Download as ppt, pdf, or txt
You might also like
- 18d Nls Use Manual EnglishDocument136 pages18d Nls Use Manual Englishneo carty100% (1)
- BTB Template Er-IntakeDocument3 pagesBTB Template Er-IntakeBoy MadNo ratings yet
- DictationDocument6 pagesDictationlizNo ratings yet
- PMDC Index Pakistan of Recognized JournalsDocument3 pagesPMDC Index Pakistan of Recognized JournalsAhmed MateenNo ratings yet
- Antipsychotic DrugsDocument47 pagesAntipsychotic DrugsIkram UddinNo ratings yet
- AntideprresentDocument54 pagesAntideprresentHadiqa KhanNo ratings yet
- Antipsychotic or Neuroleptic DrugsDocument12 pagesAntipsychotic or Neuroleptic Drugscamile buhanginNo ratings yet
- Drug Classification Indication Action and Pharmacokinetics Contraindication Adverse Effect Monitoring ParameterDocument5 pagesDrug Classification Indication Action and Pharmacokinetics Contraindication Adverse Effect Monitoring ParameteryssatNo ratings yet
- Sudden Onset (Within 2 Weeks) of at Least One of TheDocument2 pagesSudden Onset (Within 2 Weeks) of at Least One of TheNeicole BandalaNo ratings yet
- Neuroleptic Advers ReactionDocument65 pagesNeuroleptic Advers Reactionayu yulianti100% (1)
- Se 04 Abpsych PDFDocument27 pagesSe 04 Abpsych PDFBea SengcoNo ratings yet
- Midterm Psych Module 7Document14 pagesMidterm Psych Module 7Ladybelle GototosNo ratings yet
- Psychiatry Notes - Defenses MechanismsDocument2 pagesPsychiatry Notes - Defenses MechanismsLiSenNo ratings yet
- Case Study in Stahl S Essential PsychophDocument5 pagesCase Study in Stahl S Essential PsychophJessica ChavesNo ratings yet
- Treatment Resistant OCD .Document55 pagesTreatment Resistant OCD .Dr viren SolankiNo ratings yet
- PA 644 - M2 LecturesDocument412 pagesPA 644 - M2 LectureskatNo ratings yet
- Gaba Systems in PsychiatryDocument49 pagesGaba Systems in PsychiatryMATHANKUMAR ENo ratings yet
- Depression in Older Adults: A Treatable Medical ConditionDocument12 pagesDepression in Older Adults: A Treatable Medical ConditionJose Alonso Aguilar Valera100% (1)
- Introduction To NeuropharmacologyDocument6 pagesIntroduction To Neuropharmacologyammarhafez78100% (1)
- The RX Files: QT Prolongation and Torsades de Pointes: Drugs and Sudden DeathDocument2 pagesThe RX Files: QT Prolongation and Torsades de Pointes: Drugs and Sudden DeathRahul RaiNo ratings yet
- Lecture No. 3 Semiology of Psychiatry Part 2Document26 pagesLecture No. 3 Semiology of Psychiatry Part 2ozgur.yonlukNo ratings yet
- Approach To A Case of Respiratoey SystemDocument105 pagesApproach To A Case of Respiratoey SystemprashuNo ratings yet
- Anti PsychoticDocument1 pageAnti PsychoticbeautyNo ratings yet
- Nicotine Related DisordersDocument74 pagesNicotine Related DisordersKuldeep singhNo ratings yet
- Neuroleptics & AnxiolyticsDocument65 pagesNeuroleptics & AnxiolyticsAntonPurpurov100% (1)
- Bipolar Disorder PamphletDocument2 pagesBipolar Disorder Pamphletapi-3134075020% (1)
- Psychiatric Medications in Pregnancy and LactationDocument27 pagesPsychiatric Medications in Pregnancy and LactationSunija SelvamNo ratings yet
- 4 - Anti-Psychotics-Redi (Nema)Document40 pages4 - Anti-Psychotics-Redi (Nema)Endre Shitaye KulkiNo ratings yet
- Consultationliaison Psychiatry IcuDocument56 pagesConsultationliaison Psychiatry IcuChrisAlipioNo ratings yet
- Receptors Ionchannel TransporterDocument58 pagesReceptors Ionchannel TransporterDeepu Vijay100% (1)
- Study Guide Test 1Document11 pagesStudy Guide Test 1jwasylow13No ratings yet
- Substance Use DisordersDocument28 pagesSubstance Use DisordersAbdul NazarNo ratings yet
- APA - DSM5 - Severity Measure For Panic Disorder Adult PDFDocument3 pagesAPA - DSM5 - Severity Measure For Panic Disorder Adult PDFMelissandreNo ratings yet
- Psychiatric Agents: By: Paula Rose Mae Cuario Evita Lalaine Del Mundo Dennis Ragudo Sheena ZarsueloDocument80 pagesPsychiatric Agents: By: Paula Rose Mae Cuario Evita Lalaine Del Mundo Dennis Ragudo Sheena ZarsueloDennis RagudoNo ratings yet
- Mood Stablizing AgentsDocument15 pagesMood Stablizing AgentsDhAiRyA ArOrANo ratings yet
- Psychiatric Interview Kap ExtDocument61 pagesPsychiatric Interview Kap ExtNeba Yenatu100% (1)
- Antidepressant Therapy AlgorithmDocument12 pagesAntidepressant Therapy AlgorithmZubair Mahmood KamalNo ratings yet
- B /G C U I R: Anti-PsychoticsDocument2 pagesB /G C U I R: Anti-PsychoticsErsy Sakti ilhamNo ratings yet
- Approach To Aggressive PatientsDocument25 pagesApproach To Aggressive PatientsdocshahirNo ratings yet
- Terms in The Field of PsychiatryDocument18 pagesTerms in The Field of PsychiatryOchie YecyecanNo ratings yet
- Short Guide To Psychiatric DrugsDocument17 pagesShort Guide To Psychiatric Drugsjaume1010No ratings yet
- Drugs For NeurolepticsDocument1 pageDrugs For Neurolepticssyamil_daudNo ratings yet
- Bipolar and Related DisordersDocument31 pagesBipolar and Related DisordersNoelle Grace Ulep BaromanNo ratings yet
- Psychiatric Visit1 - AaronVer3Document1 pagePsychiatric Visit1 - AaronVer3api-3764308No ratings yet
- Handbook of Psychiatry 2021 v2 Sample 1Document73 pagesHandbook of Psychiatry 2021 v2 Sample 1Dragutin PetrićNo ratings yet
- Terms in The Field of Psychiatry and NeurologyDocument25 pagesTerms in The Field of Psychiatry and NeurologyMarlon SigfredNo ratings yet
- Antipsychotic DrugsDocument54 pagesAntipsychotic DrugsJackNo ratings yet
- My Basal GangliaDocument18 pagesMy Basal GangliaPriya GKNo ratings yet
- Anti-Psychotic Drugs: Submitted ToDocument28 pagesAnti-Psychotic Drugs: Submitted Torho 998No ratings yet
- Antidepressants: I. Cyclic AntidepressantDocument17 pagesAntidepressants: I. Cyclic AntidepressantVaibhav KrishnaNo ratings yet
- Antipsychotic Drugs - Wafa Bin ShamlanDocument8 pagesAntipsychotic Drugs - Wafa Bin ShamlanSara AbdoNo ratings yet
- Dr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American UniversityDocument41 pagesDr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American Universityredderdat100% (1)
- Psych Ch. 7 Notes (Tutor)Document5 pagesPsych Ch. 7 Notes (Tutor)Haylle ThomasNo ratings yet
- Clinical Features of Common Psychiatric DisordersDocument21 pagesClinical Features of Common Psychiatric DisordersShivan A.C.No ratings yet
- AntipsychoticsDocument22 pagesAntipsychoticsvinodksahuNo ratings yet
- Psych Meds 2Document2 pagesPsych Meds 2Cole SchaferNo ratings yet
- HPI GuidelinesDocument5 pagesHPI GuidelinesHani NadiahNo ratings yet
- Joshua Dodot Case StudyDocument2 pagesJoshua Dodot Case StudyJoshua Ringor100% (1)
- Psycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsDocument29 pagesPsycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsPoonam RanaNo ratings yet
- Neuroleptic Malignant SyndromeDocument11 pagesNeuroleptic Malignant SyndromeRhomizal MazaliNo ratings yet
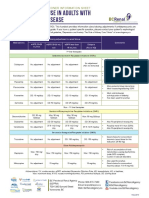
- Antidepressant Use in Adults With Chronic Kidney DiseaseDocument1 pageAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- Drugs Used in Mental IllnessDocument60 pagesDrugs Used in Mental IllnessDixa MeNo ratings yet
- A Literature Review On Improving Nurse-Patient Communication ManuDocument23 pagesA Literature Review On Improving Nurse-Patient Communication ManuMontero, Ma. Cecilia - BSN 3-BNo ratings yet
- MENTAL STATUS EXAM PowerpointDocument35 pagesMENTAL STATUS EXAM PowerpointMontero, Ma. Cecilia - BSN 3-BNo ratings yet
- SLAB MusculoskeletalCareModalitiesDocument47 pagesSLAB MusculoskeletalCareModalitiesMontero, Ma. Cecilia - BSN 3-BNo ratings yet
- Paracentesis and ColostomyDocument20 pagesParacentesis and ColostomyMontero, Ma. Cecilia - BSN 3-BNo ratings yet
- CHOLELITHIASISDocument3 pagesCHOLELITHIASISMontero, Ma. Cecilia - BSN 3-BNo ratings yet
- 10 000 Reasons Bless The Lord LyricsDocument1 page10 000 Reasons Bless The Lord LyricsMontero, Ma. Cecilia - BSN 3-BNo ratings yet
- 16 Survivors of Violence and Trauma and Child and Adolescent PsychiatricDocument4 pages16 Survivors of Violence and Trauma and Child and Adolescent PsychiatricMontero, Ma. Cecilia - BSN 3-BNo ratings yet
- Models For Working With Psychiatric PatientsDocument2 pagesModels For Working With Psychiatric PatientsMontero, Ma. Cecilia - BSN 3-BNo ratings yet
- Therapeutic Communication 1Document48 pagesTherapeutic Communication 1Montero, Ma. Cecilia - BSN 3-BNo ratings yet
- MMDST FormDocument1 pageMMDST FormMontero, Ma. Cecilia - BSN 3-BNo ratings yet
- 6 COMMUNICABLE DISEASES Nies PDocument14 pages6 COMMUNICABLE DISEASES Nies PMontero, Ma. Cecilia - BSN 3-BNo ratings yet
- Case Study 4 Drug StudyDocument9 pagesCase Study 4 Drug StudyMontero, Ma. Cecilia - BSN 3-BNo ratings yet
- Drug StudyDocument5 pagesDrug StudyMontero, Ma. Cecilia - BSN 3-BNo ratings yet
- DRUG STUDY FOR HYPOKALEMIA Case Study 3Document11 pagesDRUG STUDY FOR HYPOKALEMIA Case Study 3Montero, Ma. Cecilia - BSN 3-BNo ratings yet
- Process Recording Form 1 1Document4 pagesProcess Recording Form 1 1Montero, Ma. Cecilia - BSN 3-BNo ratings yet
- EndocrineDocument49 pagesEndocrineApsaraNo ratings yet
- 180510-Jf-STARS Blackout Checklist FINALDocument6 pages180510-Jf-STARS Blackout Checklist FINALNithyaNo ratings yet
- Metabolic Syndrome - WikipediaDocument119 pagesMetabolic Syndrome - WikipediaMudassar SattarNo ratings yet
- PUBH6000 Social Determinants of HealthDocument4 pagesPUBH6000 Social Determinants of HealthAna MariaNo ratings yet
- London Cancer Lung Radiotherapy Guidelines 2013 v1 0Document24 pagesLondon Cancer Lung Radiotherapy Guidelines 2013 v1 0Cosmin SaftaNo ratings yet
- Afp 20140501 P 731Document8 pagesAfp 20140501 P 731metabolismeproteinNo ratings yet
- Jurding Saraf Koja - Manitol - Margaretha HDocument24 pagesJurding Saraf Koja - Manitol - Margaretha HMargaretha HimawanNo ratings yet
- Tumours of The Central Nervous System: FM Brett MD., FrcpathDocument57 pagesTumours of The Central Nervous System: FM Brett MD., FrcpathRerendhutNo ratings yet
- Ipsen Announces FDA Approval of A New Delivery Device For Somatuline® Depot® (Lanreotide) PFS InjectionDocument6 pagesIpsen Announces FDA Approval of A New Delivery Device For Somatuline® Depot® (Lanreotide) PFS Injectionraju1559405No ratings yet
- Style Guide - NCDJDocument11 pagesStyle Guide - NCDJVaishnavi JayakumarNo ratings yet
- Papanicolaou StainDocument2 pagesPapanicolaou StaindeblackaNo ratings yet
- Peptic Ulcer Disease (PUD) EditedDocument9 pagesPeptic Ulcer Disease (PUD) EditedRashed ShatnawiNo ratings yet
- Classification of Handicapped ConditionsDocument23 pagesClassification of Handicapped ConditionsVaishakhi BaisaneNo ratings yet
- The Effectiveness of Pre-Operative Deep BreathingDocument5 pagesThe Effectiveness of Pre-Operative Deep BreathingJulenda CintarinovaNo ratings yet
- Books Shalakya TantraDocument4 pagesBooks Shalakya TantraSambamurthi Punninnair Narayan75% (4)
- Pricelist MonotestDocument3 pagesPricelist MonotestMimi AnugrahNo ratings yet
- Consanguinity As A Significant Risk Factor For Diabetes Mellitus: A Systematic ReviewDocument8 pagesConsanguinity As A Significant Risk Factor For Diabetes Mellitus: A Systematic ReviewIJAR JOURNALNo ratings yet
- Icd 10Document78 pagesIcd 10KumarNo ratings yet
- Studiu Cancer ColonDocument9 pagesStudiu Cancer ColonCatalina CalinNo ratings yet
- GI MAP Interpretive GuideDocument52 pagesGI MAP Interpretive GuidedulceomNo ratings yet
- Care Plan Worksheet Mental Health 2022Document3 pagesCare Plan Worksheet Mental Health 2022tahani.mah147No ratings yet
- تجميعات شهر مارس EmsDocument11 pagesتجميعات شهر مارس EmsMohamed MahmoudNo ratings yet
- Proctocolectomy: Without Ileostomy For Ulcerative ColitisDocument4 pagesProctocolectomy: Without Ileostomy For Ulcerative ColitisAlexandra constantinNo ratings yet
- Position PaperDocument4 pagesPosition PaperBing Cossid Quinones CatzNo ratings yet
- Catch Up FridayDocument4 pagesCatch Up FridayMa. Phoebe AlleoNo ratings yet
- Multiple Myeloma Patient Education Manual: October 2007 EditionDocument85 pagesMultiple Myeloma Patient Education Manual: October 2007 EditionKareem WaheedNo ratings yet
- Guidelines On Aesthetic Medical Practice For Registered Medical PractitionersDocument47 pagesGuidelines On Aesthetic Medical Practice For Registered Medical Practitionerszahisma8950% (2)
- Antibiotic Optimization in CIAIDocument33 pagesAntibiotic Optimization in CIAIAditya Pradana KNo ratings yet