Download as pptx, pdf, or txt
You might also like
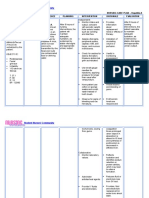
- Nursingcrib Com NURSING CARE PLAN Hepatitis ADocument2 pagesNursingcrib Com NURSING CARE PLAN Hepatitis APravesh Verma100% (1)
- #03 Signaling Mechanism Pharmacodynamics Vers 2Document57 pages#03 Signaling Mechanism Pharmacodynamics Vers 2tasnemaldaherNo ratings yet
- Cell SignalingDocument53 pagesCell SignalingKaushiki KalravNo ratings yet
- Mechanism of Hormone ActionDocument30 pagesMechanism of Hormone ActionWhite SnelliNo ratings yet
- General Principles of Metabolism Regulation. HormonesDocument90 pagesGeneral Principles of Metabolism Regulation. HormonesМохіт Кумар ЯмпатіNo ratings yet
- Endocrinology 1st TrimesterDocument16 pagesEndocrinology 1st TrimesteriwennieNo ratings yet
- Endocrine Lec-1Document73 pagesEndocrine Lec-1suriNo ratings yet
- Endocrine System: HCCA 123: Clinical Chemistry 17Document51 pagesEndocrine System: HCCA 123: Clinical Chemistry 17Gutu Garemewu BiruNo ratings yet
- Pharmacodynamics Mechanisms of Drug ActionDocument47 pagesPharmacodynamics Mechanisms of Drug ActioneciNo ratings yet
- P ('t':'3', 'I':'3053532947') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document45 pagesP ('t':'3', 'I':'3053532947') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Affandi AkbarNo ratings yet
- 4-Introduction To Endocrinology 4Document30 pages4-Introduction To Endocrinology 4tmqt2fbnzgNo ratings yet
- Endo Lect - OverviewDocument24 pagesEndo Lect - OverviewdoctorrfarrukhNo ratings yet
- 1 - Hormonal Signal Transduction 2Document43 pages1 - Hormonal Signal Transduction 2Mohammed Mansour AbdullahNo ratings yet
- 4.2 Mechanism of Action of Hormones-40Document39 pages4.2 Mechanism of Action of Hormones-40Namomsa W.No ratings yet
- PHARMACODYNAMICS ReceptorsDocument11 pagesPHARMACODYNAMICS ReceptorsMandyNo ratings yet
- Cell and Molecular Biology: Gerald KarpDocument53 pagesCell and Molecular Biology: Gerald Karppat ongNo ratings yet
- ReceptorsDocument16 pagesReceptorsM HarisNo ratings yet
- Principles of Endocrinology Szathmari Miklos 2010Document25 pagesPrinciples of Endocrinology Szathmari Miklos 2010Ryan James Lorenzo MiguelNo ratings yet
- AS211 Endocrinology Lecture Notes1Document102 pagesAS211 Endocrinology Lecture Notes1John MkotaNo ratings yet
- Endocrine Physiology: Dale Buchanan Hales, PHD Department of Physiology & BiophysicsDocument64 pagesEndocrine Physiology: Dale Buchanan Hales, PHD Department of Physiology & Biophysicshamako02No ratings yet
- Intracellular SignallingDocument45 pagesIntracellular Signallingsana iqbalNo ratings yet
- Ligand and Cell Signaling PathwaysDocument117 pagesLigand and Cell Signaling PathwaysShoaib MomenNo ratings yet
- Hormone ActionDocument142 pagesHormone ActionAnand Veeranan100% (1)
- Endocrine BiochemDocument130 pagesEndocrine BiochemDessu AshagrieNo ratings yet
- 15 1acidsDocument55 pages15 1acidsNEELAMNo ratings yet
- Receptor Mechanisms: - Receptor Are Proteins With High Affinity To ADocument45 pagesReceptor Mechanisms: - Receptor Are Proteins With High Affinity To AbevorsiNo ratings yet
- Endocrine Physiology: Dale Buchanan Hales, PHD Department of Physiology & BiophysicsDocument64 pagesEndocrine Physiology: Dale Buchanan Hales, PHD Department of Physiology & BiophysicsHello SunshineNo ratings yet
- Receptor-Ligand Interactions - Cell Signaling, Adhesion, Motility, Cell MigrationDocument31 pagesReceptor-Ligand Interactions - Cell Signaling, Adhesion, Motility, Cell MigrationLeebo PinPinNo ratings yet
- HormoneDocument7 pagesHormonedonna26royNo ratings yet
- E N D o C R I N o L o G Y: Dr. Victoria G. Giango Chair, Dept. of PhysiologyDocument23 pagesE N D o C R I N o L o G Y: Dr. Victoria G. Giango Chair, Dept. of Physiologyanon-271548No ratings yet
- ACyMSC - 03-Surface ReceptorsDocument54 pagesACyMSC - 03-Surface ReceptorsEsther NavarroNo ratings yet
- Basic EndocrinologyDocument43 pagesBasic EndocrinologyAnanya MajilaNo ratings yet
- Mechanisms of Drug ActionDocument29 pagesMechanisms of Drug ActionKAMAU FRANCIS GATHUTHINo ratings yet
- Hormones (Complete)Document75 pagesHormones (Complete)muhammadahsan660393No ratings yet
- CH 18 Endocrine3Document65 pagesCH 18 Endocrine3adamaditya666No ratings yet
- Anatomy and Physiology,: Lecture OutlineDocument79 pagesAnatomy and Physiology,: Lecture OutlineJorelyn Giron NaniongNo ratings yet
- Physical Chemistry of Drug Receptor InteractionDocument30 pagesPhysical Chemistry of Drug Receptor Interactionmaun04No ratings yet
- Receptors & Signal TransductionDocument10 pagesReceptors & Signal TransductionArslan SaeedNo ratings yet
- FarmakodinamikDocument44 pagesFarmakodinamikHarri HardiNo ratings yet
- Mecanism of Action of Hormones 9.6.20Document46 pagesMecanism of Action of Hormones 9.6.20Mohammad ZayanNo ratings yet
- Plant PromotersDocument43 pagesPlant PromotersSreejesh P CNo ratings yet
- Signaling Pathways1189Document26 pagesSignaling Pathways1189Mehedi HossainNo ratings yet
- 2 ola hormon peptidaDocument21 pages2 ola hormon peptidaMirahAvishaNo ratings yet
- General Pharmacodynamics 2022-1Document49 pagesGeneral Pharmacodynamics 2022-1Rashid LancerNo ratings yet
- Hormone FinalDocument36 pagesHormone FinalRajkishor YadavNo ratings yet
- SerotoninsDocument14 pagesSerotoninsRaja AffanNo ratings yet
- Introduction Endocrine Physiology 2Document52 pagesIntroduction Endocrine Physiology 2IshaqNo ratings yet
- Mechanism of Action of HormonesDocument33 pagesMechanism of Action of HormonesMehwishNo ratings yet
- Endocrine Control LecDocument71 pagesEndocrine Control LecTri Andini ALNo ratings yet
- Intercellular Communication: Cell and Molecular PhysiologyDocument30 pagesIntercellular Communication: Cell and Molecular PhysiologyO'Brien AlfredNo ratings yet
- General Principles of Endocrine Physiology: Vaclav - Hampl@lf2.cuni - CZDocument45 pagesGeneral Principles of Endocrine Physiology: Vaclav - Hampl@lf2.cuni - CZfrankminNo ratings yet
- Lecture 2Document28 pagesLecture 2Ushan KabirNo ratings yet
- Pharmacodynamics: DR Narendra KumarDocument76 pagesPharmacodynamics: DR Narendra Kumarperala vinaykumarNo ratings yet
- 24 Cellular SignalingDocument37 pages24 Cellular SignalingGian BanaresNo ratings yet
- ENDOCRINOLOGY in Orthodontics - Dr. HibaDocument86 pagesENDOCRINOLOGY in Orthodontics - Dr. HibaHiba AbdullahNo ratings yet
- Lecture 4Document32 pagesLecture 4Muhanad Shahin100% (1)
- Lecture 9 Part 1Document33 pagesLecture 9 Part 1Kimberly GrahamNo ratings yet
- In The Blood Substance Is Too Low, It Stimulates Neuron Directly Stimulates The GlandDocument19 pagesIn The Blood Substance Is Too Low, It Stimulates Neuron Directly Stimulates The GlandRishtaul AlamNo ratings yet
- Cell SignalingDocument75 pagesCell SignalingjhanvisNo ratings yet
- Senescencia Celular - Una Perspectiva Traslacional - Traducción AutomáticaDocument7 pagesSenescencia Celular - Una Perspectiva Traslacional - Traducción AutomáticaEduardo MartelNo ratings yet
- Coagulation StudyDocument57 pagesCoagulation Studytanweer_elevenNo ratings yet
- Hyperthyroidism and ThyrotoxicosisDocument33 pagesHyperthyroidism and Thyrotoxicosiseze033No ratings yet
- Leukemias & Lymphomas - HY USMLEDocument87 pagesLeukemias & Lymphomas - HY USMLEMatt McGlothlinNo ratings yet
- Clinical Significance of Bilirubin in Liver Function TestsDocument24 pagesClinical Significance of Bilirubin in Liver Function TestsAbdulsalam JumaiNo ratings yet
- CME Examination DermatologyDocument25 pagesCME Examination DermatologylimeddyNo ratings yet
- Ekb 4293 Green & Sustainable Chemical Process: 12 Principles of Green Chemistry Principle 1: PreventionDocument15 pagesEkb 4293 Green & Sustainable Chemical Process: 12 Principles of Green Chemistry Principle 1: PreventionMark Antony LevineNo ratings yet
- Nutrients 06 01782Document27 pagesNutrients 06 01782jasonc13No ratings yet
- SemaxDocument7 pagesSemaxblazewindNo ratings yet
- 2019.-Human Germ Cell Tumours From A Developmental PerspectiveDocument16 pages2019.-Human Germ Cell Tumours From A Developmental PerspectiveAbraham Escobedo MorenoNo ratings yet
- Genetic Variation:: Horizontal Gene TransferDocument39 pagesGenetic Variation:: Horizontal Gene TransferMaria RosaNo ratings yet
- Brianbee Sample Questions 1 PDFDocument2 pagesBrianbee Sample Questions 1 PDFLigeia100% (1)
- History of The SADS Foundation and Long QT SyndromeDocument4 pagesHistory of The SADS Foundation and Long QT Syndromeapi-341217779No ratings yet
- Chapter # 1: 1.1statement of The ProblemDocument12 pagesChapter # 1: 1.1statement of The ProblemShams Ud Din SahitoNo ratings yet
- Art 08Document6 pagesArt 08RicardoBlasNo ratings yet
- LiposomesDocument58 pagesLiposomesBharath Chinna100% (1)
- Case Study - Endocrine System PDFDocument3 pagesCase Study - Endocrine System PDFYusra Angel DelfinNo ratings yet
- The History and Scope of Microbiology: Prof. Khaled H. Abu-Elteen Hashemite UniversityDocument61 pagesThe History and Scope of Microbiology: Prof. Khaled H. Abu-Elteen Hashemite UniversityPaulo GanNo ratings yet
- Agricultural Resource BaseDocument34 pagesAgricultural Resource BaseVenus AnteroNo ratings yet
- Laboratory Test Report: Test Name Result Sars-Cov-2 (RDRP Gene)Document1 pageLaboratory Test Report: Test Name Result Sars-Cov-2 (RDRP Gene)srinathNo ratings yet
- Part 1: Listen To The Recording Twice. Complete The Table Below. Write ONEDocument19 pagesPart 1: Listen To The Recording Twice. Complete The Table Below. Write ONEyamedagomenasaiNo ratings yet
- Final Draft Research Essay 4Document12 pagesFinal Draft Research Essay 4api-451599260No ratings yet
- Evaluation and Management of Primary Amenorrhea - UpToDateDocument11 pagesEvaluation and Management of Primary Amenorrhea - UpToDateNatasya SugiantoNo ratings yet
- 3.2 Acid Fast StainingDocument26 pages3.2 Acid Fast StainingMiguel CuevasNo ratings yet
- CH 2 & 3 - Theories and PrenatalDocument21 pagesCH 2 & 3 - Theories and PrenatalScribdNo ratings yet
- Understanding The Pathophysiology of Fever.45Document2 pagesUnderstanding The Pathophysiology of Fever.45drdion mangku alamNo ratings yet
- (Answer Key) Written Competency ReticulocytesDocument25 pages(Answer Key) Written Competency ReticulocytessaharNo ratings yet
- Contrabending and Reverse Twist As A Basic Biomechanical Force To Correct Deformity in Scoliosis (Revision) Docx PDFDocument11 pagesContrabending and Reverse Twist As A Basic Biomechanical Force To Correct Deformity in Scoliosis (Revision) Docx PDFFahmi AnshoriNo ratings yet
- Male ReproductionDocument88 pagesMale ReproductionBlackHerbalsNo ratings yet