Download as ppt, pdf, or txt
You might also like
- Bula RespiratóriosDocument30 pagesBula RespiratóriosMaria Correia100% (1)
- Virology Influenza Nad ParainfluenzaDocument4 pagesVirology Influenza Nad ParainfluenzaHisham ChomanyNo ratings yet
- K.3 Pediatri-Virologi 3 2018-2019 PDFDocument76 pagesK.3 Pediatri-Virologi 3 2018-2019 PDFandi firdha restuwatiNo ratings yet
- Paramyxoviruses: Dr. Muna M A Yousif M.D Clinical MicrobiologyDocument30 pagesParamyxoviruses: Dr. Muna M A Yousif M.D Clinical MicrobiologyJaydee PlataNo ratings yet
- Paramyxovirus: Measles Virus Mumps Virus Respiratory Syncytial Virus (RSV) Parainfluenza VirusesDocument45 pagesParamyxovirus: Measles Virus Mumps Virus Respiratory Syncytial Virus (RSV) Parainfluenza VirusesRotten PotatoNo ratings yet
- Respiratory SyncytialDocument32 pagesRespiratory Syncytialtummalapalli venkateswara rao100% (2)
- Togaviridae: Rubella (German Measles)Document3 pagesTogaviridae: Rubella (German Measles)Nikita SHARMANo ratings yet
- 1 Cjcastillo : ND THDocument3 pages1 Cjcastillo : ND THArion Andronicus AvilaNo ratings yet
- Negative Stranded RNA VirusesDocument47 pagesNegative Stranded RNA VirusesNovie Carla GayosaNo ratings yet
- Pediatrics in Review 2014 Piedimonte 519 30Document15 pagesPediatrics in Review 2014 Piedimonte 519 30Felipe CeaNo ratings yet
- Virology Respiratory VirusesDocument6 pagesVirology Respiratory VirusesHisham ChomanyNo ratings yet
- Virology ControlDocument89 pagesVirology ControlNishani SatiyaseelanNo ratings yet
- WO Trpmed HHDocument26 pagesWO Trpmed HHWinona JenniferNo ratings yet
- Medical Micro ExamsDocument8 pagesMedical Micro ExamsJennifer NokuthulaNo ratings yet
- Respiratory Syncytial VirusDocument16 pagesRespiratory Syncytial VirusAradhanaRamchandaniNo ratings yet
- Virology AssignmentDocument7 pagesVirology AssignmentChethu ChethzNo ratings yet
- Microbiology Presentation: Mumps, Measles & PoliovirusDocument31 pagesMicrobiology Presentation: Mumps, Measles & PoliovirusdenekeNo ratings yet
- Viral Exanthema: Dharmendra MandalDocument57 pagesViral Exanthema: Dharmendra MandalMaunank TandelNo ratings yet
- Acute Respiratory Viral Infections: Prof. S. M. Turyanitsa Dr. Karabinyosh S.ODocument29 pagesAcute Respiratory Viral Infections: Prof. S. M. Turyanitsa Dr. Karabinyosh S.ODOCTOR DanishNo ratings yet
- Chapter 66 Respiratory & Gastro VirusesDocument8 pagesChapter 66 Respiratory & Gastro VirusesleoNo ratings yet
- HerpesviridaeDocument7 pagesHerpesviridaeRaghad AlNo ratings yet
- Virus Respiratorio SincicialDocument10 pagesVirus Respiratorio SincicialNicole Castillo AguirreNo ratings yet
- 5.0orthomyxoviruses 3.1Document41 pages5.0orthomyxoviruses 3.1Jiya MuhammadNo ratings yet
- Mumps, Measles and Rubella: Aman UllahDocument19 pagesMumps, Measles and Rubella: Aman UllahHabib UllahNo ratings yet
- 01LongChap34 Pneumoniaandcomplications PDFDocument15 pages01LongChap34 Pneumoniaandcomplications PDFAngela Mitchelle NyanganNo ratings yet
- InfluenzaDocument54 pagesInfluenzaakhmedovg16No ratings yet
- Measles: EtiologyDocument14 pagesMeasles: EtiologyHan SANo ratings yet
- PicornavirusDocument35 pagesPicornavirusAmna ShahidNo ratings yet
- Virology LecturesDocument72 pagesVirology LecturesKrishma GuptaNo ratings yet
- Measles EpiDocument22 pagesMeasles Epiمحمد صالحNo ratings yet
- M U M P S: Dr.T.V.Rao MDDocument35 pagesM U M P S: Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Orthomyxoviruses: Retno Budiarti Microbiology Department FK UhtDocument40 pagesOrthomyxoviruses: Retno Budiarti Microbiology Department FK UhtDwi faidah agustinaNo ratings yet
- Paramyxoviridae EditedDocument30 pagesParamyxoviridae EditedstudymedicNo ratings yet
- MUMPSDocument3 pagesMUMPSCarla NicoleNo ratings yet
- Viral and Atypical Pneumonias PDFDocument12 pagesViral and Atypical Pneumonias PDFtaxxusNo ratings yet
- Viral Infection: NAME-Rahul Pawar (Roll No.17) Sanket Joshi (Roll No.25)Document25 pagesViral Infection: NAME-Rahul Pawar (Roll No.17) Sanket Joshi (Roll No.25)aditya_aditya_mayekar199No ratings yet
- MUMPSDocument32 pagesMUMPSVer Garcera TalosigNo ratings yet
- Orthomyxoviridae - Avian, Equine and Swine InfluenzaDocument19 pagesOrthomyxoviridae - Avian, Equine and Swine InfluenzaELIJAH EUMIR CUNANANNo ratings yet
- Paramyxoviridae: For 3 Year MLS StudentsDocument57 pagesParamyxoviridae: For 3 Year MLS StudentsAbdurhman SeidNo ratings yet
- Classification:: Influenza, Commonly Referred To As The Flu, Is An Infectious Disease Caused by RNA Viruses ofDocument6 pagesClassification:: Influenza, Commonly Referred To As The Flu, Is An Infectious Disease Caused by RNA Viruses ofSi VeekeeNo ratings yet
- HerpesvirusesDocument54 pagesHerpesvirusessameera ruffaiNo ratings yet
- 5 Herpes VirusesDocument5 pages5 Herpes VirusesTᕼE FᗩᗪEᗪ ᔕOᑌᒪNo ratings yet
- HE ParotitisDocument17 pagesHE ParotitisWaktuku KecilNo ratings yet
- Coxsackie VirusDocument10 pagesCoxsackie Virusjyothsna yarraNo ratings yet
- Influenza VirusDocument15 pagesInfluenza VirusadwNo ratings yet
- Brief: Human Metapneumovirus InfectionDocument4 pagesBrief: Human Metapneumovirus InfectionmedicotayacajaNo ratings yet
- Day 6 Virology - January 2021Document222 pagesDay 6 Virology - January 2021ShriefElghazalyNo ratings yet
- Respiratory Virus InfectionsDocument9 pagesRespiratory Virus InfectionsChawki MokademNo ratings yet
- MRCPCH Guide InfDocument19 pagesMRCPCH Guide InfRajiv Kabad100% (1)
- (MIKROBIOLOGI) IT 20 - Orthomyxovirus, Paramyxovirus - KHSDocument37 pages(MIKROBIOLOGI) IT 20 - Orthomyxovirus, Paramyxovirus - KHSRessy FelisaNo ratings yet
- RubellaDocument30 pagesRubellatummalapalli venkateswara rao100% (1)
- General Concepts: Clinical ManifestationsDocument6 pagesGeneral Concepts: Clinical ManifestationsSyafda Heroni FirdausNo ratings yet
- Rubella VirusDocument14 pagesRubella VirusLincy JohnyNo ratings yet
- Medical Virology CLS 413: by DR - Dalia M. MohsenDocument20 pagesMedical Virology CLS 413: by DR - Dalia M. MohsenDalia M. MohsenNo ratings yet
- ORTHOMYXOVIRUSESDocument21 pagesORTHOMYXOVIRUSESkarengregorio2No ratings yet
- Viral Infections of The Skin and Mucus MembranesDocument54 pagesViral Infections of The Skin and Mucus MembranesVikaNo ratings yet
- Mycoplasma Infect The Upper Respiratory Tract and Can Cause Pneumonia. Pneumonia Is AnDocument11 pagesMycoplasma Infect The Upper Respiratory Tract and Can Cause Pneumonia. Pneumonia Is AnJenny TaylorNo ratings yet
- Lecture 5/ Medical Microbiology / 2ed Class StreptococcusDocument9 pagesLecture 5/ Medical Microbiology / 2ed Class Streptococcusهدى قحطان جليلNo ratings yet
- CDs L2 4th 2021 2022Document46 pagesCDs L2 4th 2021 2022محمد رافد لطيفNo ratings yet
- ORTHOMYXOVIRUS and PARAMYXOVIRUSDocument21 pagesORTHOMYXOVIRUS and PARAMYXOVIRUSDaniel SantosNo ratings yet
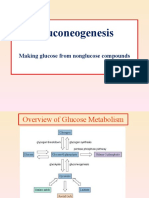
- Curs GluconeogenesisDocument25 pagesCurs GluconeogenesisOnofrei MariaNo ratings yet
- Parvoviruses and AdenovirusesDocument15 pagesParvoviruses and AdenovirusesOnofrei MariaNo ratings yet
- HIV Engleza BriefDocument108 pagesHIV Engleza BriefOnofrei MariaNo ratings yet
- Arboviruses LectureDocument42 pagesArboviruses LectureOnofrei MariaNo ratings yet
- Nobivac l4 Epar Product Information - enDocument18 pagesNobivac l4 Epar Product Information - enakshaygarande4048No ratings yet
- The Management of Acute Bronchitis in Children: ReviewDocument12 pagesThe Management of Acute Bronchitis in Children: ReviewRismaNo ratings yet
- Croup (Laryngotracheobronchitis) : EtiologyDocument13 pagesCroup (Laryngotracheobronchitis) : EtiologyOmar mohamedNo ratings yet
- Bp2013 Vet IndexDocument10 pagesBp2013 Vet IndexPatel VivekNo ratings yet
- ParamyxoviridaeDocument27 pagesParamyxoviridaeFarrah BenoitNo ratings yet
- Paramyxoviridae EditedDocument30 pagesParamyxoviridae EditedstudymedicNo ratings yet
- Daniela Ferreira Pneumococcus and Respiratory VirusDocument38 pagesDaniela Ferreira Pneumococcus and Respiratory Viruskp.bestellingenNo ratings yet
- A Fuller Picture of Vaccination - FinalDocument36 pagesA Fuller Picture of Vaccination - FinalJessica Learmond-CriquiNo ratings yet
- Virology Influenza Nad ParainfluenzaDocument4 pagesVirology Influenza Nad ParainfluenzaHisham ChomanyNo ratings yet
- ParamyxovirusesDocument21 pagesParamyxovirusesKhorusakiNo ratings yet
- Diagnosis, Treatment, and Prevention of Adenovirus Infection - UpToDateDocument28 pagesDiagnosis, Treatment, and Prevention of Adenovirus Infection - UpToDateMisael TaverasNo ratings yet
- Influenza y ParainfluenzaDocument14 pagesInfluenza y ParainfluenzaLaura Natalia Cordoba RiañoNo ratings yet
- Croup - Clinical Features, Evaluation, and Diagnosis - UpToDateDocument43 pagesCroup - Clinical Features, Evaluation, and Diagnosis - UpToDateRafaela BassettiNo ratings yet
- RFIT-PRT-0895 FilmArrayPneumoplus Instructions For Use EN PDFDocument112 pagesRFIT-PRT-0895 FilmArrayPneumoplus Instructions For Use EN PDFGuneyden GuneydenNo ratings yet
- Mcqs On Virology by Misango Da Phd.Document101 pagesMcqs On Virology by Misango Da Phd.Musa yohana100% (2)
- Survival of Human Coronaviruses 229E and OC43 in Suspension and After Drying On Surfaces: A Possible Source of Hospital-Acquired InfectionsDocument6 pagesSurvival of Human Coronaviruses 229E and OC43 in Suspension and After Drying On Surfaces: A Possible Source of Hospital-Acquired InfectionsR JNo ratings yet
- Croup - Clinical Features, Evaluation, and Diagnosis - UpToDateDocument30 pagesCroup - Clinical Features, Evaluation, and Diagnosis - UpToDateAmr MohamedNo ratings yet
- Canigen l4 Epar Product Information - en PDFDocument21 pagesCanigen l4 Epar Product Information - en PDFKris Pam Gorion PerezNo ratings yet
- Pediatrics InfectionDocument75 pagesPediatrics InfectionHikufe JesayaNo ratings yet
- Eurican Technicalsheet 12-08-2019Document2 pagesEurican Technicalsheet 12-08-2019dzulfikarfaizin romasNo ratings yet
- Microbiology TablesDocument19 pagesMicrobiology TablesRebecca MarshallNo ratings yet
- Paramyxoviruses: Dr. Muna M A Yousif M.D Clinical MicrobiologyDocument30 pagesParamyxoviruses: Dr. Muna M A Yousif M.D Clinical MicrobiologyJaydee PlataNo ratings yet
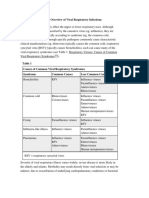
- 1 - Overview of Viral Respiratory InfectionsDocument3 pages1 - Overview of Viral Respiratory Infectionssapik zirafNo ratings yet
- Infectious Diseases of The Lungs: Viral InfectionsDocument46 pagesInfectious Diseases of The Lungs: Viral InfectionsSusana PaçoNo ratings yet
- Paramyxoviridae: For 3 Year MLS StudentsDocument57 pagesParamyxoviridae: For 3 Year MLS StudentsAbdurhman SeidNo ratings yet
- Respiratory Virus InfectionsDocument9 pagesRespiratory Virus InfectionsChawki MokademNo ratings yet
- Spectra 10 Detail Sheet PDFDocument1 pageSpectra 10 Detail Sheet PDFTITUS WHITENo ratings yet
- Virologi Bronkitis-BronkiolitisDocument28 pagesVirologi Bronkitis-BronkiolitisVia EkawatiNo ratings yet
- Bronchiolitis in Infants and Children - Clinical Features and DiagnosisDocument18 pagesBronchiolitis in Infants and Children - Clinical Features and DiagnosisJose GiertzNo ratings yet