Download as ppt, pdf, or txt
You might also like
- 7.down SyndromeDocument15 pages7.down SyndromeTiara Khairina100% (1)
- Icd 10 Cm/PcsDocument4 pagesIcd 10 Cm/Pcsmuhammad maulana67% (6)
- Multiple Pregnancy LectureDocument33 pagesMultiple Pregnancy Lecturefarid_nchep100% (1)
- Treatment of Bronchial AsthmaDocument50 pagesTreatment of Bronchial AsthmaJindal Chest ClinicNo ratings yet
- Asma Dan Penyakit Paru Obstruktif KronisDocument34 pagesAsma Dan Penyakit Paru Obstruktif KronisAtikah ArifahNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument33 pagesChronic Obstructive Pulmonary DiseasealexpharmNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) : Assistant Sukhonos NDocument17 pagesChronic Obstructive Pulmonary Disease (COPD) : Assistant Sukhonos NRayan Rayan darwishNo ratings yet
- Update MX of COPDDocument60 pagesUpdate MX of COPDNusrat JahanNo ratings yet
- Copd PDFDocument28 pagesCopd PDFDarawan MirzaNo ratings yet
- Copd in Primary CareDocument27 pagesCopd in Primary CarerobyalfNo ratings yet
- COPD1Document1 pageCOPD1kentkriziaNo ratings yet
- Gold and Gina Guideline For Copd and AsthmaDocument56 pagesGold and Gina Guideline For Copd and AsthmaSomnath Das Gupta100% (1)
- Asthma: Chronic Inflammation of The Airways. The Hyper-Responsive Airways Typical of AsthmaDocument7 pagesAsthma: Chronic Inflammation of The Airways. The Hyper-Responsive Airways Typical of AsthmaRaj PaulNo ratings yet
- Chronic Obstructive Pulmonary Disease: Olga Alexeevna EfremovaDocument56 pagesChronic Obstructive Pulmonary Disease: Olga Alexeevna Efremovaسيف الشمريNo ratings yet
- Asthma and COPDDocument28 pagesAsthma and COPDShoaib PatelNo ratings yet
- 1 - CopdDocument40 pages1 - Copdvmj8tyh5dsNo ratings yet
- Copd 2022Document45 pagesCopd 2022Mubassir NisarNo ratings yet
- CopdDocument41 pagesCopdneelumshaukatNo ratings yet
- Chronic Obstructive Pulmonary Disease: Presented byDocument25 pagesChronic Obstructive Pulmonary Disease: Presented byChinni 12599No ratings yet
- COPD Bat NoteDocument6 pagesCOPD Bat NoteLankeshwaraNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) : Assistant Professor:Tong JinDocument39 pagesChronic Obstructive Pulmonary Disease (COPD) : Assistant Professor:Tong JinEINSTEIN2DNo ratings yet
- COPD FixDocument47 pagesCOPD FixerniNo ratings yet
- Pulmonary Diseases: Medically Compromised PatientDocument50 pagesPulmonary Diseases: Medically Compromised Patientمحمد عبدالهادي إسماعيلNo ratings yet
- COPDDocument6 pagesCOPDAubrey PerezNo ratings yet
- COPDDocument49 pagesCOPDArmoured SpartanNo ratings yet
- Copd ReportDocument69 pagesCopd ReportRadley Jed C. PelagioNo ratings yet
- N24: Class #8 Obstructive and Inflammatory Lung Disease: Emphysema Chronic Bronchitis AsthmaDocument42 pagesN24: Class #8 Obstructive and Inflammatory Lung Disease: Emphysema Chronic Bronchitis Asthmadentist40No ratings yet
- (Chronic Obstructive Pulmonary Disease) : Kelompok DDocument31 pages(Chronic Obstructive Pulmonary Disease) : Kelompok DErwin BawonoNo ratings yet
- COPD - Salmorin & SatairapanDocument13 pagesCOPD - Salmorin & SatairapanMichelle SatairapanNo ratings yet
- Acute Exacerbation of CopdDocument28 pagesAcute Exacerbation of CopdMohd RafiNo ratings yet
- DR Premkumar M.D Assistant Professor Department of MedicineDocument22 pagesDR Premkumar M.D Assistant Professor Department of MedicineGowripathy B GowripathyNo ratings yet
- 7a COPDDocument45 pages7a COPDDerrick GramataNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument10 pagesChronic Obstructive Pulmonary DiseaseZinya RobinsonNo ratings yet
- Obstructive Lung DiseasesDocument34 pagesObstructive Lung DiseasesshivaniNo ratings yet
- Copd (Chronic Obstructive: Pulmonary Disease)Document68 pagesCopd (Chronic Obstructive: Pulmonary Disease)sinan kNo ratings yet
- COPDDocument42 pagesCOPDAnoos rabayarabayaNo ratings yet
- Respiratory EmergenciesDocument34 pagesRespiratory EmergenciesRoshana MallawaarachchiNo ratings yet
- Respiratory AssessmentDocument8 pagesRespiratory AssessmentScott HalNo ratings yet
- SURGERY Important NotesDocument14 pagesSURGERY Important Notesnob2011nobNo ratings yet
- #6 Copd 11 PDFDocument11 pages#6 Copd 11 PDFOmar BasimNo ratings yet
- COPDDocument41 pagesCOPDsanalcrazy100% (3)
- CopdDocument47 pagesCopdNingshesil Ny HermantNo ratings yet
- A Case Presentation On Chronic Obstructive Disease (COPD)Document18 pagesA Case Presentation On Chronic Obstructive Disease (COPD)Harvey T. Dato-onNo ratings yet
- Chronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredDocument25 pagesChronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredOmar AbdillahiNo ratings yet
- Obstructive Airways Disease: Asthma and COPDDocument29 pagesObstructive Airways Disease: Asthma and COPDRaxter ErNo ratings yet
- 70, - H 35 - H 2 - O N, L T: T: E G D - Develop A Self Management PlanDocument11 pages70, - H 35 - H 2 - O N, L T: T: E G D - Develop A Self Management PlanjljoioiuNo ratings yet
- Optimizing Management of Asthma and COPDDocument58 pagesOptimizing Management of Asthma and COPDJindal Chest ClinicNo ratings yet
- COPDDocument21 pagesCOPDAnnisNo ratings yet
- Chronic BronchitisDocument2 pagesChronic BronchitisKhalid Mahmud ArifinNo ratings yet
- Copd (Chronic Obstructive Pulmonary Disease)Document11 pagesCopd (Chronic Obstructive Pulmonary Disease)Catherine MetraNo ratings yet
- Merged 37Document21 pagesMerged 37abdulkreemsalem4No ratings yet
- CopdDocument22 pagesCopdNARUTONo ratings yet
- Copd by Musa Afridi 17-029Document6 pagesCopd by Musa Afridi 17-029Essa AfridiNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD)Document5 pagesChronic Obstructive Pulmonary Disease (COPD)mzunl25476No ratings yet
- K10 - Copd 2011Document47 pagesK10 - Copd 20111e23e2ewNo ratings yet
- Patient Prep: Follow Guidelines On P. 65 of Clinical PacketDocument4 pagesPatient Prep: Follow Guidelines On P. 65 of Clinical PacketKatherine AmbrosiaNo ratings yet
- Gold 2019Document43 pagesGold 2019Hayatillah Natasya100% (1)
- Asthma 1. DefinitionDocument11 pagesAsthma 1. DefinitionKarl RobleNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument45 pagesChronic Obstructive Pulmonary DiseaseAlexander Santiago ParelNo ratings yet
- Respiratory DiseasesDocument9 pagesRespiratory Diseaseschristian pulmonesNo ratings yet
- Drugs Affecting The Respiratory Systems: Kuntarti, SKP, MbiomedDocument32 pagesDrugs Affecting The Respiratory Systems: Kuntarti, SKP, MbiomedRichard BungaNo ratings yet
- Drug Induced Pulmonary DiseasesDocument26 pagesDrug Induced Pulmonary Diseaseswiona morasNo ratings yet
- Medico Legal IssuesDocument18 pagesMedico Legal IssuesJindal Chest ClinicNo ratings yet
- AllergyDocument23 pagesAllergyJindal Chest ClinicNo ratings yet
- Difficult Airway in ICU by Dr. Aditya Jindal - JIndal Chest ClinicDocument32 pagesDifficult Airway in ICU by Dr. Aditya Jindal - JIndal Chest ClinicJindal Chest ClinicNo ratings yet
- Disease Consequences of Bidi Smoking - Jindal Chest ClinicDocument20 pagesDisease Consequences of Bidi Smoking - Jindal Chest ClinicJindal Chest ClinicNo ratings yet
- Breathing Difficulty - Jindal Chest JindalDocument2 pagesBreathing Difficulty - Jindal Chest JindalJindal Chest ClinicNo ratings yet
- Sleep Disorders - Overview and PitfallsDocument77 pagesSleep Disorders - Overview and PitfallsJindal Chest ClinicNo ratings yet
- Pleural Cavity - Jindal Chest ClinicDocument36 pagesPleural Cavity - Jindal Chest ClinicJindal Chest ClinicNo ratings yet
- Intractable, Refractory Cough - Jindal IVF ChandigarhDocument9 pagesIntractable, Refractory Cough - Jindal IVF ChandigarhJindal Chest ClinicNo ratings yet
- Table 59-1 - Nia-Aa Core Clinical Diagnostic Criteria For AllDocument2 pagesTable 59-1 - Nia-Aa Core Clinical Diagnostic Criteria For AllDragutin PetrićNo ratings yet
- Non KeratinocytesDocument21 pagesNon KeratinocytesAbi AbiramithangamNo ratings yet
- Yakima Co (WA) Protocols 2010Document117 pagesYakima Co (WA) Protocols 2010Anthony James-Hartwell100% (1)
- PapulosquamousDocument5 pagesPapulosquamousMinh ChâuNo ratings yet
- Methanolic Leaf Extraction of Cogon (POACEAE: Imperata Cylindrica) AS A Potential Alternative Therapeutics For Breast CancerDocument8 pagesMethanolic Leaf Extraction of Cogon (POACEAE: Imperata Cylindrica) AS A Potential Alternative Therapeutics For Breast CancerRechelle CabagingNo ratings yet
- Resume Charlie Castro 2Document13 pagesResume Charlie Castro 2JasonV.PanayNo ratings yet
- Immune Response: Chapter-31 Lesson-3 Page-890-894Document19 pagesImmune Response: Chapter-31 Lesson-3 Page-890-894JanaNo ratings yet
- LetrozoleDocument10 pagesLetrozoleThunnisa SivNo ratings yet
- Quizlet WK 8 NursingDocument5 pagesQuizlet WK 8 NursingWerner Ferman100% (1)
- Questions and Answer Group 3 "Glaucoma" Nama: Gustin Ibrahim Umamah Kelas: A S1 FARMASI 2017 NIM: 821417021Document13 pagesQuestions and Answer Group 3 "Glaucoma" Nama: Gustin Ibrahim Umamah Kelas: A S1 FARMASI 2017 NIM: 821417021Afni YunitaNo ratings yet
- AIDA3 Pool Manual - EnglishDocument97 pagesAIDA3 Pool Manual - EnglishHimar Mendoza MárquezNo ratings yet
- NBNS2604 Psychiatric Mental Health Nursing - Eaug20Document257 pagesNBNS2604 Psychiatric Mental Health Nursing - Eaug20Ranusha Anusha100% (1)
- Moa PCMDocument32 pagesMoa PCMHinaRaviNo ratings yet
- Puerperium Q ADocument2 pagesPuerperium Q AMae Rose Charlene Mendoza100% (1)
- Ijspt 2022 17 3 33151Document13 pagesIjspt 2022 17 3 33151AV Niken AstutiNo ratings yet
- TESDA COVID-19 Health Status Daily Monitoring TESDA COVID - 19 Health Status Daily MonitoringDocument1 pageTESDA COVID-19 Health Status Daily Monitoring TESDA COVID - 19 Health Status Daily MonitoringMICS TVNo ratings yet
- Ciy745 PDFDocument35 pagesCiy745 PDFPhúc LâmNo ratings yet
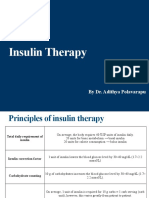
- Insulin Therapy: by Dr. Adithya PolavarapuDocument18 pagesInsulin Therapy: by Dr. Adithya Polavarapuadithya polavarapuNo ratings yet
- Benefits of Butterfly PeaDocument2 pagesBenefits of Butterfly PeaMarie MarsilNo ratings yet
- Test Bank For Clinical Immunology and Serology A Laboratory Perspective 3rd Edition StevensDocument11 pagesTest Bank For Clinical Immunology and Serology A Laboratory Perspective 3rd Edition StevensWilbur Penny100% (40)
- Blood Bank ReportDocument15 pagesBlood Bank Reportsalamon2tNo ratings yet
- Residency Recommended Books - Neurosurgery - NEUROCIRURGIÃO SÃO PAULODocument5 pagesResidency Recommended Books - Neurosurgery - NEUROCIRURGIÃO SÃO PAULOisaacmendonca.sp2No ratings yet
- Application of Interventional RadiologyDocument21 pagesApplication of Interventional RadiologyappleizANo ratings yet
- Patient History Form: Dow Executive CheckupDocument6 pagesPatient History Form: Dow Executive CheckupAkhtar AbbasNo ratings yet
- Dr. Kiki - Pengantar Trauma UpdateDocument20 pagesDr. Kiki - Pengantar Trauma UpdateRsud Malinau Ppk Blud100% (1)
- Diane Kazer Loving On Our LymphDocument22 pagesDiane Kazer Loving On Our LymphKátia BárbaraNo ratings yet
- CHN ComputationDocument3 pagesCHN ComputationRhyann AdvinculaNo ratings yet