Download as pptx, pdf, or txt
You might also like
- USMLE World Step 3 High Yield Notes 90 PagesDocument90 pagesUSMLE World Step 3 High Yield Notes 90 PagesVS95% (57)
- Color Atlas of Pediatrics PDFDocument1,399 pagesColor Atlas of Pediatrics PDFJose Guaman100% (10)
- Rademacher V ABC - MSJDocument26 pagesRademacher V ABC - MSJTHROnlineNo ratings yet
- Health Care Policy and NursingDocument32 pagesHealth Care Policy and NursingJas EstalloNo ratings yet
- Neil H. Riordan - Stem Cell Therapy A Rising Tide How Stem Cells Are Disrupting Medicine and Transforming LivesDocument341 pagesNeil H. Riordan - Stem Cell Therapy A Rising Tide How Stem Cells Are Disrupting Medicine and Transforming LivesLuca Dato100% (2)
- Introduction To Community Strategy PresentationDocument35 pagesIntroduction To Community Strategy PresentationKaranja Gitau100% (1)
- Atls MCQDocument10 pagesAtls MCQTerri Sandi Susyanto67% (15)
- Strategies of Health PromotionDocument20 pagesStrategies of Health PromotionLuis Mendoza Sy Jr100% (1)
- The Bamako InitiativeDocument4 pagesThe Bamako Initiativejohn mwangiNo ratings yet
- Community Health Nursing LectureDocument35 pagesCommunity Health Nursing LectureMaxeneDhaleNo ratings yet
- 5-Health PromotionDocument27 pages5-Health PromotionAsal Salah100% (1)
- PHC Concept & PrinciplesDocument68 pagesPHC Concept & PrinciplesDayò BáyòNo ratings yet
- 02 ManagementDocument78 pages02 Managementsandeepv08No ratings yet
- Health Education and Community Organizing Are Necessary in Providing Community Health ServicesDocument9 pagesHealth Education and Community Organizing Are Necessary in Providing Community Health ServicesDonaJeanNo ratings yet
- Health EducationDocument8 pagesHealth Educationmmeiring123480% (5)
- Ethiopia Public Health Training Initiative PDFDocument2 pagesEthiopia Public Health Training Initiative PDFAngieNo ratings yet
- Community Health Course Outline 2014 KingstonDocument11 pagesCommunity Health Course Outline 2014 KingstonJerilee SoCute Watts100% (2)
- Health Promotion and EducationDocument75 pagesHealth Promotion and EducationDaniel DubeNo ratings yet
- Health Administration NewDocument10 pagesHealth Administration NewjessyNo ratings yet
- Perform Nursing AssessmentDocument81 pagesPerform Nursing AssessmentAhmanur SuleNo ratings yet
- Kotebe Metropolitan University Menelik Ii Medical and Healthscience CollegeDocument25 pagesKotebe Metropolitan University Menelik Ii Medical and Healthscience Collegezeyneb pinkNo ratings yet
- 1 - Leadership and ManagementDocument7 pages1 - Leadership and Managementomer1998sul22100% (1)
- Health Education IIDocument59 pagesHealth Education IISakthi AbbiramiNo ratings yet
- Minimum Package of Service and Standards For Adolescent HealthDocument13 pagesMinimum Package of Service and Standards For Adolescent HealthAdeniyi Ademola Olaoluwa100% (1)
- Determinants of Health by VeereshDocument12 pagesDeterminants of Health by VeereshVeeresh TopalakattiNo ratings yet
- Health Financing: Dr. Jamelah R. Usman-PasagiDocument27 pagesHealth Financing: Dr. Jamelah R. Usman-PasagiGada AbdulcaderNo ratings yet
- Human Resources For Health-Dr T Sundar PresentnDocument29 pagesHuman Resources For Health-Dr T Sundar PresentnCharu BhatiNo ratings yet
- Introduction To Community Health NursingDocument23 pagesIntroduction To Community Health NursingAlmasNo ratings yet
- 1.2 Health Care Delivery SystemDocument53 pages1.2 Health Care Delivery Systemsefal mansuri100% (1)
- Che 262 Referral System and Outreach ServicesDocument15 pagesChe 262 Referral System and Outreach ServicesBalkos 61100% (3)
- Primary Health CareDocument2 pagesPrimary Health CareShamsa RiazNo ratings yet
- Public Health and Primary Health CareDocument15 pagesPublic Health and Primary Health Caremisdduaa100% (2)
- Pre Test Exam On Adolescent Youth Friendly Service For Health WorkersDocument2 pagesPre Test Exam On Adolescent Youth Friendly Service For Health WorkersTamiruNo ratings yet
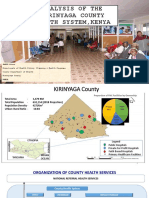
- Analysis of The Kirinyaga County Health System - Esbon - GakuuDocument18 pagesAnalysis of The Kirinyaga County Health System - Esbon - Gakuuesbon gakuu100% (1)
- Viva-Questions Community MedicineDocument3 pagesViva-Questions Community Medicineadeel_khan_48No ratings yet
- Primary Health CareDocument41 pagesPrimary Health CareKailash NagarNo ratings yet
- Complete CHEW CurriculumDocument162 pagesComplete CHEW CurriculumAbdulhamidNo ratings yet
- Unit 1 Planning and Organization of Nursing Service: 1 0 ObjectivesDocument12 pagesUnit 1 Planning and Organization of Nursing Service: 1 0 ObjectivesRenita ChrisNo ratings yet
- Health Promotion LO1&2Document24 pagesHealth Promotion LO1&2Mohd Johari Mohd ShafuwanNo ratings yet
- Health Information SystemDocument11 pagesHealth Information SystemVineeta Jose100% (1)
- National Health Policy and PlanDocument92 pagesNational Health Policy and PlanChetan BhattaNo ratings yet
- The Factors That Influence Our Food Choices: 1. Major Determinants of Food ChoiceDocument18 pagesThe Factors That Influence Our Food Choices: 1. Major Determinants of Food ChoiceFrancis GongNo ratings yet
- Health EducationDocument8 pagesHealth EducationJamie Rose FontanillaNo ratings yet
- Evaluation of Health ServicesDocument42 pagesEvaluation of Health Servicesdrsanjeev15No ratings yet
- Health System in India at District LevelDocument8 pagesHealth System in India at District LevelKailash Nagar100% (1)
- 5.2 Intersectoral ApproachDocument55 pages5.2 Intersectoral ApproachShivangi SharmaNo ratings yet
- Module 4 - Community Health AssessmentDocument8 pagesModule 4 - Community Health AssessmentSteffi100% (1)
- 2nutritionassmt Studay1819Document101 pages2nutritionassmt Studay1819RaysonChoo100% (2)
- Question Bank QP 1774 Management of Nursing Services and EducationDocument14 pagesQuestion Bank QP 1774 Management of Nursing Services and Educationmelby2604No ratings yet
- Unit - 1 Introduction To Public HealthDocument63 pagesUnit - 1 Introduction To Public HealthVedansha SinghalNo ratings yet
- Epidemiology AssignmentDocument12 pagesEpidemiology AssignmentSagar ParajuliNo ratings yet
- RN BSN-CIG-Topic 14 - Concepts of Primary Health CareDocument34 pagesRN BSN-CIG-Topic 14 - Concepts of Primary Health CarebettinabetsonNo ratings yet
- Asella Teaching & Referral Hospital Asella Teaching & Referral HospitalDocument43 pagesAsella Teaching & Referral Hospital Asella Teaching & Referral Hospitalnemo amboNo ratings yet
- Community Health Nursing Process (The Basics of Community Health Nursing by Gesmundo)Document18 pagesCommunity Health Nursing Process (The Basics of Community Health Nursing by Gesmundo)YsabellaPlarisan100% (1)
- Women and Occupational HealthDocument12 pagesWomen and Occupational Healthniju_grgNo ratings yet
- Rapid Appraisal Tool For Hospital ManagementDocument40 pagesRapid Appraisal Tool For Hospital Managementrehanbutt78100% (1)
- Health Management Information SystemDocument4 pagesHealth Management Information SystemMica Capistrano100% (3)
- National Harmonized Nursing Curriculum February 2013Document476 pagesNational Harmonized Nursing Curriculum February 2013Yakob TadeseNo ratings yet
- 3136 - OA - Motivation Among Nurses PDFDocument6 pages3136 - OA - Motivation Among Nurses PDFShahnaz DarNo ratings yet
- Basic Principles of Health EconomicsDocument13 pagesBasic Principles of Health EconomicsMuna Hassan Mustafa100% (1)
- Introduction To Public HealthDocument24 pagesIntroduction To Public HealthGaurav PuriNo ratings yet
- Philosophy and Theoretical Framework For Community Health Nursing Practice HandoutDocument3 pagesPhilosophy and Theoretical Framework For Community Health Nursing Practice Handoutᜀᜇᜒᜐ᜔ ᜇᜒᜎ ᜃ᜔ᜇᜓᜐ᜔100% (1)
- Community Health A Complete Guide - 2020 EditionFrom EverandCommunity Health A Complete Guide - 2020 EditionRating: 5 out of 5 stars5/5 (1)
- Chronic Non-communicable Diseases in Ghana: Multidisciplinary PerspectivesFrom EverandChronic Non-communicable Diseases in Ghana: Multidisciplinary PerspectivesNo ratings yet
- Basic Principles of Primary HealthcareDocument43 pagesBasic Principles of Primary HealthcareShyla Bantolinao100% (1)
- Adrenal DiseasesDocument66 pagesAdrenal DiseasesNebiyu NegaNo ratings yet
- Introduction To Economics Exercise Chapter TwoDocument5 pagesIntroduction To Economics Exercise Chapter TwoNebiyu NegaNo ratings yet
- Introduction To Nursing ProcessDocument62 pagesIntroduction To Nursing ProcessNebiyu NegaNo ratings yet
- ThermoregulationDocument27 pagesThermoregulationNebiyu NegaNo ratings yet
- First Aid For Severe Bleeding: HS95-072D (9-06) A 5-Minute Safety Training AidDocument1 pageFirst Aid For Severe Bleeding: HS95-072D (9-06) A 5-Minute Safety Training Aidعلي منصور الوليNo ratings yet
- Bhastrika Kapalbhati: Sidhhasan, Padamasan, SukhasanDocument1 pageBhastrika Kapalbhati: Sidhhasan, Padamasan, SukhasanrajivmohinderNo ratings yet
- Carotid-Cavernous Fistula: Current Concepts in Aetiology, Investigation, and ManagementDocument9 pagesCarotid-Cavernous Fistula: Current Concepts in Aetiology, Investigation, and Managementandre halimNo ratings yet
- 2020, Grubb Et Al., 2020 AAHA Anesthesia and Monitoring Guidelines For Dogs and CatsDocument29 pages2020, Grubb Et Al., 2020 AAHA Anesthesia and Monitoring Guidelines For Dogs and CatsyohanethNo ratings yet
- Lung Expansion TherapyDocument108 pagesLung Expansion TherapyJean NoronhaNo ratings yet
- The Care of Congenital Myopathy: A Guide For Families. CMFG-2018-9-29 Update (Web Quality)Document105 pagesThe Care of Congenital Myopathy: A Guide For Families. CMFG-2018-9-29 Update (Web Quality)congenitalmyopathyresourceNo ratings yet
- CH-7 Class 12Document54 pagesCH-7 Class 12Mahima FamousNo ratings yet
- SCRC One Pager Version 1.0 Oct 2020Document2 pagesSCRC One Pager Version 1.0 Oct 2020naval730107No ratings yet
- Hukm Ophthal Guideline-Latest Edited PDFDocument107 pagesHukm Ophthal Guideline-Latest Edited PDFNur atikahNo ratings yet
- Bmjopen 2020 January 10 1 Inline Supplementary Material 1Document31 pagesBmjopen 2020 January 10 1 Inline Supplementary Material 1mazen alkarras100% (1)
- Lentile ScleraleDocument40 pagesLentile ScleraleLauraNo ratings yet
- Gems Opt Select Brochure 2021 v6 3Document2 pagesGems Opt Select Brochure 2021 v6 3Bongani West VuthaNo ratings yet
- AHCCCS Pharmacy and Therapeutics Committee May 19, 2021Document247 pagesAHCCCS Pharmacy and Therapeutics Committee May 19, 2021hussam mazinNo ratings yet
- Recent Trials in Neonatology - Part IIDocument70 pagesRecent Trials in Neonatology - Part IIPranay MallNo ratings yet
- Bowel Obstruction SurgeryDocument12 pagesBowel Obstruction SurgeryDivya JoyNo ratings yet
- Superficial Thrombophlebitis Follow-Up Study: Legs: Randomized, ControlledDocument7 pagesSuperficial Thrombophlebitis Follow-Up Study: Legs: Randomized, ControlledFlorin BzoviiNo ratings yet
- Fnhum 09 00513Document13 pagesFnhum 09 00513MichelleSpurlockNo ratings yet
- Perioperative Care For CABG PatientsDocument32 pagesPerioperative Care For CABG PatientsAya EyadNo ratings yet
- Peri Op FINAL OBJECTIVES May 2021Document12 pagesPeri Op FINAL OBJECTIVES May 2021Omar SanyangNo ratings yet
- Questions and Answers: TetanusDocument4 pagesQuestions and Answers: TetanusJahanzaib NiaziNo ratings yet
- The Safe Food HandlerDocument51 pagesThe Safe Food Handlernagalariel04No ratings yet
- Covid 19 y Trombosis VacunasDocument7 pagesCovid 19 y Trombosis VacunasSMIBA MedicinaNo ratings yet
- 1 Cervical and Vaginal CytologyDocument63 pages1 Cervical and Vaginal Cytologynanxtoyah100% (1)
- Pest and Disease Problems in Mushroom CultivationDocument6 pagesPest and Disease Problems in Mushroom CultivationJOSE ESTRADANo ratings yet
- Airway Emergency ManagementDocument47 pagesAirway Emergency ManagementTerefe AlemayehuNo ratings yet