Download as ppt, pdf, or txt
You might also like
- Poultry Farming Ebook 2Document14 pagesPoultry Farming Ebook 2irmaNo ratings yet
- Whipple ProcedureDocument8 pagesWhipple ProcedureDae AhmadNo ratings yet
- Lymphatic Drainage of The Head and Neck - AatifDocument6 pagesLymphatic Drainage of The Head and Neck - AatifAatif AnsariNo ratings yet
- Lymphatic Drainage of Head and NeckDocument60 pagesLymphatic Drainage of Head and NeckKhadija VasiNo ratings yet
- LundeeriaDocument79 pagesLundeeriaAmitabha100% (2)
- Biomedic (Myology)Document19 pagesBiomedic (Myology)Sadam_fasterNo ratings yet
- Manual Lymph DrainageDocument2 pagesManual Lymph DrainageChetna Kanchan Bhagat100% (1)
- Ennio Nimis - Kriya Yoga - Synthesis of A Personal Experience IDocument76 pagesEnnio Nimis - Kriya Yoga - Synthesis of A Personal Experience IJdM2012No ratings yet
- Upper Limb BreastDocument40 pagesUpper Limb BreastewijayapalaNo ratings yet
- Lymph Drainage For DetoxificationDocument8 pagesLymph Drainage For DetoxificationJay JonesNo ratings yet
- Peritoneum: General FeaturesDocument92 pagesPeritoneum: General FeaturestuhinsinghNo ratings yet
- Anatomy of The NeckDocument34 pagesAnatomy of The NeckAsma AlamoudiNo ratings yet
- Lesser Omentum Project: Penny Fleming Kimberly BurnhamDocument32 pagesLesser Omentum Project: Penny Fleming Kimberly BurnhamspiraldaoNo ratings yet
- 4) Mammary Gland 220413 Upnm2Document22 pages4) Mammary Gland 220413 Upnm2AaronMaroonFive100% (1)
- Islamic Code of LifeDocument2 pagesIslamic Code of LifewaqarNo ratings yet
- Anatomy - Lymphatic Drainage Handwritten NotesDocument4 pagesAnatomy - Lymphatic Drainage Handwritten NotesMrunal DoiphodeNo ratings yet
- Ana 201 (Axilla N Axillary Artery) - 1Document119 pagesAna 201 (Axilla N Axillary Artery) - 1Favour OnyeaboNo ratings yet
- Lymphatic System 7thDocument14 pagesLymphatic System 7thAna Sofia Pinzón UlloaNo ratings yet
- Examination of Cerebrospinal FluidDocument25 pagesExamination of Cerebrospinal FluidKhalid IbrahimNo ratings yet
- Peripheral CirculationDocument27 pagesPeripheral CirculationRachel ThomsonNo ratings yet
- Lecture 19 - Vessels and CirculationDocument67 pagesLecture 19 - Vessels and CirculationSasikala MohanNo ratings yet
- Colorectal MalignancyDocument108 pagesColorectal MalignancySatishht SatishNo ratings yet
- Integration and Coordination - SG3Document180 pagesIntegration and Coordination - SG3Marcos AlbaridaNo ratings yet
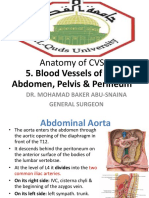
- Anatomy of CVS: 5. Blood Vessels of The Abdomen, Pelvis & PerineumDocument30 pagesAnatomy of CVS: 5. Blood Vessels of The Abdomen, Pelvis & Perineumsultan khabeebNo ratings yet
- Istology: Lymphatic SystemDocument48 pagesIstology: Lymphatic Systemninja-2001No ratings yet
- The Lymphatic SystemDocument23 pagesThe Lymphatic SystemMERIDIAN SEESNo ratings yet
- Dna and Rna Powerpoint 2Document46 pagesDna and Rna Powerpoint 2api-267309851No ratings yet
- Endocrine System NotesDocument23 pagesEndocrine System NoteslacyNo ratings yet
- Health Death Full Incarnation of The Spirit/ Disincarnatination of The SpiritDocument3 pagesHealth Death Full Incarnation of The Spirit/ Disincarnatination of The SpiritKalmer KaruNo ratings yet
- Skin and Its AppendagesDocument28 pagesSkin and Its AppendagesTK Balbin Liquit100% (1)
- Massage and Soft Tissue TechniquesDocument15 pagesMassage and Soft Tissue TechniquesBenruNo ratings yet
- 16-Genital ProlapseDocument37 pages16-Genital Prolapseapi-3703352No ratings yet
- DNA TopoisomerasesDocument61 pagesDNA TopoisomerasesBabak NamiNo ratings yet
- Lymphatic Organs and TissuesDocument3 pagesLymphatic Organs and TissuesSaman Bharatha KotigalaNo ratings yet
- Manual Lymphatic Drainage Versus Exercise in The Early PostoperativeDocument7 pagesManual Lymphatic Drainage Versus Exercise in The Early PostoperativeSofia Adão da FonsecaNo ratings yet
- ChaosDocument9 pagesChaosTim WengenmayrNo ratings yet
- 9 Anterior Triangle of The Neck E-LearningDocument22 pages9 Anterior Triangle of The Neck E-LearningHashim GhazoNo ratings yet
- Medicinal MushroomsDocument4 pagesMedicinal MushroomsRavenzDDNo ratings yet
- Holistic Therapy Part 1Document8 pagesHolistic Therapy Part 1Engy MoneebNo ratings yet
- Body Cavities PPT & Anatomical SystemDocument10 pagesBody Cavities PPT & Anatomical Systemnandhini raguNo ratings yet
- Genital ProlapseDocument9 pagesGenital Prolapsesher singhNo ratings yet
- Dr. Reynaldo V. Lopez Senior Lecturer Department of AnatomyDocument55 pagesDr. Reynaldo V. Lopez Senior Lecturer Department of AnatomyMohammad AliNo ratings yet
- Case 5 - Embryology of AppendixDocument3 pagesCase 5 - Embryology of Appendixshilviadevi100% (1)
- How I Evaluate The Neck Lymph NodesDocument29 pagesHow I Evaluate The Neck Lymph NodesMartín Avellaneda SantoméNo ratings yet
- Anatomy and Physiology of The Lymphatic SystemDocument153 pagesAnatomy and Physiology of The Lymphatic SystemNellie Grace Montes Aba-aNo ratings yet
- Emily Iker, MD: LymphedemaDocument37 pagesEmily Iker, MD: LymphedemaJustin HarperNo ratings yet
- Spermatogenesis, OogenesisDocument16 pagesSpermatogenesis, Oogenesisannita100% (1)
- Brain and Neural NetworksDocument17 pagesBrain and Neural NetworksKristyle BalagosaNo ratings yet
- Respiratory Examination - Protected 1Document4 pagesRespiratory Examination - Protected 1anirudh811100% (1)
- The Physic Body MechanicsDocument8 pagesThe Physic Body MechanicsNur RasyiqahNo ratings yet
- Micro Endocrine OrgansDocument8 pagesMicro Endocrine OrgansMonica100% (1)
- 5 - Anatomy of The BreastDocument18 pages5 - Anatomy of The Breasthabtsh habshaNo ratings yet
- The Role of Cupping Therapy in Pain Management A LDocument19 pagesThe Role of Cupping Therapy in Pain Management A LMohitha Parla100% (1)
- Femoral Region, Anterior and Medial Compartments of The ThighDocument49 pagesFemoral Region, Anterior and Medial Compartments of The ThighNolanNo ratings yet
- Lymphatic System and Immune SystemDocument4 pagesLymphatic System and Immune SystemKyle Labor100% (1)
- LymphedemaDocument4 pagesLymphedemaSAKAI69No ratings yet
- Thoracic Wall.Document48 pagesThoracic Wall.Shimmering MoonNo ratings yet
- Breast Health Handbook and Medical Thermography: Healthy Happy BreastsFrom EverandBreast Health Handbook and Medical Thermography: Healthy Happy BreastsNo ratings yet
- An Introduction to Pain and its relation to Nervous System DisordersFrom EverandAn Introduction to Pain and its relation to Nervous System DisordersAnna A. BattagliaNo ratings yet
- Examination of The Neck ModifiedDocument30 pagesExamination of The Neck ModifiedMenna AhmedNo ratings yet
- Enbloc Left ZMC #Document20 pagesEnbloc Left ZMC #Mehek BatraNo ratings yet
- Diagnosis Tests For Carcinoma CervixDocument5 pagesDiagnosis Tests For Carcinoma CervixMehek BatraNo ratings yet
- Panfacial Trauma (1) .PPT (Autosaved)Document96 pagesPanfacial Trauma (1) .PPT (Autosaved)Mehek BatraNo ratings yet
- Panfacial TraumaDocument104 pagesPanfacial TraumaMehek BatraNo ratings yet
- Diagnosis of ImpactionDocument33 pagesDiagnosis of ImpactionMehek BatraNo ratings yet
- Lymphatic DrainageDocument49 pagesLymphatic DrainageMehek BatraNo ratings yet
- JC 1-CompressedDocument21 pagesJC 1-CompressedMehek BatraNo ratings yet
- EthicsDocument54 pagesEthicsMehek BatraNo ratings yet
- Basic Principles of SurgDocument56 pagesBasic Principles of SurgMehek BatraNo ratings yet
- Clinical Presentation of Diabetic FootDocument13 pagesClinical Presentation of Diabetic FootMehek BatraNo ratings yet
- Jurnal Data P4GN 2012 - Edisi 2013 - ENDocument262 pagesJurnal Data P4GN 2012 - Edisi 2013 - ENAnti NarkobaNo ratings yet
- Scanning Electron Microscope (SEM) (The Analysis of Enamel Remineralization Increase in Pure Soy Milk (Glycine Max (L.) Merill) Immersion Using Scanning Electron Microscope (SEM) )Document5 pagesScanning Electron Microscope (SEM) (The Analysis of Enamel Remineralization Increase in Pure Soy Milk (Glycine Max (L.) Merill) Immersion Using Scanning Electron Microscope (SEM) )Sarah Ariefah SantriNo ratings yet
- Stress and Adaptation Crisis and Its InterventionDocument27 pagesStress and Adaptation Crisis and Its InterventionPuy Puy ChhangteNo ratings yet
- UntitledDocument125 pagesUntitledSunni Gallegos100% (1)
- Characteristics of Cognitive in Children With LearDocument6 pagesCharacteristics of Cognitive in Children With LearNampatnampat 6969No ratings yet
- 12/07/20 3PM-11PM: Fdar ChartingDocument5 pages12/07/20 3PM-11PM: Fdar ChartingElle ctricaNo ratings yet
- Internal Exam Dairy Chemistry May - June 2021 (Responses)Document12 pagesInternal Exam Dairy Chemistry May - June 2021 (Responses)pawaryogeshNo ratings yet
- Documents As of 2021 08 15 ISTDocument9 pagesDocuments As of 2021 08 15 ISTprakashNo ratings yet
- Anganwadi Workers - Midhun Varghese-2Document17 pagesAnganwadi Workers - Midhun Varghese-2FEBIN RAJUNo ratings yet
- Woodhead 2004Document18 pagesWoodhead 2004andris88No ratings yet
- MCN Normal AntepartumDocument9 pagesMCN Normal AntepartumCHARLHYN GRACE BISNARNo ratings yet
- 3.review of Literature PDFDocument38 pages3.review of Literature PDFJalajarani AridassNo ratings yet
- Appendix B Achilles Tendinopathy: Low Level Laser Therapy Dosage CalculationDocument1 pageAppendix B Achilles Tendinopathy: Low Level Laser Therapy Dosage CalculationManpreet SandhuNo ratings yet
- HL 7 Q3 08 Mental Health and Stress SW1Document3 pagesHL 7 Q3 08 Mental Health and Stress SW1glydel.pototNo ratings yet
- Glossary of NICU Medical Terms FINAL 19-02-2019Document7 pagesGlossary of NICU Medical Terms FINAL 19-02-2019Diulia SantanaNo ratings yet
- Anaesthesia, Pharmacology, Intensive Care and Emergency A.P.I.C.E PDFDocument253 pagesAnaesthesia, Pharmacology, Intensive Care and Emergency A.P.I.C.E PDFRatheesh KumarNo ratings yet
- Protinex RevDocument2 pagesProtinex Revnilesh patilNo ratings yet
- LO Week 5 Tutorial 2Document7 pagesLO Week 5 Tutorial 2Hizkia MarlissaNo ratings yet
- Nicotinic Acid (Or Niacin) & Nicotinamide (Or Niacinamide)Document3 pagesNicotinic Acid (Or Niacin) & Nicotinamide (Or Niacinamide)Jann ericka JaoNo ratings yet
- Pre EclampsiaDocument179 pagesPre EclampsiaAnton RossiniNo ratings yet
- PubertyDocument6 pagesPubertyNata LiaNo ratings yet
- Research Paper of Deep Learning Based Frameworks by IIT GuwahatiDocument18 pagesResearch Paper of Deep Learning Based Frameworks by IIT GuwahatiPrasad SangameshwaranNo ratings yet
- Nurses 05-2023Document81 pagesNurses 05-2023PRC BaguioNo ratings yet
- Renal Disease in PregnancyDocument28 pagesRenal Disease in PregnancysuperjaxxxonNo ratings yet
- Sabyasachi Panda's LetterDocument40 pagesSabyasachi Panda's LetterThenewsminuteNo ratings yet
- Treatment, Prevention and Control of Intestinal Parasitic InfectionDocument49 pagesTreatment, Prevention and Control of Intestinal Parasitic InfectiononilaNo ratings yet
- In Primary Care: Chronic Kidney Disease (CKD)Document4 pagesIn Primary Care: Chronic Kidney Disease (CKD)NotForAbuseNo ratings yet
- Rotamat® Rok 4 Pumping Stations Screen: WasteDocument4 pagesRotamat® Rok 4 Pumping Stations Screen: WastecrvenicajNo ratings yet
- Tiqqun - 1999 - Machine-Men - User's GuideDocument15 pagesTiqqun - 1999 - Machine-Men - User's Guidesleslie100% (2)