Download as pptx, pdf, or txt
You might also like
- Preclinical Anatomy Review 2023: For USMLE Step 1 and COMLEX-USA Level 1From EverandPreclinical Anatomy Review 2023: For USMLE Step 1 and COMLEX-USA Level 1Rating: 5 out of 5 stars5/5 (2)
- EM2.Gametogenesis (At)Document52 pagesEM2.Gametogenesis (At)MUDIN ABDELLANo ratings yet
- Presentation GametogenesisDocument33 pagesPresentation GametogenesisAndy ZempaNo ratings yet
- Significance of MeiosisDocument40 pagesSignificance of MeiosisJovy SanchezNo ratings yet
- The Significance of MeiosisDocument24 pagesThe Significance of MeiosisDiosa BakingNo ratings yet
- OogenesisDocument10 pagesOogenesisOm Prakash SinghNo ratings yet
- Week 6 BiologyDocument3 pagesWeek 6 BiologyKimberly ValsoteNo ratings yet
- Embryo WorksheetDocument9 pagesEmbryo WorksheetDestiny RossNo ratings yet
- Oo GenesisDocument39 pagesOo Genesismayssenbenmaad1970No ratings yet
- EMBRYO Oogenesis, Comparison of GametesDocument20 pagesEMBRYO Oogenesis, Comparison of Gametessolatayesha16No ratings yet
- The Significance of MeiosisDocument5 pagesThe Significance of MeiosisKaren CasternoboNo ratings yet
- 5.1 Female 2023 - JPDocument89 pages5.1 Female 2023 - JPtexasrepublican1976No ratings yet
- EMBRIOLOGYDocument36 pagesEMBRIOLOGYHelena Pascual PérezNo ratings yet
- OogenesisDocument31 pagesOogenesismaryumaziz388No ratings yet
- EMBRYOLOGY Part1Document90 pagesEMBRYOLOGY Part1Daly DaliaNo ratings yet
- EMBRYOLOGY - First Week of Human DevelopmentDocument7 pagesEMBRYOLOGY - First Week of Human DevelopmentMeow CattoNo ratings yet
- Basic Embryology Series PDFDocument252 pagesBasic Embryology Series PDFGrace Nduta0% (1)
- Embryology 1 GametogenesisDocument64 pagesEmbryology 1 Gametogenesiselphas walelaNo ratings yet
- Gametogenesis by Anagha JoseDocument16 pagesGametogenesis by Anagha JoseanaghaNo ratings yet
- Gametogenesis: by Anagha Jose Class - Xii Reg ScienceDocument16 pagesGametogenesis: by Anagha Jose Class - Xii Reg ScienceanaghaNo ratings yet
- Chapter 2 GametogenesisDocument37 pagesChapter 2 GametogenesisAdan ImanNo ratings yet
- Oogenesis Data RawDocument4 pagesOogenesis Data RawMichael Angelo DejandoNo ratings yet
- Human Embryology: Professor of Anatomy and Embryology Faculty of Medicine Hamadan University of Medical SciencesDocument51 pagesHuman Embryology: Professor of Anatomy and Embryology Faculty of Medicine Hamadan University of Medical SciencesGaziza MaaroofNo ratings yet
- Lecture 8 - 30.12.2022Document17 pagesLecture 8 - 30.12.2022Adnan Mohammad Adnan HailatNo ratings yet
- gametogenesis جديد للطلاب - ٠٣٤٠٢٨Document58 pages gametogenesis جديد للطلاب - ٠٣٤٠٢٨Saleh SaddamNo ratings yet
- OogenesisDocument45 pagesOogenesisSabio DenmenNo ratings yet
- ANAT0001 Fertilisation and CleavageDocument7 pagesANAT0001 Fertilisation and CleavageOmed ZarifiNo ratings yet
- Fertilisation Ad ImplantationDocument3 pagesFertilisation Ad ImplantationAine GrahamNo ratings yet
- Nzary El 3maliDocument13 pagesNzary El 3maliGana KhaledNo ratings yet
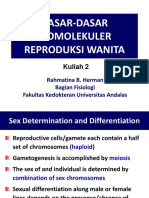
- Dasar2 Biomolekuler Repro WanitaDocument51 pagesDasar2 Biomolekuler Repro WanitaFitriaNo ratings yet
- Gametogenesis:: DR KibeDocument46 pagesGametogenesis:: DR KibeDenis KaguiNo ratings yet
- Game To GenesisDocument48 pagesGame To GenesisJovie Esquivias NicolasNo ratings yet
- Introduction To Embryology.Document24 pagesIntroduction To Embryology.Mercy AdeolaNo ratings yet
- ANAT2341 Student 2015 Quiz QuestionsDocument12 pagesANAT2341 Student 2015 Quiz QuestionsHassan ContehNo ratings yet
- Bimbel MGDocument78 pagesBimbel MGArdi PratamaNo ratings yet
- Fertilization & ImplantationDocument54 pagesFertilization & ImplantationMarvelousNo ratings yet
- h1 Reproductive Physiology Course Summary NotesDocument11 pagesh1 Reproductive Physiology Course Summary NotesHoney BaseriNo ratings yet
- EmbryologyDocument101 pagesEmbryologytawandarukwavamadisonNo ratings yet
- General Embryology PDFDocument9 pagesGeneral Embryology PDFsidhu sNo ratings yet
- G. Embryo FDocument102 pagesG. Embryo FA. AsadiNo ratings yet
- Kelainan GenetikDocument36 pagesKelainan GenetikNicko Erdy Kusuma100% (1)
- Methods of Human GeneticsDocument81 pagesMethods of Human Geneticsfae-ar_raziNo ratings yet
- Maturation of Oocytes Begins at Birth: OogenesisDocument2 pagesMaturation of Oocytes Begins at Birth: OogenesisJoseph MuimiNo ratings yet
- Lec7 Sem1 FMWK3 20140115Document7 pagesLec7 Sem1 FMWK3 20140115Uloko ChristopherNo ratings yet
- Anbt - 608: Submitted ToDocument50 pagesAnbt - 608: Submitted ToMayuriGulhaneNo ratings yet
- 3 Oogenesis DR - GosaiDocument29 pages3 Oogenesis DR - GosaiDr.B.B.GosaiNo ratings yet
- General Biology 1: Quarter 1 - Module 4Document4 pagesGeneral Biology 1: Quarter 1 - Module 4karyo eseymNo ratings yet
- Week 1-2 - Veterinary Embryology IntroductionDocument8 pagesWeek 1-2 - Veterinary Embryology IntroductionAleia GoNo ratings yet
- Oo GenesisDocument20 pagesOo GenesisDinar Yudistira FirdausNo ratings yet
- OogenesisDocument27 pagesOogenesisrukkygodsgiftNo ratings yet
- 1 - Gametogenesis & Early Development of The Fertilized Ovum v2Document1,803 pages1 - Gametogenesis & Early Development of The Fertilized Ovum v2moamen.nlNo ratings yet
- Gammetogenesis in FemaleDocument18 pagesGammetogenesis in FemaleJoyceNo ratings yet
- Craniofacial Biology Notes Unit 1Document37 pagesCraniofacial Biology Notes Unit 1nohacksNo ratings yet
- Meiosis Is The First Step in Gametogenesis: Separation of Homologous Chromosomes Into Haploid Daughter CellsDocument18 pagesMeiosis Is The First Step in Gametogenesis: Separation of Homologous Chromosomes Into Haploid Daughter CellsMichael DiosesNo ratings yet
- Congenital AnomaliesDocument121 pagesCongenital AnomaliesIptisam SwalehNo ratings yet
- Embryology of Cervix & OvaryDocument40 pagesEmbryology of Cervix & Ovaryshrinkhala bhattaraiNo ratings yet
- Fertilization and Implantation-1Document9 pagesFertilization and Implantation-1hussain AltaherNo ratings yet
- DR Anangwe-GametogenesisDocument23 pagesDR Anangwe-GametogenesisStanley OdiraNo ratings yet
- MCN Lec M1L3B ReviewerDocument6 pagesMCN Lec M1L3B ReviewerEmily BernatNo ratings yet
- 01 OogenesisDocument21 pages01 OogenesisMu LokNo ratings yet
- Molecular Regulation and SignalingDocument45 pagesMolecular Regulation and SignalingJovie Esquivias NicolasNo ratings yet
- Introduction To Developmental BiologyDocument32 pagesIntroduction To Developmental BiologyJovie Esquivias NicolasNo ratings yet
- Game To GenesisDocument48 pagesGame To GenesisJovie Esquivias NicolasNo ratings yet
- Ovulation and ImplantationDocument29 pagesOvulation and ImplantationJovie Esquivias NicolasNo ratings yet
- parametruli da araparametruli testebi კვლევაDocument2 pagesparametruli da araparametruli testebi კვლევაAnna JortmenadzeNo ratings yet
- 2015 Health ScienceDocument15 pages2015 Health SciencePharez-david GrantNo ratings yet
- NullDocument8 pagesNullAna Maria MahechaNo ratings yet
- Prolactin OmaDocument3 pagesProlactin OmafynneroNo ratings yet
- Learning Outcomes (KAS) TA Teaching-Learning Activities Method/Learning Materials ResourceDocument5 pagesLearning Outcomes (KAS) TA Teaching-Learning Activities Method/Learning Materials ResourceBevianyl TinapayNo ratings yet
- Normal Delivery Instrument SetsDocument14 pagesNormal Delivery Instrument SetsFrances Kaye Sta. CruzNo ratings yet
- Rupture of Tubal Pregnancy in The Vilnius Population: Pasquale Berlingieri, Grazina Bogdanskiene, Jurgis G. GrudzinskasDocument4 pagesRupture of Tubal Pregnancy in The Vilnius Population: Pasquale Berlingieri, Grazina Bogdanskiene, Jurgis G. Grudzinskaslilis lestariNo ratings yet
- Partido State University: Republic of The Philippines Goa, Camarines SurDocument2 pagesPartido State University: Republic of The Philippines Goa, Camarines SurChano Pacamarra100% (1)
- Bp503t Pcol Unit-VDocument46 pagesBp503t Pcol Unit-VAakkkNo ratings yet
- AI and ET in Mares 2011Document5 pagesAI and ET in Mares 2011Andy jamesNo ratings yet
- Obstetric Emergencies: First - Trimester Pregnancy EmergenciesDocument14 pagesObstetric Emergencies: First - Trimester Pregnancy EmergenciesdianNo ratings yet
- Effect of Obesity On Assisted Reproductive TOG 2017Document8 pagesEffect of Obesity On Assisted Reproductive TOG 2017Muhammad Javed GabaNo ratings yet
- Access To Health 13th Edition Donatelle Test BankDocument38 pagesAccess To Health 13th Edition Donatelle Test Bankorpheussheathy8k6ut100% (15)
- Republic of The PhilippinesDocument6 pagesRepublic of The Philippinescalma3961No ratings yet
- Lesson 5-The Process of ReproductionDocument25 pagesLesson 5-The Process of ReproductionDiana HernandezNo ratings yet
- Characteristics of The Obstetric ForcepsDocument10 pagesCharacteristics of The Obstetric ForcepsNIRANJANA SHALININo ratings yet
- 101 Vitri Kit ProtocolDocument1 page101 Vitri Kit ProtocolNgân Phạm Thị KimNo ratings yet
- Manonmaniam Sundaranar University: B.Sc. Psychology - I YearDocument72 pagesManonmaniam Sundaranar University: B.Sc. Psychology - I Yearhimansu reddyNo ratings yet
- Chart Medical Eligibility Contraceptives EnglishDocument1 pageChart Medical Eligibility Contraceptives EnglishTiang Soon TeckNo ratings yet
- Emergency Contraceptive Pills: Medical and Service Delivery GuidanceDocument24 pagesEmergency Contraceptive Pills: Medical and Service Delivery GuidanceAdityaWijayaNo ratings yet
- 15 Aja 2.0 Handbook 2023Document266 pages15 Aja 2.0 Handbook 2023hcmambayecNo ratings yet
- Study of Adaptability and Efficacy of Menstrual CuDocument10 pagesStudy of Adaptability and Efficacy of Menstrual CuAnnisaaNo ratings yet
- Maternal ExamDocument52 pagesMaternal ExamEdRobertArnad100% (14)
- Gurukula Patasala 10thDocument5 pagesGurukula Patasala 10thPrudhvi Saranya AkulaNo ratings yet
- Female Ejaculation and The G-SpotDocument188 pagesFemale Ejaculation and The G-SpotRui Alves0% (1)
- Full Chapter Manual of Sperm Function Testing in Human Assisted Reproduction 1St Edition Ashok Agarwal Ralf Henkel Ahmad Majzoub PDFDocument54 pagesFull Chapter Manual of Sperm Function Testing in Human Assisted Reproduction 1St Edition Ashok Agarwal Ralf Henkel Ahmad Majzoub PDFjacob.huggard941100% (6)
- Lesson Plan Science 5Document9 pagesLesson Plan Science 5Marj Reña LunaNo ratings yet
- Assisting With Perineal CareDocument33 pagesAssisting With Perineal CareGenki Fay B. LequiganNo ratings yet
- Membangun Kembali Organisasi Berbasis Gerakan: Ippa As A Movement Based OrganizationDocument27 pagesMembangun Kembali Organisasi Berbasis Gerakan: Ippa As A Movement Based OrganizationMuhammad AzkaNo ratings yet
- Chorioamnionitis by DR Simon ByonanuweDocument31 pagesChorioamnionitis by DR Simon ByonanuweDr Simon ByonanuweNo ratings yet