yet
- Impact of Tooth Loss On The Quality of LifeDocument5 pagesImpact of Tooth Loss On The Quality of LifesonyanilaNo ratings yet
- Dexmedetomidine For Prolonged Sedation in The PICU: A Systematic Review and Meta-AnalysisDocument8 pagesDexmedetomidine For Prolonged Sedation in The PICU: A Systematic Review and Meta-AnalysisEliana Lopez BaronNo ratings yet
- Winchester Public School Pediculosis (Head Lice) : Our GoalsDocument2 pagesWinchester Public School Pediculosis (Head Lice) : Our GoalsFebby Indah NurcahyatiNo ratings yet
- Assessment of Hand Hygiene of Nursing and Medical Students: Rev Rene April 2017Document12 pagesAssessment of Hand Hygiene of Nursing and Medical Students: Rev Rene April 2017Durga Shankar DhakarNo ratings yet
- International Clinical Fellowship Programme Brochure - September - 2023Document29 pagesInternational Clinical Fellowship Programme Brochure - September - 2023Anam QadeerNo ratings yet
- Project Proposal On Transition ShelterDocument49 pagesProject Proposal On Transition ShelterLouie Jazper Jho Molina100% (1)
- OSHA 3186 - Bloodborne PathogensDocument29 pagesOSHA 3186 - Bloodborne PathogensWahed Mn ElnasNo ratings yet
- Perineal RuptureDocument24 pagesPerineal RuptureIzz ShuhaimiNo ratings yet
- Women and Mental HealthDocument15 pagesWomen and Mental HealthMAMTA SANODIYA100% (1)
- CBDR Handouts V2Document49 pagesCBDR Handouts V2Ariane Villanueva100% (2)
- CancerDocument15 pagesCancerGordo y TutucaNo ratings yet
- A Healthy Diet Is Essential For Good Health and NutritionDocument2 pagesA Healthy Diet Is Essential For Good Health and NutritionthenameisvijayNo ratings yet