Download as pptx, pdf, or txt
You might also like
- References ASEAN2Document3 pagesReferences ASEAN2M IrwaniNo ratings yet
- Design Guide 7 Pinned Base Plate Connections For Columns Contents and Preface Bk745Document7 pagesDesign Guide 7 Pinned Base Plate Connections For Columns Contents and Preface Bk745Hebert Rodriguez0% (8)
- New - 4 - Flares FinalDocument49 pagesNew - 4 - Flares FinalMamdouhAlhanafy83% (12)
- Prevention and Management of MDR-TB in ChildrenDocument32 pagesPrevention and Management of MDR-TB in ChildrenHarpreet SinghNo ratings yet
- Multi-Drug-Resistant Tuberculosis (MDR-TB) Is Defined: EpidemiologyDocument3 pagesMulti-Drug-Resistant Tuberculosis (MDR-TB) Is Defined: EpidemiologyJhemar Handa JulhamidNo ratings yet
- 3.0 Drug ResistanceDocument18 pages3.0 Drug ResistanceMeenachi ChidambaramNo ratings yet
- TB RX Part 4Document30 pagesTB RX Part 4Ibrahim JeldiNo ratings yet
- Mdrtuberculosis DR GyanDocument64 pagesMdrtuberculosis DR GyanSanket AgrawalNo ratings yet
- Drugs Used in Tuberculosis With Recent AdvancesDocument35 pagesDrugs Used in Tuberculosis With Recent AdvancesBindira MaharjanNo ratings yet
- EpiDocument10 pagesEpishenric16100% (1)
- Recent TB Treatment GuidelinesDocument28 pagesRecent TB Treatment GuidelinesDr venkatesh jalluNo ratings yet
- What Is Multidrug-Resistant Tuberculosis (MDR-TB) and How Do We Control It?Document2 pagesWhat Is Multidrug-Resistant Tuberculosis (MDR-TB) and How Do We Control It?Dvica SarahNo ratings yet
- Diagnosing and Treating Latent TB Infection (LTBI) : Module 14 - March 2010Document38 pagesDiagnosing and Treating Latent TB Infection (LTBI) : Module 14 - March 2010wisnu kuncoroNo ratings yet
- WHO - Anti TB Treatment For ChildrenDocument7 pagesWHO - Anti TB Treatment For ChildrenSistya RestuningrumNo ratings yet
- Multi-Drug-resistant Tuberculosis - Wikipedia, The Free EncyclopediaDocument8 pagesMulti-Drug-resistant Tuberculosis - Wikipedia, The Free Encyclopedianayan555No ratings yet
- Communicablediseases 110227001506 Phpapp02 PDFDocument30 pagesCommunicablediseases 110227001506 Phpapp02 PDFCrystal Ann Monsale TadiamonNo ratings yet
- DR José Caminero of The Union On Challenge of anti-TB Resistance in Context of SDGsDocument29 pagesDR José Caminero of The Union On Challenge of anti-TB Resistance in Context of SDGsbobbyramakantNo ratings yet
- Akurit 4 TBDocument14 pagesAkurit 4 TBNicolloNo ratings yet
- TuberculosisDocument28 pagesTuberculosisGuilherme ReisNo ratings yet
- Epidemiology: Isoniazid (INH) Rifampicin (RMP) First-LineDocument14 pagesEpidemiology: Isoniazid (INH) Rifampicin (RMP) First-LineEttedab Abrogar ChavezNo ratings yet
- PTBDocument46 pagesPTBJai AdoraNo ratings yet
- Tata Laksana TB MDR Dr. PrayudiDocument58 pagesTata Laksana TB MDR Dr. PrayudiDeaNo ratings yet
- 16.MDR-XDR TBDocument18 pages16.MDR-XDR TBLinna SriwaningsiNo ratings yet
- TuberculosisDocument20 pagesTuberculosisaditya.3757No ratings yet
- Anti Tubercular DrugsDocument66 pagesAnti Tubercular DrugsKasturiRangan SrivatsaNo ratings yet
- TB Hiv CoinfectionDocument29 pagesTB Hiv CoinfectionVinobhachowdary DondapatiNo ratings yet
- Tuberculosis Management Guidelines and Associated DENTAL Management GuidelinesDocument11 pagesTuberculosis Management Guidelines and Associated DENTAL Management GuidelinesAbdul AkhtarNo ratings yet
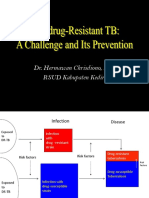
- Dr. Hermawan Chrisdiono, SP.P RSUD Kabupaten KediriDocument48 pagesDr. Hermawan Chrisdiono, SP.P RSUD Kabupaten KediribotolkecapNo ratings yet
- MDR TBDocument8 pagesMDR TBMahira Bayu AdiftaNo ratings yet
- Developments in The Diagnosis & Management of PTBDocument50 pagesDevelopments in The Diagnosis & Management of PTBadamu mohammadNo ratings yet
- Anti-Tuberculosis Treatment: DR Wong VF Sibu GH 27/7/2013Document27 pagesAnti-Tuberculosis Treatment: DR Wong VF Sibu GH 27/7/2013Widy StefannyNo ratings yet
- Case Study For TuberculosisDocument7 pagesCase Study For TuberculosisGabbii CincoNo ratings yet
- DOTS GuidelinesDocument43 pagesDOTS GuidelinesRanjita SantraNo ratings yet
- Multidrug Resistance Tuberculosis in Children: Rina TriasihDocument37 pagesMultidrug Resistance Tuberculosis in Children: Rina Triasihrina triasihNo ratings yet
- BY Dr. Tahmina AzharDocument71 pagesBY Dr. Tahmina Azharscribdnotes123No ratings yet
- Tuberculosis: Dr. Shami Pokhrel Dept. of Pediatrics, LMCDocument37 pagesTuberculosis: Dr. Shami Pokhrel Dept. of Pediatrics, LMCShami PokhrelNo ratings yet
- Adult ImmunizationDocument6 pagesAdult ImmunizationAmit GoelNo ratings yet
- TB 2Document11 pagesTB 2giant nitaNo ratings yet
- 3.0 Drug ResistanceDocument18 pages3.0 Drug ResistanceRey AlwiwikhNo ratings yet
- Tuberculosis 01Document70 pagesTuberculosis 01kurutalaNo ratings yet
- 3.0 Drug ResistanceDocument18 pages3.0 Drug ResistanceMohammed HammedNo ratings yet
- Tuberculosis:Development of New Drugs and Treatment RegimensDocument10 pagesTuberculosis:Development of New Drugs and Treatment RegimensMedylin DualloNo ratings yet
- DotsDocument5 pagesDotsYusephAwangSanaaniNo ratings yet
- Diagnosis and Treatment of Drug-Resistant Tuberculosis-Hermanto QuedarusmanDocument20 pagesDiagnosis and Treatment of Drug-Resistant Tuberculosis-Hermanto QuedarusmanHermanto QuedarusmanNo ratings yet
- Tuberculosis 022007 HartDocument68 pagesTuberculosis 022007 HartWildan HumairahNo ratings yet
- Multidrug Resistant Tuberculosis A Pharmacological View Based On Revised National Tuberculosis Control Programme DOTS-Plus GuidelinesDocument7 pagesMultidrug Resistant Tuberculosis A Pharmacological View Based On Revised National Tuberculosis Control Programme DOTS-Plus GuidelinesIOSR Journal of PharmacyNo ratings yet
- Sem2 Anti TB DrugsDocument35 pagesSem2 Anti TB DrugsZijieNo ratings yet
- Tuberculosis For Dec 1Document23 pagesTuberculosis For Dec 1Tony Rose Reataza-BaylonNo ratings yet
- Treatment of TB in Adults: by Dr. Irfhan Ali Hyder AliDocument45 pagesTreatment of TB in Adults: by Dr. Irfhan Ali Hyder AliInspireGutsNo ratings yet
- Tuberculosis: Forgotten But Not GoneDocument65 pagesTuberculosis: Forgotten But Not GoneNational Press FoundationNo ratings yet
- Homeopathic Perspective in Multi Drug Resistant Pulmonary TuberculosisDocument12 pagesHomeopathic Perspective in Multi Drug Resistant Pulmonary Tuberculosisrenu mittalNo ratings yet
- TUBERKULOSISDocument47 pagesTUBERKULOSISRay SadisNo ratings yet
- Tuberculosis Treatment: General Principles and ApproachDocument24 pagesTuberculosis Treatment: General Principles and ApproachRahul PatilNo ratings yet
- Anti-Tuberculosis DrugsDocument23 pagesAnti-Tuberculosis DrugsemmanuelmkibuniNo ratings yet
- What Is Multidrug-Resistant Tuberculosis (MDR-TB) ?Document63 pagesWhat Is Multidrug-Resistant Tuberculosis (MDR-TB) ?Birhanu AbebeNo ratings yet
- 2018 Article 490Document15 pages2018 Article 490alunnashofiaNo ratings yet
- Rntcp-Revised National Tuberculosis Control ProgrammeDocument29 pagesRntcp-Revised National Tuberculosis Control ProgrammedranshulitrivediNo ratings yet
- The Revised National Tuberculosis Control ProgrammeDocument2 pagesThe Revised National Tuberculosis Control ProgrammesuryaslideNo ratings yet
- Multi-Drug Resistant Tuberculosis (MDR TB)Document2 pagesMulti-Drug Resistant Tuberculosis (MDR TB)Ali AlisonNo ratings yet
- Targeted Tuberculosis (TB) Testing and Treatment of Latent TB InfectionDocument90 pagesTargeted Tuberculosis (TB) Testing and Treatment of Latent TB Infectionwisnu kuncoroNo ratings yet
- You Are Infected and You Don't Even Know It: The Viruses, Bacteria, and Parasites Already Inside YouFrom EverandYou Are Infected and You Don't Even Know It: The Viruses, Bacteria, and Parasites Already Inside YouRating: 5 out of 5 stars5/5 (1)
- A Statistical Inquiry Into the Nature and Treatment of EpilepsyFrom EverandA Statistical Inquiry Into the Nature and Treatment of EpilepsyNo ratings yet
- Health Advice and Immunizations for TravelersFrom EverandHealth Advice and Immunizations for TravelersNo ratings yet
- Chadha1999 PDFDocument9 pagesChadha1999 PDFBárbaraCarrilloNo ratings yet
- LIFESTYLE INTERNATIONAL Private Limited - My Colourful Kitchen 2021-22Document49 pagesLIFESTYLE INTERNATIONAL Private Limited - My Colourful Kitchen 2021-22chaitanya.maisaNo ratings yet
- DLL Science 9 JulyDocument10 pagesDLL Science 9 JulyMark Kiven MartinezNo ratings yet
- Zeiss Erosion ModuleDocument13 pagesZeiss Erosion ModulepakhiddeyasNo ratings yet
- The Making of Self-Disposing Contactless Motion-Activated Trash Bin Using Ultrasonic SensorsDocument7 pagesThe Making of Self-Disposing Contactless Motion-Activated Trash Bin Using Ultrasonic SensorsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 42pt250b Manual ServicioDocument63 pages42pt250b Manual ServicioLuis Carlos Bonilla AldanaNo ratings yet
- 27 To 930Mhz Fsk/Fm/Ask Transceiver FeaturesDocument44 pages27 To 930Mhz Fsk/Fm/Ask Transceiver FeaturesMuhammad Amir YousufNo ratings yet
- Atlas FiltriDocument18 pagesAtlas FiltriCristi CicireanNo ratings yet
- HP 245 G6 Notebook PC: Maintenance and Service GuideDocument106 pagesHP 245 G6 Notebook PC: Maintenance and Service GuideStevenson QuinteroNo ratings yet
- Tech Mahindra Antonyms and QuestionsDocument27 pagesTech Mahindra Antonyms and QuestionsNehaNo ratings yet
- Mobil PajeroDocument2 pagesMobil Pajeroesemelekete wele2No ratings yet
- Hotpoint Washing Machine Wmf740Document16 pagesHotpoint Washing Machine Wmf740furheavensakeNo ratings yet
- DL24MP HDocument13 pagesDL24MP HTamás SzabóNo ratings yet
- Revelation I Excerpt PDFDocument10 pagesRevelation I Excerpt PDFMikhael ChangNo ratings yet
- Techniques For Collection, Isolation and Preservation of MicroorganismsDocument42 pagesTechniques For Collection, Isolation and Preservation of Microorganismsaziskf100% (2)
- Cable HDMI 10 MetrosDocument3 pagesCable HDMI 10 Metroschristian eduardoNo ratings yet
- Turbo Charger - ProjectDocument36 pagesTurbo Charger - ProjectSam Sams100% (2)
- Msds UreaDocument5 pagesMsds UreaHunterlan Register FilanNo ratings yet
- Caffeine in Tea by HPLCDocument3 pagesCaffeine in Tea by HPLCanita_shar29No ratings yet
- Soal OkeDocument12 pagesSoal OkefredyNo ratings yet
- Circut Diagram For GlucometerDocument22 pagesCircut Diagram For GlucometerSaranyaNo ratings yet
- Stresses in Finite Anisotropic Plate Weakened by Rectangular HoleDocument8 pagesStresses in Finite Anisotropic Plate Weakened by Rectangular Holemihir.chauhanNo ratings yet
- Chemistry Practical Procedure Systematic Analysis of Salt STD: Xi & XiiDocument9 pagesChemistry Practical Procedure Systematic Analysis of Salt STD: Xi & XiivarshiniNo ratings yet
- SPAP05A Sevaka - EngDocument7 pagesSPAP05A Sevaka - EngNava NarasimhaNo ratings yet
- SRF PresentationDocument28 pagesSRF PresentationSajeev KumarNo ratings yet
- The Estimation of Drying-Flux Profiles in Continuously Worked DryersDocument3 pagesThe Estimation of Drying-Flux Profiles in Continuously Worked DryerslorencorumbaNo ratings yet
- Guidelines To An Informal LetterDocument3 pagesGuidelines To An Informal LetterNik Syahina0% (1)