Download as pptx, pdf, or txt
You might also like
- Osce Notes - Myocardial InfarctionDocument10 pagesOsce Notes - Myocardial InfarctionmmmalcampoNo ratings yet
- Cardiovascular Assessment ChecklistDocument2 pagesCardiovascular Assessment Checklistvishnu100% (3)
- Lecture 12 Cardio Intensive CasesDocument32 pagesLecture 12 Cardio Intensive Casesraul0% (1)
- Chapter 5 Cardiovascular EmergenciesDocument6 pagesChapter 5 Cardiovascular Emergenciesعلاء البناءNo ratings yet
- Myocardial Perfusion ScanDocument47 pagesMyocardial Perfusion ScanAkramNo ratings yet
- Pemicu 6 KGD DeniseDocument95 pagesPemicu 6 KGD DeniseVincent VandestyoNo ratings yet
- Ruptured AAA For AnaesthetistsDocument41 pagesRuptured AAA For AnaesthetistsJoe WildNo ratings yet
- Atrial Fibrillation: Key TreatmentsDocument2 pagesAtrial Fibrillation: Key TreatmentschoobiNo ratings yet
- Pericardium PDFDocument50 pagesPericardium PDFRawabi rawabi1997No ratings yet
- Perioperative Care: Nur Azimah Izyan IrdinaDocument42 pagesPerioperative Care: Nur Azimah Izyan IrdinaGx Navin100% (2)
- Stable Ischemic HeartDocument217 pagesStable Ischemic HeartReda SoNo ratings yet
- Myocardial Infarction: Maj Aswathy Ganesh I Year MSC (N) Con, AfmcDocument45 pagesMyocardial Infarction: Maj Aswathy Ganesh I Year MSC (N) Con, AfmcAswathy ganeshNo ratings yet
- CLASS 2 Low Cardiac Output Syndrome in Cardiac SurgeryDocument53 pagesCLASS 2 Low Cardiac Output Syndrome in Cardiac SurgeryjuanolivelloNo ratings yet
- Ob Cardiovascular DisordersDocument10 pagesOb Cardiovascular DisordersJessa Grace GultianoNo ratings yet
- Angiography PDFDocument1 pageAngiography PDFanon_720827871No ratings yet
- Angiography PDFDocument1 pageAngiography PDFanon_720827871No ratings yet
- Ptca PDFDocument1 pagePtca PDFOEDIEN-kmbNo ratings yet
- MINI CP Angina PectorisDocument11 pagesMINI CP Angina Pectorisyasira100% (1)
- Episode 163 Acute Heart Failure Part 1Document8 pagesEpisode 163 Acute Heart Failure Part 1Dk YadavNo ratings yet
- Anesthetic Management of Intracranial Aneurysms R-MasriDocument66 pagesAnesthetic Management of Intracranial Aneurysms R-MasriadheNo ratings yet
- MVR CabgDocument57 pagesMVR CabgRoshani sharma100% (1)
- Shock: Erdiansyah Zulyadaini, MD, FIHA FK Universitas Muhammadiyah Purwokerto/ RSUD Dr. Soeselo Kabupaten TegalDocument47 pagesShock: Erdiansyah Zulyadaini, MD, FIHA FK Universitas Muhammadiyah Purwokerto/ RSUD Dr. Soeselo Kabupaten TegalFarah AkhwanisNo ratings yet
- Abdominal Aortic Aneurysms-EditDocument32 pagesAbdominal Aortic Aneurysms-EditrandikaNo ratings yet
- 02.emergency CardiologyDocument135 pages02.emergency Cardiologyapi-19916399No ratings yet
- Shock and Inotropes With DR Sumesh AroraDocument54 pagesShock and Inotropes With DR Sumesh AroraAhmed AhmedNo ratings yet
- 10.15 Edrian Zulkarnain - ShockDocument42 pages10.15 Edrian Zulkarnain - ShockBintang UbamnataNo ratings yet
- Anestezia in Chirurgia CardiacaDocument179 pagesAnestezia in Chirurgia Cardiacamd.dascalescu2486No ratings yet
- Penyakit Kardiovaskular Yang Sering DijumpaiDocument121 pagesPenyakit Kardiovaskular Yang Sering Dijumpaiandikaagus13No ratings yet
- ShockDocument24 pagesShockYaacub IbrahimNo ratings yet
- Neurologic and Neurosurgical Emergencies For Nursing StudentsDocument39 pagesNeurologic and Neurosurgical Emergencies For Nursing StudentsDr Ganeshgouda MajigoudraNo ratings yet
- CCU Clinical GuidelinesDocument63 pagesCCU Clinical GuidelinesHAMMYER ALROKHAMINo ratings yet
- Kegawatan Jantung - MeDocument41 pagesKegawatan Jantung - MeNam Min BinNo ratings yet
- Basic Cardiac ImagingDocument40 pagesBasic Cardiac ImagingSarah Sy-SantosNo ratings yet
- EmergencyDocument47 pagesEmergencymedstudy123No ratings yet
- Natriuretic Peptide SystemDocument30 pagesNatriuretic Peptide SystemKhaled S. Harb100% (1)
- Journal Presentation: Thrombin-Receptor Antagonist Vorapaxar in Acute Coronary SyndromesDocument16 pagesJournal Presentation: Thrombin-Receptor Antagonist Vorapaxar in Acute Coronary SyndromesStellaNo ratings yet
- Preanesthetic Assessment of Cardiac Patients UndDocument42 pagesPreanesthetic Assessment of Cardiac Patients UndParvathy R NairNo ratings yet
- Acute Lower Extremity Ischaemia (ALEXI) : Nadraj G NaidooDocument25 pagesAcute Lower Extremity Ischaemia (ALEXI) : Nadraj G NaidooVishad NaidooNo ratings yet
- Day 3Document31 pagesDay 3Sara AlramdhanNo ratings yet
- Cardio DiseasesDocument77 pagesCardio Diseasesrea bentayaoNo ratings yet
- Problems of Cardiovascular Function: NUR 222 AWC Cookie'sDocument75 pagesProblems of Cardiovascular Function: NUR 222 AWC Cookie'sKariSilaMarieNo ratings yet
- 3.preoperative Patient Assessment and ManagementDocument76 pages3.preoperative Patient Assessment and Managementoliyad alemayehuNo ratings yet
- Acute Coronary Syndrome - Manchester Students 23.11.2020Document27 pagesAcute Coronary Syndrome - Manchester Students 23.11.2020Dalila ZildžićNo ratings yet
- ShockDocument68 pagesShockseries recapNo ratings yet
- Case Presentation: K/Cof: o HTN o Cerebral Aneurysm S/P Clipping On 1992. o CKD Stage 5Document74 pagesCase Presentation: K/Cof: o HTN o Cerebral Aneurysm S/P Clipping On 1992. o CKD Stage 5Thea DinoNo ratings yet
- PUD KeymessageDocument13 pagesPUD Keymessagenando baehaNo ratings yet
- Assessment of Heart MI NewDocument70 pagesAssessment of Heart MI NewSuzanne AndresNo ratings yet
- Acute HF-IAIDocument49 pagesAcute HF-IAIAndita ListyannisaNo ratings yet
- Peripeheral Artery DiseaseDocument85 pagesPeripeheral Artery DiseaseriniNo ratings yet
- 11 Care of The CV Surgery Patient EmilDocument2 pages11 Care of The CV Surgery Patient EmilameliajamirusNo ratings yet
- Case StudyDocument16 pagesCase StudyArmand Bong Santiago100% (1)
- L15-Shock & Resuscitation LectureDocument49 pagesL15-Shock & Resuscitation LectureYosra —No ratings yet
- Materi Ppds Prep Stroke, Vertigo, ImagingDocument106 pagesMateri Ppds Prep Stroke, Vertigo, Imagingintanurpratiwi4No ratings yet
- Revascularization On Bilateral Renal Artery Stenosis - Rifqi AryaDocument15 pagesRevascularization On Bilateral Renal Artery Stenosis - Rifqi Aryazakiyyatul aflakhaNo ratings yet
- CardiologyDocument8 pagesCardiologyMa. Kristina Cazandra IbañezNo ratings yet
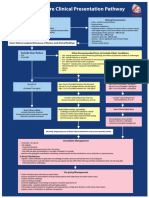
- Heart Failure Clinical Presentation PathwayDocument1 pageHeart Failure Clinical Presentation PathwayJesse Helmut Hansen-BartelNo ratings yet
- ACC Fellows Echo Board ReviewDocument160 pagesACC Fellows Echo Board Reviewdr.bedussa.nhNo ratings yet
- Model Answer -I & II سبتمبر 2015تحريريDocument12 pagesModel Answer -I & II سبتمبر 2015تحريريAmr El TaherNo ratings yet
- Angina Pectoris: Stable Angina Unstable AnginaDocument3 pagesAngina Pectoris: Stable Angina Unstable AnginaDanesa MadoNo ratings yet
- The Ideal Heart Healthy Diet Cookbook; The Superb Diet Guide To Lower Your Blood Pressure And Cholesterol Levels With Nutritious Low Sodium Low Fat RecipesFrom EverandThe Ideal Heart Healthy Diet Cookbook; The Superb Diet Guide To Lower Your Blood Pressure And Cholesterol Levels With Nutritious Low Sodium Low Fat RecipesNo ratings yet
- Cardiology-5 DysrhythmiaDocument16 pagesCardiology-5 DysrhythmiaMahmoud RamadanNo ratings yet
- Cardiovascular 9. Acute Myocardial InfarctionDocument39 pagesCardiovascular 9. Acute Myocardial Infarctionapi-19641337100% (2)
- Epidemiology, Risk Factors, Pathogenesis, and Natural History of Thoracic Aortic AneurysmDocument5 pagesEpidemiology, Risk Factors, Pathogenesis, and Natural History of Thoracic Aortic AneurysmNathaliazuosNo ratings yet
- Heart Sounds PDFDocument38 pagesHeart Sounds PDFZennon Blaze ArceusNo ratings yet
- AneurysmDocument7 pagesAneurysmLillabinNo ratings yet
- Cardio-Vascular ExaminationDocument43 pagesCardio-Vascular ExaminationDimas FrasesaNo ratings yet
- Internal Medicine Case Studies BMHDocument4 pagesInternal Medicine Case Studies BMHParsaant SinghNo ratings yet
- Daftar PustakaDocument9 pagesDaftar Pustakaaajeng ftnyNo ratings yet
- Hi-Yield Notes in Im & PediaDocument20 pagesHi-Yield Notes in Im & PediaJohn Christopher LucesNo ratings yet
- ECG ReviewingDocument50 pagesECG ReviewingLutfir Rahman TarisNo ratings yet
- Radiology Packet 7 Congenital Cardiac DiseaseDocument27 pagesRadiology Packet 7 Congenital Cardiac Diseaseludiegues752No ratings yet
- Atherosclerosis and Coronary Artery Disease AtherosclerosisDocument8 pagesAtherosclerosis and Coronary Artery Disease Atherosclerosiskarim mohamedNo ratings yet
- Case Report STEMI Inferior PosteriorDocument38 pagesCase Report STEMI Inferior PosteriorNorazeela BaharudinNo ratings yet
- KROK 2-CardioDocument12 pagesKROK 2-CardioberdaderagaNo ratings yet
- Imei Cardiac DiseaseDocument4 pagesImei Cardiac DiseaseMakNo ratings yet
- 12 Lead EKG Interpretation PDFDocument251 pages12 Lead EKG Interpretation PDFRobert So JrNo ratings yet
- Heart and Neck Vessels AssessmentDocument66 pagesHeart and Neck Vessels Assessmentmarianneladislao07No ratings yet
- Congenital Heart DiseaseDocument2 pagesCongenital Heart Diseasejhayviec0% (1)
- Dr. Senthil Priya Heart Disease in Pregnancy FINALDocument68 pagesDr. Senthil Priya Heart Disease in Pregnancy FINALKai ParkerNo ratings yet
- Angina PectorisDocument4 pagesAngina PectorisJohiarra Madanglog TabigneNo ratings yet
- HEART MURMURS by NISHDocument41 pagesHEART MURMURS by NISHurtikikeNo ratings yet
- Mitral Valve RepairDocument109 pagesMitral Valve RepairheldhiNo ratings yet
- Laporan SP3 LB1 2021 DMDocument1 pageLaporan SP3 LB1 2021 DMfitra rezaNo ratings yet
- MANIFESTASI KLINIK Penyakit Jantung KoronerDocument4 pagesMANIFESTASI KLINIK Penyakit Jantung KoronerDwitya NoviariNo ratings yet
- ACSDocument56 pagesACSGabriel CalderónNo ratings yet
- Pathophysiology NSTEMI 2022Document14 pagesPathophysiology NSTEMI 2022usmlesteveNo ratings yet
- Soal MCQ Dari EJVESDocument4 pagesSoal MCQ Dari EJVESAnonymous 7I3ns1zTCNo ratings yet
- Daftar PustakaDocument3 pagesDaftar Pustakasinta merlinda yuniNo ratings yet