Download as pptx, pdf, or txt
You might also like
- EVM Module While On Quarantine - SectionDocument10 pagesEVM Module While On Quarantine - SectionFish BallNo ratings yet
- Clinical Handbook of Infectious Diseases in Farm AnimalsDocument146 pagesClinical Handbook of Infectious Diseases in Farm Animalsigorgalopp100% (1)
- NCP Ineffective Airway ClearanceDocument5 pagesNCP Ineffective Airway ClearanceEmm Estipona HaoNo ratings yet
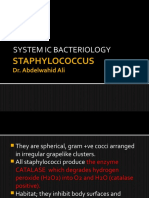
- Gram Positive Cocci StaphylococciDocument41 pagesGram Positive Cocci StaphylococciZainab ElgehaniNo ratings yet
- A. Staphylococcus Aureus B. Staphylococcus Epidermidis C. Staphylococcus SaprophyticusDocument8 pagesA. Staphylococcus Aureus B. Staphylococcus Epidermidis C. Staphylococcus SaprophyticusRuel MaddawinNo ratings yet
- L1 - StaphylococciDocument35 pagesL1 - Staphylococciyouservezeropurpose113No ratings yet
- Gram Positive CocciDocument140 pagesGram Positive CocciBles Cy LagrimasNo ratings yet
- Streptococcus Pneumoniae MbbsDocument53 pagesStreptococcus Pneumoniae MbbsShyam MishraNo ratings yet
- Pyogenic Cocci Pyogenic Means " Pus Forming" Cocci Means "Spherical Bacteria"Document14 pagesPyogenic Cocci Pyogenic Means " Pus Forming" Cocci Means "Spherical Bacteria"Ab AbNo ratings yet
- Bacterial Infections of The SkinDocument9 pagesBacterial Infections of The Skinbeia21No ratings yet
- Staphylococci & MicrococciDocument52 pagesStaphylococci & Micrococcihoneylemon.coNo ratings yet
- S. AureusDocument39 pagesS. AureusRajkishor YadavNo ratings yet
- CB Part 3Document76 pagesCB Part 3Mohammad MambuayNo ratings yet
- staplylococci محاضرة الاولىDocument20 pagesstaplylococci محاضرة الاولىArwa HussienNo ratings yet
- Gram Positive Cocci Sem 1 1Document45 pagesGram Positive Cocci Sem 1 1Charmaine Corpuz Granil100% (1)
- Staphylococcus: Made By: Shalini BishtDocument70 pagesStaphylococcus: Made By: Shalini BishtEduardo SalazarNo ratings yet
- Staphylococcus: Made By: Shalini BishtDocument70 pagesStaphylococcus: Made By: Shalini BishtEduardo SalazarNo ratings yet
- 3.1 Staphylococci PDFDocument36 pages3.1 Staphylococci PDFWong ShuanNo ratings yet
- Staphylococcus Aureus: DR Surender Kaur Asst - Prof. GMCDocument22 pagesStaphylococcus Aureus: DR Surender Kaur Asst - Prof. GMCkaursurenderNo ratings yet
- Chapter 2 Pathogenic Gram Positive CocciDocument76 pagesChapter 2 Pathogenic Gram Positive CocciMubaarįk ÝãřeNo ratings yet
- Staphylococci and StreptococciDocument40 pagesStaphylococci and StreptococciAshwani Mathur, Ma-306100% (1)
- 1.1 Gram Positive CocciDocument9 pages1.1 Gram Positive CocciJustine Mel Concepcion IlardeNo ratings yet
- Complete Bacteriology 240302 021020Document2,416 pagesComplete Bacteriology 240302 021020Usama HameedNo ratings yet
- 34 Staphylococcus - IncompleteDocument9 pages34 Staphylococcus - IncompleteHarshada GhanekarNo ratings yet
- N MeningitidisDocument3 pagesN MeningitidisSajjad Hossain ShuvoNo ratings yet
- 3 Streptococcus: 3.2.1 The Direct Bacteriological Diagnosis in Streptococcal PharyngitisDocument5 pages3 Streptococcus: 3.2.1 The Direct Bacteriological Diagnosis in Streptococcal PharyngitisMahmoud IdlbiNo ratings yet
- 760 Staphylococcus PPT UG LectureDocument47 pages760 Staphylococcus PPT UG Lectureridwan.biotekNo ratings yet
- GRAM Positive CocciDocument67 pagesGRAM Positive CocciNoraine Princess TabangcoraNo ratings yet
- Microbiologia de Murray 8va Edicion-194-227Document34 pagesMicrobiologia de Murray 8va Edicion-194-227Ailyn Montalvo FigueroaNo ratings yet
- Gram Positive Cocci Genus: Staphylococcus SPPDocument9 pagesGram Positive Cocci Genus: Staphylococcus SPPعزوز الراويNo ratings yet
- BacteriologyDocument107 pagesBacteriologyVivek ChaudharyNo ratings yet
- The Staphylococci: Membranes of Humans Others Cause Suppuration, Abscess Formation, A Variety ofDocument18 pagesThe Staphylococci: Membranes of Humans Others Cause Suppuration, Abscess Formation, A Variety ofزين العابدين محمد عويش مشريNo ratings yet
- Gram Positive CocciDocument21 pagesGram Positive CocciRedelle Mae Nini100% (2)
- Staphylococcus: Zeinab Abd Elkhalek Prof. of Medical Microbiology & ImmunologyDocument26 pagesStaphylococcus: Zeinab Abd Elkhalek Prof. of Medical Microbiology & ImmunologyMustafa SaßerNo ratings yet
- G-Positive Non Spore Forminmg Rods-Listeria and Coynebacterium-FinalDocument36 pagesG-Positive Non Spore Forminmg Rods-Listeria and Coynebacterium-FinalDaniel AtiehNo ratings yet
- Strepto Cocci PDFDocument34 pagesStrepto Cocci PDFMustafa SaßerNo ratings yet
- MYCOPLASMA UREAPLASMA LECTURE 2nd Prof MBBS 2012 BatchDocument41 pagesMYCOPLASMA UREAPLASMA LECTURE 2nd Prof MBBS 2012 Batchpodcast gazalNo ratings yet
- Family Micrococcaceae and StreptococcaceaeDocument114 pagesFamily Micrococcaceae and StreptococcaceaeAshwani Mathur, Ma-306No ratings yet
- Lecture2 1hDocument6 pagesLecture2 1hوسيم جمال مياسNo ratings yet
- Gram Positive Cocci The Staphylococci CharacteristicsDocument15 pagesGram Positive Cocci The Staphylococci CharacteristicsKyle PicocNo ratings yet
- 1 - Systemic BacteriologyDocument316 pages1 - Systemic BacteriologyAlsirNo ratings yet
- Practical 4 Staphylococci PresentationDocument24 pagesPractical 4 Staphylococci PresentationPatrisha BuanNo ratings yet
- Gram Positive Bacteria Staphylococci, StreptococciDocument32 pagesGram Positive Bacteria Staphylococci, Streptococcidanishirfan120200No ratings yet
- STREPTOCOCCUSDocument24 pagesSTREPTOCOCCUSTUSHAR MORESHWARNo ratings yet
- Prepared By: Ken Robin A. Canada, RMT, Mls AscpiDocument35 pagesPrepared By: Ken Robin A. Canada, RMT, Mls AscpiKen Robin CanadaNo ratings yet
- Finasls 1 Staph Strep PDFDocument50 pagesFinasls 1 Staph Strep PDFFrancis ValdezNo ratings yet
- PneumococcusDocument29 pagesPneumococcusThe tooth fairyNo ratings yet
- Bacterial Isolation From Wounds-1Document33 pagesBacterial Isolation From Wounds-1Muneez Hussain HameediNo ratings yet
- Bacteriology ReviewDocument128 pagesBacteriology ReviewJoy Adrianne AdisonNo ratings yet
- Infectious DiseasesDocument37 pagesInfectious Diseasespolaris_027No ratings yet
- Pathogenic Gram Positive BacteriaDocument34 pagesPathogenic Gram Positive BacteriaFahimRazmandehNo ratings yet
- Theophilus MicrobDocument4 pagesTheophilus MicrobRaymond NyarkoNo ratings yet
- Lab 6Document5 pagesLab 6moodyNo ratings yet
- Extra Cellular Microbes: DR - Amithbabu.C.B Mscd-EndoDocument35 pagesExtra Cellular Microbes: DR - Amithbabu.C.B Mscd-EndoDR.AMITHBABU.C.BNo ratings yet
- 10 - Bacteria With Unusual GrowthDocument98 pages10 - Bacteria With Unusual GrowthJohanna Kate DiestroNo ratings yet
- Micro KurthDocument47 pagesMicro KurthErika Joille Patayon100% (1)
- Dr. Husni Samadin Mikrobiologi .FK - UnsriDocument125 pagesDr. Husni Samadin Mikrobiologi .FK - UnsriIlham Akbar Ilaker'ErumbiaNo ratings yet
- Gram Positive CocciDocument55 pagesGram Positive CocciAyat MostafaNo ratings yet
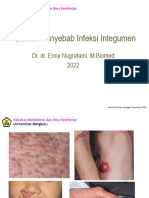
- K20 Infeksi Bakteri Pada Kulit DR DR Enny Nugraheni, M BiomedDocument38 pagesK20 Infeksi Bakteri Pada Kulit DR DR Enny Nugraheni, M BiomedFajar Cristianta GintingNo ratings yet
- Microbiology Medical MicrobiologyDocument40 pagesMicrobiology Medical MicrobiologyAngelic khanNo ratings yet
- The Staphylococci: Lecture SixDocument8 pagesThe Staphylococci: Lecture SixjohnsmithprayNo ratings yet
- Virology and Immunology PracticalDocument6 pagesVirology and Immunology PracticallivehologramNo ratings yet
- World Sleep Day Minitheme by SlidesgoDocument20 pagesWorld Sleep Day Minitheme by SlidesgoTayyaba TahiraNo ratings yet
- Week 2 Topic 1 Pathogenesis and Transmission of Bacterial Infection Copy 06102022 031705pmDocument21 pagesWeek 2 Topic 1 Pathogenesis and Transmission of Bacterial Infection Copy 06102022 031705pmTayyaba TahiraNo ratings yet
- Week 3 - Topic 2 - Antigenic Structures and Virulence Factors of StaphylococciDocument26 pagesWeek 3 - Topic 2 - Antigenic Structures and Virulence Factors of StaphylococciTayyaba TahiraNo ratings yet
- Week 2 - Topic 2 - Bacterial Virulence FactorsDocument24 pagesWeek 2 - Topic 2 - Bacterial Virulence FactorsTayyaba TahiraNo ratings yet
- Week 1-Topic 1-Principles of Diagnostic Medical MicrobiologyDocument27 pagesWeek 1-Topic 1-Principles of Diagnostic Medical MicrobiologyTayyaba TahiraNo ratings yet
- Week 1 - Topic 2 - Diagnostic Tools Used in Identification of Bacterial InfectionsDocument2 pagesWeek 1 - Topic 2 - Diagnostic Tools Used in Identification of Bacterial InfectionsTayyaba TahiraNo ratings yet
- A Comparative Study On Patient Satisfaction Among Public and Private Hospitals in City of Pune, MaharashtraDocument8 pagesA Comparative Study On Patient Satisfaction Among Public and Private Hospitals in City of Pune, MaharashtraSaurav BhowmikNo ratings yet
- Priyanka Pradhan: A Project Work On Study of Pathogenic Bacteria From Brackish Waters of Chilika Lake, OdishaDocument33 pagesPriyanka Pradhan: A Project Work On Study of Pathogenic Bacteria From Brackish Waters of Chilika Lake, Odishapraanya kishoreNo ratings yet
- Cmpa411 Imci Post TestDocument3 pagesCmpa411 Imci Post TestKathleen Dela CruzNo ratings yet
- U-5-Pharyngitis & TonsillitisDocument12 pagesU-5-Pharyngitis & TonsillitisBhawna PandhuNo ratings yet
- 1 Semester: Anti-Migraine Agents Are Used To Treat Migraine HeadachesDocument26 pages1 Semester: Anti-Migraine Agents Are Used To Treat Migraine HeadachesMARY BERNADETTE EGANANo ratings yet
- Department of Health Services: (State Nodal Institution)Document64 pagesDepartment of Health Services: (State Nodal Institution)Amar ChandNo ratings yet
- Pediatric 3 - Answers v1 (Wide)Document56 pagesPediatric 3 - Answers v1 (Wide)Humzala BashamNo ratings yet
- QP Code: Reg - No.: MD Degree Examinations in Community MedicineDocument4 pagesQP Code: Reg - No.: MD Degree Examinations in Community MedicineKumar KPNo ratings yet
- Bailey Scott's Diagnostic Microbiolog13th Ed (Dragged) 2Document1 pageBailey Scott's Diagnostic Microbiolog13th Ed (Dragged) 2Reg LagartejaNo ratings yet
- Lifebuoy Advertisement PDFDocument4 pagesLifebuoy Advertisement PDFNiha RikaNo ratings yet
- JCIMCR v3 1706Document2 pagesJCIMCR v3 1706Mohan ChikkalaNo ratings yet
- Vanessa LeprosyDocument18 pagesVanessa LeprosyMichael Angelo SeñaNo ratings yet
- Vaccines 08 00764Document19 pagesVaccines 08 00764Mai Chi PhạmNo ratings yet
- Application Form WAHSDocument7 pagesApplication Form WAHSAndrit JansenNo ratings yet
- Signs and Symptoms: Abdominal Pain and TendernessDocument6 pagesSigns and Symptoms: Abdominal Pain and TendernessFajriRoziKamarisNo ratings yet
- Delta Memo - COVID-19 UpdateDocument2 pagesDelta Memo - COVID-19 UpdateWTXL ABC27No ratings yet
- Exam in Microbiology and Parasitology I CDocument3 pagesExam in Microbiology and Parasitology I CJoycee Bo100% (2)
- Mycv311lab MergedDocument99 pagesMycv311lab MergedAljohn VillarinNo ratings yet
- La Consolacion College Manila School of Nursing Course SyllabusDocument4 pagesLa Consolacion College Manila School of Nursing Course SyllabusJayson Magdael SalvadorNo ratings yet
- Jurnal PneumoniaDocument2 pagesJurnal PneumoniaSafira R. AissyNo ratings yet
- Group 6 Vaccination Management System of Brgy 6 (Revised)Document72 pagesGroup 6 Vaccination Management System of Brgy 6 (Revised)Ryan Christian MenorNo ratings yet
- Gelsemium Sempervirens: Other Names: Made FromDocument49 pagesGelsemium Sempervirens: Other Names: Made FromDohn JoeNo ratings yet
- Black Death LEQ: Naomi PedigoDocument2 pagesBlack Death LEQ: Naomi PedigoNaomi PedigoNo ratings yet
- Flipbook SummaryDocument5 pagesFlipbook SummaryMario Jr S. FloraNo ratings yet
- Epidemiology The Foundation of Public Health PDFDocument34 pagesEpidemiology The Foundation of Public Health PDFgabe18No ratings yet
- Bird A. - Eliminative Abduction. Examples From MedicineDocument8 pagesBird A. - Eliminative Abduction. Examples From MedicineFede FestaNo ratings yet
- Midterm Module SocSci 111Document40 pagesMidterm Module SocSci 111Frances Georgina FabaleNo ratings yet