
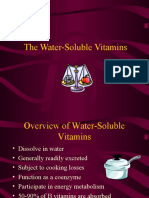
Water Soluble Vitamins
Water Soluble Vitamins
You might also like
- Aortic Stenosis (As)Document20 pagesAortic Stenosis (As)rameshbmc100% (1)
- Ictal and Postictal Psychiatric Disturbances - TrimbleDocument5 pagesIctal and Postictal Psychiatric Disturbances - Trimblegoo99No ratings yet
- Pico PaperDocument9 pagesPico PaperTraci Braden100% (2)
- Stages of LaborDocument5 pagesStages of LaborGeraldine Marie Salvo100% (4)
- Water Soluble VitaminDocument96 pagesWater Soluble Vitaminjeevalakshmanan29No ratings yet
- Vitamin B2 - B6Document19 pagesVitamin B2 - B6Biruk GeremewNo ratings yet
- B ComplexDocument25 pagesB ComplexBimalKrishnaNo ratings yet
- Bs VitaminsDocument9 pagesBs Vitaminsrin_ndNo ratings yet
- Vitamin 20 JulyDocument33 pagesVitamin 20 JulySafura IjazNo ratings yet
- VitaminsDocument96 pagesVitaminskiedd_0480% (5)
- NIACINDocument4 pagesNIACINJustin Paul ChanNo ratings yet
- Water Soluble Vitamin (Kuliah 3) - 2Document95 pagesWater Soluble Vitamin (Kuliah 3) - 2Pardamean SamosirNo ratings yet
- 01 VitaminsDocument49 pages01 VitaminsFatish BanguraNo ratings yet
- VitaminsDocument191 pagesVitaminsAyush JainNo ratings yet
- Nutrition VitaminDocument7 pagesNutrition VitaminIsabella SupardiNo ratings yet
- Vitamins and MineralsDocument91 pagesVitamins and MineralsPyaesone AungNo ratings yet
- DR Okunowo Wahab Introductory Molecular Biology Lecture Note I (Nucleotides Metabolism)Document20 pagesDR Okunowo Wahab Introductory Molecular Biology Lecture Note I (Nucleotides Metabolism)modelprof100% (2)
- 081220190water Soluble Vit. (E.Sh) Lecture 2 - 2019 StudentsDocument22 pages081220190water Soluble Vit. (E.Sh) Lecture 2 - 2019 Studentsslmen1269No ratings yet
- Vit B1,2,3 (Autosaved)Document23 pagesVit B1,2,3 (Autosaved)lovi bahunNo ratings yet
- Niacin: DR. Beenish Zafar BiochemistryDocument32 pagesNiacin: DR. Beenish Zafar BiochemistryShehryar AbbasNo ratings yet
- Water-Soluble VitaminsDocument32 pagesWater-Soluble VitaminsHomed OpriNo ratings yet
- Vitamin B3Document6 pagesVitamin B3JIHAN LUTHFINo ratings yet
- Vitamin B CDocument67 pagesVitamin B CAulia IsnaidaNo ratings yet
- Protein SynthesisDocument12 pagesProtein SynthesisDenny DevandyaNo ratings yet
- Water Soluble VitaminsDocument55 pagesWater Soluble VitaminsDr. M. Prasad Naidu100% (1)
- Degradation of Purine PDFDocument36 pagesDegradation of Purine PDFShrey SundriyalNo ratings yet
- Degradation of PurineDocument36 pagesDegradation of PurineShrey SundriyalNo ratings yet
- Angel Bds Water Soluble VitaminsDocument107 pagesAngel Bds Water Soluble Vitaminsseenuu53No ratings yet
- Vitamin BDocument6 pagesVitamin BFatinNo ratings yet
- Water Soluble VitaminsDocument87 pagesWater Soluble VitaminsSwosti ShresthaNo ratings yet
- Nutritional Biochemistry: Vitamins Dr. Bidhan Chandra KonerDocument50 pagesNutritional Biochemistry: Vitamins Dr. Bidhan Chandra KonerElenanana100% (1)
- 8 Chat PDFDocument9 pages8 Chat PDFPertiwi Dwi WahyuniNo ratings yet
- VitaminsDocument32 pagesVitaminsdivya100% (5)
- Vitamins: Lec.1: Dr. NahidaDocument11 pagesVitamins: Lec.1: Dr. NahidaxxxdarknessNo ratings yet
- Water Soluble Vitamin: Dept. of Nutrition Medical School Universitas PadjadjaranDocument49 pagesWater Soluble Vitamin: Dept. of Nutrition Medical School Universitas PadjadjaranHadiyatussalamah Pusfa KencanasariNo ratings yet
- Nucleotide Metabolism PPDocument65 pagesNucleotide Metabolism PPCLEMENTNo ratings yet
- Vitamin B5: (Pantothenic Acid)Document53 pagesVitamin B5: (Pantothenic Acid)Sagar BadnakheNo ratings yet
- Metabolitos Azealaic AcidDocument4 pagesMetabolitos Azealaic AcidGuillermo GonzalezNo ratings yet
- Vitamins B5, B6, B7: Amal Fahma Ak S1 MSC BiotechologyDocument51 pagesVitamins B5, B6, B7: Amal Fahma Ak S1 MSC BiotechologyRoman DudeNo ratings yet
- Vitamins + Their DeficienciesDocument6 pagesVitamins + Their DeficienciesKieran KillingtonNo ratings yet
- Metabolism of TryptophanDocument38 pagesMetabolism of Tryptophanjagan mohan rao vanaNo ratings yet
- VitaminDocument62 pagesVitaminKrunal Patel100% (1)
- Metabolism HW1 Energy Vitamins SP24Document5 pagesMetabolism HW1 Energy Vitamins SP24raybuaNo ratings yet
- 32 LN Water Soluble Vitamins II BLGDocument45 pages32 LN Water Soluble Vitamins II BLGDakshitha DharmakeerthiNo ratings yet
- Metabolic Bioquem Kaplan NotesDocument6 pagesMetabolic Bioquem Kaplan NotesDrbee10100% (1)
- Vitamin A, Vitamin D, Thiamine, Riboflavine, Pyridoxine, Niacinamide, Folic Acid, Ascorbic Acid, Panth. AcidDocument130 pagesVitamin A, Vitamin D, Thiamine, Riboflavine, Pyridoxine, Niacinamide, Folic Acid, Ascorbic Acid, Panth. AcidsalinaNo ratings yet
- Vitamin and Trace ElementsDocument8 pagesVitamin and Trace Elementskiedd_04100% (2)
- Acute Poisoning of Therapeutic Agents: by Alemayehu TomaDocument42 pagesAcute Poisoning of Therapeutic Agents: by Alemayehu TomaYohannis AsefaNo ratings yet
- Water-Soluble Vitamins: Intestinal Absorption For Selected VitaminsDocument58 pagesWater-Soluble Vitamins: Intestinal Absorption For Selected VitaminsRoxanna LevineNo ratings yet
- Biochemistry One Liners by Medical LearnerDocument13 pagesBiochemistry One Liners by Medical LearnerSwapnil PawarNo ratings yet
- Purine MetabolismDocument30 pagesPurine MetabolismSamarTharwatNo ratings yet
- Vitamin b52c b62cb72cb9b12 Final 1Document53 pagesVitamin b52c b62cb72cb9b12 Final 1Anonymous zJcGQRnQCNo ratings yet
- Vitamins Dr. Luzon Water SolubleDocument3 pagesVitamins Dr. Luzon Water SolubleTina Malabanan CobarrubiasNo ratings yet
- VitaminsDocument77 pagesVitaminsEsosa OdighizuwaNo ratings yet
- Water Soluble Vitamins Lecture For 1st Year MBBS by DR Sadia HaroonDocument67 pagesWater Soluble Vitamins Lecture For 1st Year MBBS by DR Sadia HaroonIMDCBiochem100% (2)
- 2 - Vitamin B ComplexDocument57 pages2 - Vitamin B ComplexPaulinNo ratings yet
- Biochemistry Last Minute Revision PDFDocument23 pagesBiochemistry Last Minute Revision PDFSUBHANAN SAHANo ratings yet
- Lecture 10. Basic Concepts of Vitaminology. Biochemistry of Water-Soluble and Fat-Soluble VitaminsDocument58 pagesLecture 10. Basic Concepts of Vitaminology. Biochemistry of Water-Soluble and Fat-Soluble VitaminsВіталій Михайлович НечипорукNo ratings yet
- VitaminsDocument29 pagesVitaminsVijay KrishnaNo ratings yet
- Micronutrients, VitaminsDocument32 pagesMicronutrients, VitaminsEsdras DountioNo ratings yet
- Vit B1-6Document84 pagesVit B1-6ffshikaariNo ratings yet
- Defisiensi VitaminDocument30 pagesDefisiensi VitaminRulianis ApriantiNo ratings yet
- How To Lose Belly Fats in 20 Days Guaranteed (Action Required)Document3 pagesHow To Lose Belly Fats in 20 Days Guaranteed (Action Required)Idongesit KoffiNo ratings yet
- M. Roberts - Modernity, Mental Illness and The Crisis of MeaningDocument5 pagesM. Roberts - Modernity, Mental Illness and The Crisis of MeaningKenneth AndersonNo ratings yet
- Pituitary Adenoma FinalDocument44 pagesPituitary Adenoma FinalTuhinaRaj100% (1)
- Patogenesis Malaria - Dr. A. Visi Kartika, SP - PADocument26 pagesPatogenesis Malaria - Dr. A. Visi Kartika, SP - PAahmadyawidyatmaNo ratings yet
- Surgery For Gastric Cancer Hoon Noh 1 Ed 2019 PDFDocument355 pagesSurgery For Gastric Cancer Hoon Noh 1 Ed 2019 PDFKarem MaaliNo ratings yet
- CDC - Stool Specimen CollectionDocument3 pagesCDC - Stool Specimen CollectionC. HidalgoNo ratings yet
- DM Health Teaching PlanDocument5 pagesDM Health Teaching PlancamilatanNo ratings yet
- Course Specs Template FinalDocument11 pagesCourse Specs Template FinalDena MohamedNo ratings yet
- Curacen EngDocument19 pagesCuracen Engstanescu_radu_mirceaNo ratings yet
- Gandhi - Collected Works Vol 12Document487 pagesGandhi - Collected Works Vol 12Nrusimha ( नृसिंह )No ratings yet
- Fever in Children With ChemoteraphyDocument23 pagesFever in Children With ChemoteraphyImanuel Far-FarNo ratings yet
- Hypovolemic Shock Pathophysiology, Symptoms, Signs, Treatment - EHealthStarDocument15 pagesHypovolemic Shock Pathophysiology, Symptoms, Signs, Treatment - EHealthStarKaloy KamaoNo ratings yet
- Neonatal Hiatal Hernia - A Rare Case ReportDocument4 pagesNeonatal Hiatal Hernia - A Rare Case ReportAgus DarwiyantoNo ratings yet
- Health: Minidoka County Joint School District #331Document13 pagesHealth: Minidoka County Joint School District #331Minidoka County Joint School DistrictNo ratings yet
- Scientific ProgramDocument40 pagesScientific ProgramDrAhmad HammadyNo ratings yet
- English Worksheet 8 N3Document3 pagesEnglish Worksheet 8 N3Will MendozaNo ratings yet
- Bassett and Turner 2007Document17 pagesBassett and Turner 2007Ludovic FanstenNo ratings yet
- Oncology Drills With Answers and RationalesDocument41 pagesOncology Drills With Answers and RationalesCarol Kayas100% (1)
- Thesis On Antioxidant Activity of Medicinal Plants PDFDocument6 pagesThesis On Antioxidant Activity of Medicinal Plants PDFafazapfjl100% (2)
- Nhis Ghana - Overview Reforms Achievements Version 3Document29 pagesNhis Ghana - Overview Reforms Achievements Version 3Nana Virtuoso EsselNo ratings yet
- Antimicrobial Sensitivity TestingDocument21 pagesAntimicrobial Sensitivity TestingLaiba FarooqNo ratings yet
- Teens and Mobile PhonesDocument2 pagesTeens and Mobile PhonesHeyNo ratings yet
- Quiz 2Document5 pagesQuiz 2Ani MepharishviliNo ratings yet
- Examination of Intestinal Obstruction, Acute Abdomen and Acute Appendicitis - Eugh & BwembyaDocument29 pagesExamination of Intestinal Obstruction, Acute Abdomen and Acute Appendicitis - Eugh & BwembyaForeighn97No ratings yet
- Dysfunctional LaborDocument29 pagesDysfunctional LaborKolimlim, Marienne SD.No ratings yet
- Manajemen Sindroma Metabolik Pada Lansia Lisa BaruDocument55 pagesManajemen Sindroma Metabolik Pada Lansia Lisa BaruvianemichelleNo ratings yet



















































































Download as pptx, pdf, or txt
You might also like
- Aortic Stenosis (As)Document20 pagesAortic Stenosis (As)rameshbmc100% (1)
- Ictal and Postictal Psychiatric Disturbances - TrimbleDocument5 pagesIctal and Postictal Psychiatric Disturbances - Trimblegoo99No ratings yet
- Pico PaperDocument9 pagesPico PaperTraci Braden100% (2)
- Stages of LaborDocument5 pagesStages of LaborGeraldine Marie Salvo100% (4)
- Water Soluble VitaminDocument96 pagesWater Soluble Vitaminjeevalakshmanan29No ratings yet
- Vitamin B2 - B6Document19 pagesVitamin B2 - B6Biruk GeremewNo ratings yet
- B ComplexDocument25 pagesB ComplexBimalKrishnaNo ratings yet
- Bs VitaminsDocument9 pagesBs Vitaminsrin_ndNo ratings yet
- Vitamin 20 JulyDocument33 pagesVitamin 20 JulySafura IjazNo ratings yet
- VitaminsDocument96 pagesVitaminskiedd_0480% (5)
- NIACINDocument4 pagesNIACINJustin Paul ChanNo ratings yet
- Water Soluble Vitamin (Kuliah 3) - 2Document95 pagesWater Soluble Vitamin (Kuliah 3) - 2Pardamean SamosirNo ratings yet
- 01 VitaminsDocument49 pages01 VitaminsFatish BanguraNo ratings yet
- VitaminsDocument191 pagesVitaminsAyush JainNo ratings yet
- Nutrition VitaminDocument7 pagesNutrition VitaminIsabella SupardiNo ratings yet
- Vitamins and MineralsDocument91 pagesVitamins and MineralsPyaesone AungNo ratings yet
- DR Okunowo Wahab Introductory Molecular Biology Lecture Note I (Nucleotides Metabolism)Document20 pagesDR Okunowo Wahab Introductory Molecular Biology Lecture Note I (Nucleotides Metabolism)modelprof100% (2)
- 081220190water Soluble Vit. (E.Sh) Lecture 2 - 2019 StudentsDocument22 pages081220190water Soluble Vit. (E.Sh) Lecture 2 - 2019 Studentsslmen1269No ratings yet
- Vit B1,2,3 (Autosaved)Document23 pagesVit B1,2,3 (Autosaved)lovi bahunNo ratings yet
- Niacin: DR. Beenish Zafar BiochemistryDocument32 pagesNiacin: DR. Beenish Zafar BiochemistryShehryar AbbasNo ratings yet
- Water-Soluble VitaminsDocument32 pagesWater-Soluble VitaminsHomed OpriNo ratings yet
- Vitamin B3Document6 pagesVitamin B3JIHAN LUTHFINo ratings yet
- Vitamin B CDocument67 pagesVitamin B CAulia IsnaidaNo ratings yet
- Protein SynthesisDocument12 pagesProtein SynthesisDenny DevandyaNo ratings yet
- Water Soluble VitaminsDocument55 pagesWater Soluble VitaminsDr. M. Prasad Naidu100% (1)
- Degradation of Purine PDFDocument36 pagesDegradation of Purine PDFShrey SundriyalNo ratings yet
- Degradation of PurineDocument36 pagesDegradation of PurineShrey SundriyalNo ratings yet
- Angel Bds Water Soluble VitaminsDocument107 pagesAngel Bds Water Soluble Vitaminsseenuu53No ratings yet
- Vitamin BDocument6 pagesVitamin BFatinNo ratings yet
- Water Soluble VitaminsDocument87 pagesWater Soluble VitaminsSwosti ShresthaNo ratings yet
- Nutritional Biochemistry: Vitamins Dr. Bidhan Chandra KonerDocument50 pagesNutritional Biochemistry: Vitamins Dr. Bidhan Chandra KonerElenanana100% (1)
- 8 Chat PDFDocument9 pages8 Chat PDFPertiwi Dwi WahyuniNo ratings yet
- VitaminsDocument32 pagesVitaminsdivya100% (5)
- Vitamins: Lec.1: Dr. NahidaDocument11 pagesVitamins: Lec.1: Dr. NahidaxxxdarknessNo ratings yet
- Water Soluble Vitamin: Dept. of Nutrition Medical School Universitas PadjadjaranDocument49 pagesWater Soluble Vitamin: Dept. of Nutrition Medical School Universitas PadjadjaranHadiyatussalamah Pusfa KencanasariNo ratings yet
- Nucleotide Metabolism PPDocument65 pagesNucleotide Metabolism PPCLEMENTNo ratings yet
- Vitamin B5: (Pantothenic Acid)Document53 pagesVitamin B5: (Pantothenic Acid)Sagar BadnakheNo ratings yet
- Metabolitos Azealaic AcidDocument4 pagesMetabolitos Azealaic AcidGuillermo GonzalezNo ratings yet
- Vitamins B5, B6, B7: Amal Fahma Ak S1 MSC BiotechologyDocument51 pagesVitamins B5, B6, B7: Amal Fahma Ak S1 MSC BiotechologyRoman DudeNo ratings yet
- Vitamins + Their DeficienciesDocument6 pagesVitamins + Their DeficienciesKieran KillingtonNo ratings yet
- Metabolism of TryptophanDocument38 pagesMetabolism of Tryptophanjagan mohan rao vanaNo ratings yet
- VitaminDocument62 pagesVitaminKrunal Patel100% (1)
- Metabolism HW1 Energy Vitamins SP24Document5 pagesMetabolism HW1 Energy Vitamins SP24raybuaNo ratings yet
- 32 LN Water Soluble Vitamins II BLGDocument45 pages32 LN Water Soluble Vitamins II BLGDakshitha DharmakeerthiNo ratings yet
- Metabolic Bioquem Kaplan NotesDocument6 pagesMetabolic Bioquem Kaplan NotesDrbee10100% (1)
- Vitamin A, Vitamin D, Thiamine, Riboflavine, Pyridoxine, Niacinamide, Folic Acid, Ascorbic Acid, Panth. AcidDocument130 pagesVitamin A, Vitamin D, Thiamine, Riboflavine, Pyridoxine, Niacinamide, Folic Acid, Ascorbic Acid, Panth. AcidsalinaNo ratings yet
- Vitamin and Trace ElementsDocument8 pagesVitamin and Trace Elementskiedd_04100% (2)
- Acute Poisoning of Therapeutic Agents: by Alemayehu TomaDocument42 pagesAcute Poisoning of Therapeutic Agents: by Alemayehu TomaYohannis AsefaNo ratings yet
- Water-Soluble Vitamins: Intestinal Absorption For Selected VitaminsDocument58 pagesWater-Soluble Vitamins: Intestinal Absorption For Selected VitaminsRoxanna LevineNo ratings yet
- Biochemistry One Liners by Medical LearnerDocument13 pagesBiochemistry One Liners by Medical LearnerSwapnil PawarNo ratings yet
- Purine MetabolismDocument30 pagesPurine MetabolismSamarTharwatNo ratings yet
- Vitamin b52c b62cb72cb9b12 Final 1Document53 pagesVitamin b52c b62cb72cb9b12 Final 1Anonymous zJcGQRnQCNo ratings yet
- Vitamins Dr. Luzon Water SolubleDocument3 pagesVitamins Dr. Luzon Water SolubleTina Malabanan CobarrubiasNo ratings yet
- VitaminsDocument77 pagesVitaminsEsosa OdighizuwaNo ratings yet
- Water Soluble Vitamins Lecture For 1st Year MBBS by DR Sadia HaroonDocument67 pagesWater Soluble Vitamins Lecture For 1st Year MBBS by DR Sadia HaroonIMDCBiochem100% (2)
- 2 - Vitamin B ComplexDocument57 pages2 - Vitamin B ComplexPaulinNo ratings yet
- Biochemistry Last Minute Revision PDFDocument23 pagesBiochemistry Last Minute Revision PDFSUBHANAN SAHANo ratings yet
- Lecture 10. Basic Concepts of Vitaminology. Biochemistry of Water-Soluble and Fat-Soluble VitaminsDocument58 pagesLecture 10. Basic Concepts of Vitaminology. Biochemistry of Water-Soluble and Fat-Soluble VitaminsВіталій Михайлович НечипорукNo ratings yet
- VitaminsDocument29 pagesVitaminsVijay KrishnaNo ratings yet
- Micronutrients, VitaminsDocument32 pagesMicronutrients, VitaminsEsdras DountioNo ratings yet
- Vit B1-6Document84 pagesVit B1-6ffshikaariNo ratings yet
- Defisiensi VitaminDocument30 pagesDefisiensi VitaminRulianis ApriantiNo ratings yet
- How To Lose Belly Fats in 20 Days Guaranteed (Action Required)Document3 pagesHow To Lose Belly Fats in 20 Days Guaranteed (Action Required)Idongesit KoffiNo ratings yet
- M. Roberts - Modernity, Mental Illness and The Crisis of MeaningDocument5 pagesM. Roberts - Modernity, Mental Illness and The Crisis of MeaningKenneth AndersonNo ratings yet
- Pituitary Adenoma FinalDocument44 pagesPituitary Adenoma FinalTuhinaRaj100% (1)
- Patogenesis Malaria - Dr. A. Visi Kartika, SP - PADocument26 pagesPatogenesis Malaria - Dr. A. Visi Kartika, SP - PAahmadyawidyatmaNo ratings yet
- Surgery For Gastric Cancer Hoon Noh 1 Ed 2019 PDFDocument355 pagesSurgery For Gastric Cancer Hoon Noh 1 Ed 2019 PDFKarem MaaliNo ratings yet
- CDC - Stool Specimen CollectionDocument3 pagesCDC - Stool Specimen CollectionC. HidalgoNo ratings yet
- DM Health Teaching PlanDocument5 pagesDM Health Teaching PlancamilatanNo ratings yet
- Course Specs Template FinalDocument11 pagesCourse Specs Template FinalDena MohamedNo ratings yet
- Curacen EngDocument19 pagesCuracen Engstanescu_radu_mirceaNo ratings yet
- Gandhi - Collected Works Vol 12Document487 pagesGandhi - Collected Works Vol 12Nrusimha ( नृसिंह )No ratings yet
- Fever in Children With ChemoteraphyDocument23 pagesFever in Children With ChemoteraphyImanuel Far-FarNo ratings yet
- Hypovolemic Shock Pathophysiology, Symptoms, Signs, Treatment - EHealthStarDocument15 pagesHypovolemic Shock Pathophysiology, Symptoms, Signs, Treatment - EHealthStarKaloy KamaoNo ratings yet
- Neonatal Hiatal Hernia - A Rare Case ReportDocument4 pagesNeonatal Hiatal Hernia - A Rare Case ReportAgus DarwiyantoNo ratings yet
- Health: Minidoka County Joint School District #331Document13 pagesHealth: Minidoka County Joint School District #331Minidoka County Joint School DistrictNo ratings yet
- Scientific ProgramDocument40 pagesScientific ProgramDrAhmad HammadyNo ratings yet
- English Worksheet 8 N3Document3 pagesEnglish Worksheet 8 N3Will MendozaNo ratings yet
- Bassett and Turner 2007Document17 pagesBassett and Turner 2007Ludovic FanstenNo ratings yet
- Oncology Drills With Answers and RationalesDocument41 pagesOncology Drills With Answers and RationalesCarol Kayas100% (1)
- Thesis On Antioxidant Activity of Medicinal Plants PDFDocument6 pagesThesis On Antioxidant Activity of Medicinal Plants PDFafazapfjl100% (2)
- Nhis Ghana - Overview Reforms Achievements Version 3Document29 pagesNhis Ghana - Overview Reforms Achievements Version 3Nana Virtuoso EsselNo ratings yet
- Antimicrobial Sensitivity TestingDocument21 pagesAntimicrobial Sensitivity TestingLaiba FarooqNo ratings yet
- Teens and Mobile PhonesDocument2 pagesTeens and Mobile PhonesHeyNo ratings yet
- Quiz 2Document5 pagesQuiz 2Ani MepharishviliNo ratings yet
- Examination of Intestinal Obstruction, Acute Abdomen and Acute Appendicitis - Eugh & BwembyaDocument29 pagesExamination of Intestinal Obstruction, Acute Abdomen and Acute Appendicitis - Eugh & BwembyaForeighn97No ratings yet
- Dysfunctional LaborDocument29 pagesDysfunctional LaborKolimlim, Marienne SD.No ratings yet
- Manajemen Sindroma Metabolik Pada Lansia Lisa BaruDocument55 pagesManajemen Sindroma Metabolik Pada Lansia Lisa BaruvianemichelleNo ratings yet