
Psychopharmacology in Medically Ill Patients
Psychopharmacology in Medically Ill Patients
You might also like
- Aa - LMR Georgette - Final VersionDocument47 pagesAa - LMR Georgette - Final Versionpickles.squad11No ratings yet
- PSYCH EOR EXAM QsDocument2 pagesPSYCH EOR EXAM Qskhalil bryant100% (1)
- Lab Monitoring For Psychiatric Medications: Reference TableDocument1 pageLab Monitoring For Psychiatric Medications: Reference TableTimothy Turscak100% (2)
- BTB Template Er-IntakeDocument3 pagesBTB Template Er-IntakeBoy MadNo ratings yet
- Second and Third Generation Antipsychotics: A Comprehensive HandbookFrom EverandSecond and Third Generation Antipsychotics: A Comprehensive HandbookRating: 5 out of 5 stars5/5 (1)
- Psychiatry HX TakingDocument4 pagesPsychiatry HX TakingP KasikrishnarajaNo ratings yet
- Psychotropic Medications During PregnancyDocument20 pagesPsychotropic Medications During PregnancyMaria Von ShaftNo ratings yet
- Psychopharmacologic Drugs: - Antipsychotic Agents - Antimanic Drugs - Antidepressant DrugsDocument18 pagesPsychopharmacologic Drugs: - Antipsychotic Agents - Antimanic Drugs - Antidepressant DrugsDrima EdiNo ratings yet
- Chronic Headache 2019 PDFDocument398 pagesChronic Headache 2019 PDFDaniel SisniegasNo ratings yet
- Laboratory Testing in PsychiatryDocument29 pagesLaboratory Testing in PsychiatrySera ChunNo ratings yet
- Antipsychotic DrugsDocument54 pagesAntipsychotic DrugsJackNo ratings yet
- PMHNP Case Study - EditedDocument7 pagesPMHNP Case Study - EditedSoumyadeep BoseNo ratings yet
- Laboratory Monitoring When Prescribing PsychotropicsDocument5 pagesLaboratory Monitoring When Prescribing PsychotropicswaleskacrzNo ratings yet
- Lab TestsDocument1 pageLab TestsnkivcNo ratings yet
- Shortened REM Latency and Increased REM: Previous AttemptDocument19 pagesShortened REM Latency and Increased REM: Previous AttemptActeen MyoseenNo ratings yet
- Final FY Presentation1Document45 pagesFinal FY Presentation1SamNo ratings yet
- The RX Files: QT Prolongation and Torsades de Pointes: Drugs and Sudden DeathDocument2 pagesThe RX Files: QT Prolongation and Torsades de Pointes: Drugs and Sudden DeathRahul RaiNo ratings yet
- Psychiatry Made EasyDocument14 pagesPsychiatry Made EasyD. W. S JayarathnaNo ratings yet
- 1: Adhd: Scientific Name Dose CommentsDocument4 pages1: Adhd: Scientific Name Dose CommentsSadiq Abdo92No ratings yet
- Varun Kumar, 2017 - Getting Started in PsychiatryDocument148 pagesVarun Kumar, 2017 - Getting Started in PsychiatryBernard FZ100% (1)
- AntipsychoticsDocument10 pagesAntipsychoticswawing16No ratings yet
- AnxietyDocument4 pagesAnxietyIT’S ME HAYLANo ratings yet
- Quick Reference Guide FallDocument62 pagesQuick Reference Guide FallKreshnik IdrizajNo ratings yet
- Antipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationDocument6 pagesAntipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationJaylord Verazon100% (1)
- Antidepressant Therapy AlgorithmDocument12 pagesAntidepressant Therapy AlgorithmZubair Mahmood KamalNo ratings yet
- HPI GuidelinesDocument5 pagesHPI GuidelinesHani NadiahNo ratings yet
- 504 - Pediatric Psychopharmacology - General PrinciplesDocument54 pages504 - Pediatric Psychopharmacology - General PrinciplesAlvaro HuidobroNo ratings yet
- Drugs For NeurolepticsDocument1 pageDrugs For Neurolepticssyamil_daudNo ratings yet
- Malingering NbiDocument5 pagesMalingering NbiPridina SyadirahNo ratings yet
- Risk Assessment Decision TreeDocument1 pageRisk Assessment Decision TreeHeather RamettaNo ratings yet
- Translate Kaplan Sadock Sinopsis Psikiatri Komprehensif Halaman 721 730 PDF FreeDocument76 pagesTranslate Kaplan Sadock Sinopsis Psikiatri Komprehensif Halaman 721 730 PDF FreeHadi GunaNo ratings yet
- B /G C U I R: Anti-PsychoticsDocument2 pagesB /G C U I R: Anti-PsychoticsErsy Sakti ilhamNo ratings yet
- Terms in The Field of Psychiatry and NeurologyDocument25 pagesTerms in The Field of Psychiatry and NeurologyMarlon SigfredNo ratings yet
- PsychopharmacologyDocument148 pagesPsychopharmacologyAsther Mantua100% (2)
- Pediatric Psychopharmacology: General PrinciplesDocument55 pagesPediatric Psychopharmacology: General PrinciplesAlvaro HuidobroNo ratings yet
- Psychotropic Drugs.Document15 pagesPsychotropic Drugs.Xiaoqing SongNo ratings yet
- Practical Notebook Adult PsychiatryDocument121 pagesPractical Notebook Adult PsychiatryCarly DyaNo ratings yet
- Structured Approach To Acute Psychiatry EmergenciesDocument41 pagesStructured Approach To Acute Psychiatry EmergenciesRaimondo RomanazziNo ratings yet
- Pharmacology - (5) Psychotic DrugsDocument8 pagesPharmacology - (5) Psychotic DrugsSamantha DiegoNo ratings yet
- Neuroleptic Advers ReactionDocument65 pagesNeuroleptic Advers Reactionayu yulianti100% (1)
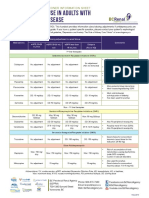
- Antidepressant Use in Adults With Chronic Kidney DiseaseDocument1 pageAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- Pharmacological Management of DepressionDocument66 pagesPharmacological Management of DepressionPriyash JainNo ratings yet
- Psychiatric Interview (Autosaved)Document22 pagesPsychiatric Interview (Autosaved)Jana Victor100% (1)
- Psychiatric Visit1 - AaronVer3Document1 pagePsychiatric Visit1 - AaronVer3api-3764308No ratings yet
- Clozapine Care GuideDocument16 pagesClozapine Care GuideERWIN SUMARDINo ratings yet
- Psychiatry History & Suicide Risk Assessment TemplatesDocument32 pagesPsychiatry History & Suicide Risk Assessment TemplatesDuncan Jackson100% (2)
- MMP Handy Chart October 2011 V2Document69 pagesMMP Handy Chart October 2011 V2Icha IchaNo ratings yet
- SCTL NeurotransmitterDocument32 pagesSCTL Neurotransmitternur qistina humaira zulkarshamsiNo ratings yet
- Psychiatric Medications in Pregnancy and LactationDocument27 pagesPsychiatric Medications in Pregnancy and LactationSunija SelvamNo ratings yet
- The BrainDocument22 pagesThe BrainClae NapiNo ratings yet
- Handy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Document3 pagesHandy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Mariya ZhekovaNo ratings yet
- Week 2 (OSCE CASC Book II 2018-19) 03.09.2018Document48 pagesWeek 2 (OSCE CASC Book II 2018-19) 03.09.2018Andrew WdsmithNo ratings yet
- Psychiatry Notes Psychiatry Notes: Medicine (Queen Mary University of London) Medicine (Queen Mary University of London)Document28 pagesPsychiatry Notes Psychiatry Notes: Medicine (Queen Mary University of London) Medicine (Queen Mary University of London)Noman ButtNo ratings yet
- Study Guide Test 1Document11 pagesStudy Guide Test 1jwasylow13No ratings yet
- Psychiatry Grand NotesDocument10 pagesPsychiatry Grand NotesNathan T. CheungNo ratings yet
- BTB Template Er-IntakeDocument3 pagesBTB Template Er-IntakehectorNo ratings yet
- Adhd Toolkit MedicationsDocument1 pageAdhd Toolkit MedicationsreneezNo ratings yet
- Reviewer On PsychopharmacologyDocument28 pagesReviewer On PsychopharmacologyKristine Ann Hernandez100% (1)
- Long-Acting Injectable AntipsychoticsDocument18 pagesLong-Acting Injectable AntipsychoticsMia BlackattNo ratings yet
- Psychiatry Notes - Defenses MechanismsDocument2 pagesPsychiatry Notes - Defenses MechanismsLiSenNo ratings yet
- Mania: Carbamazepine, Valproic AcidDocument16 pagesMania: Carbamazepine, Valproic AcidKylie Elaine100% (1)
- Introduction To NeuropharmacologyDocument6 pagesIntroduction To Neuropharmacologyammarhafez78100% (1)
- Postpartum Psychiatric DisordersDocument55 pagesPostpartum Psychiatric DisordersAklile TsegaNo ratings yet
- Academic StressDocument5 pagesAcademic StressAklile TsegaNo ratings yet
- DeliriumDocument40 pagesDeliriumAklile TsegaNo ratings yet
- Quality of LifeDocument27 pagesQuality of LifeAklile TsegaNo ratings yet
- Nihms 446239Document9 pagesNihms 446239Aklile TsegaNo ratings yet
- Mubarek Aplied Neuroscience PPT Lecture NoteDocument50 pagesMubarek Aplied Neuroscience PPT Lecture NoteAklile TsegaNo ratings yet
- AssignmentDocument29 pagesAssignmentAklile TsegaNo ratings yet
- Psychiatric EmergencyDocument88 pagesPsychiatric EmergencyAklile TsegaNo ratings yet
- Country Focus Document Orange Knowledge ProgrammeDocument12 pagesCountry Focus Document Orange Knowledge ProgrammeAklile TsegaNo ratings yet
- Fpsyt 13 843984Document10 pagesFpsyt 13 843984Aklile TsegaNo ratings yet
- Higher Diploma Program A Centrally Initiated and Successfully Institutionalized Professional Development Program For Teachers in Ethiopian PublicDocument26 pagesHigher Diploma Program A Centrally Initiated and Successfully Institutionalized Professional Development Program For Teachers in Ethiopian PublicAklile TsegaNo ratings yet
- Almaz Mamaru Counseling Psychologist (BA, MA) Department of Psychiatry, Bahardar UniversityDocument39 pagesAlmaz Mamaru Counseling Psychologist (BA, MA) Department of Psychiatry, Bahardar UniversityAklile TsegaNo ratings yet
- NRR 328749 The Magnitude of Perceived Professionalism and Its AssociateDocument10 pagesNRR 328749 The Magnitude of Perceived Professionalism and Its AssociateAklile TsegaNo ratings yet
- Direct and Indirect Aggression in Intimate Relationships in Mexico and FinlandDocument1 pageDirect and Indirect Aggression in Intimate Relationships in Mexico and FinlandAklile TsegaNo ratings yet
- Conduct Disorder Diagnosis & TreatmentDocument13 pagesConduct Disorder Diagnosis & TreatmentAklile TsegaNo ratings yet
- Interpersonal Psychotherapy (IPT)Document39 pagesInterpersonal Psychotherapy (IPT)Aklile TsegaNo ratings yet
- Prevalence of Aggression, Antisocial Behaviors, and SuicideDocument18 pagesPrevalence of Aggression, Antisocial Behaviors, and SuicideAklile TsegaNo ratings yet
- Behavioral Therapies: Hailemariam Hailesilassie (Asst - Professor) Department of Psychiatry, FMS, JUDocument21 pagesBehavioral Therapies: Hailemariam Hailesilassie (Asst - Professor) Department of Psychiatry, FMS, JUAklile TsegaNo ratings yet
- Cognitive Behavior Therapy: Hailemariam Hailesilassie (Assist - Professor) Department of Psychiatry Jimma UniversityDocument109 pagesCognitive Behavior Therapy: Hailemariam Hailesilassie (Assist - Professor) Department of Psychiatry Jimma UniversityAklile TsegaNo ratings yet
- Eye Movement Desensitization Reprocessing Therapy (EMDR)Document48 pagesEye Movement Desensitization Reprocessing Therapy (EMDR)Aklile TsegaNo ratings yet
- Acceptance and Commitment Therapy (ACT)Document36 pagesAcceptance and Commitment Therapy (ACT)Aklile TsegaNo ratings yet
- Almaz Mamaru BA, MA (Counseling Psychology) Department of Psychiatry Collage of Medicine Health Science Bahardar UniversityDocument37 pagesAlmaz Mamaru BA, MA (Counseling Psychology) Department of Psychiatry Collage of Medicine Health Science Bahardar UniversityAklile TsegaNo ratings yet
- Bahirdar University College of Medicine and Health Science Department of Psychiatry Mood Disorder Assignment FEB 2020Document25 pagesBahirdar University College of Medicine and Health Science Department of Psychiatry Mood Disorder Assignment FEB 2020Aklile TsegaNo ratings yet
- Cognitive Behavioral Therapy Training in Core SkillsDocument65 pagesCognitive Behavioral Therapy Training in Core SkillsAklile TsegaNo ratings yet
- DoubleDocument25 pagesDoubleAklile TsegaNo ratings yet
- Nter-Ersonal HerapyDocument46 pagesNter-Ersonal HerapyAklile TsegaNo ratings yet
- Diversity Primer Chapter 04Document11 pagesDiversity Primer Chapter 04Aklile TsegaNo ratings yet
- Child and Adolescent Psychiatry AssignmentDocument3 pagesChild and Adolescent Psychiatry AssignmentAklile TsegaNo ratings yet
- Pharmacology Related To Psychiatric NursingDocument7 pagesPharmacology Related To Psychiatric NursingGlenn Daryll SantosNo ratings yet
- MCQS Dr. Aalia New 31 October 2008Document4 pagesMCQS Dr. Aalia New 31 October 2008rawalianNo ratings yet
- DigoxinDocument6 pagesDigoxinSEIYADU IBRAHIM KNo ratings yet
- Adult ADHD - What Do When Your First Drug Fails - Dr.-James-LazowskiDocument77 pagesAdult ADHD - What Do When Your First Drug Fails - Dr.-James-LazowskiJason WongNo ratings yet
- Falls in Older Persons - Risk Factors and Patient Evaluation - UpToDateDocument24 pagesFalls in Older Persons - Risk Factors and Patient Evaluation - UpToDateNhungVũNo ratings yet
- Basic Nursing PharmacologyDocument78 pagesBasic Nursing PharmacologyLloyd Rafael EstabilloNo ratings yet
- Mitral Valve Prolapse (MVP) : Auscultation of MurmursDocument55 pagesMitral Valve Prolapse (MVP) : Auscultation of MurmursYagyeshNo ratings yet
- Antihistamines: Author: Kimberly Mulcahy, Pharmd, Bcps Editor: Claudia Lee, RPH, MDDocument16 pagesAntihistamines: Author: Kimberly Mulcahy, Pharmd, Bcps Editor: Claudia Lee, RPH, MDHassan Ait YachouNo ratings yet
- Who MSD Mer 17.6 EngDocument656 pagesWho MSD Mer 17.6 Engnoto susantoNo ratings yet
- Diabetic Foot Pocketbook ColoplastDocument21 pagesDiabetic Foot Pocketbook ColoplastangienutterNo ratings yet
- 3 - Antidepressants DrugsDocument27 pages3 - Antidepressants DrugsHadeelNo ratings yet
- Mood Disorders StudentDocument32 pagesMood Disorders StudentRafly FernandaNo ratings yet
- Depression: SymptomsDocument12 pagesDepression: SymptomsSavio RebelloNo ratings yet
- Case Study No.4 The Telltale Heart: Group 2 Nuñez, Refuerzo, Abalos, Almonte, AlmueteDocument11 pagesCase Study No.4 The Telltale Heart: Group 2 Nuñez, Refuerzo, Abalos, Almonte, AlmueteRejeanne MonroyNo ratings yet
- Drug AbreviationDocument14 pagesDrug AbreviationGlenn Suerte100% (1)
- Determination of Packaging Efficiency of Norflu (Fluphenazine-Nortriptyline) in Case of Normal PackagingDocument74 pagesDetermination of Packaging Efficiency of Norflu (Fluphenazine-Nortriptyline) in Case of Normal PackagingRinta MoonNo ratings yet
- Jurnal DepresiDocument4 pagesJurnal DepresiBagus Ridho SetiadiNo ratings yet
- 800 Recalls With CorrectionDocument72 pages800 Recalls With CorrectionnancyNo ratings yet
- Pregabalin in Neurophatic Pain Related To DPN, Cancer and Back Pain Analysis of A 6 Week Observational StudyDocument11 pagesPregabalin in Neurophatic Pain Related To DPN, Cancer and Back Pain Analysis of A 6 Week Observational StudyadityaNo ratings yet
- Treating Panic Disorder: A Quick Reference GuideDocument23 pagesTreating Panic Disorder: A Quick Reference GuideAntónio MartinsNo ratings yet
- Psychiatric NursingDocument43 pagesPsychiatric NursingHaru100% (1)
- Drugs Affecting The Central Nervous SystemDocument22 pagesDrugs Affecting The Central Nervous Systemአብይ በላይነሽ ጥላሁንNo ratings yet
- Psychiatric MedicationsDocument1 pagePsychiatric MedicationspavanNo ratings yet
- Ibs JurnalDocument11 pagesIbs JurnalimuhammadfahmiNo ratings yet
- Atypical Antidepressants - Pharmacology, Administration, and Side Effects - UpToDateDocument16 pagesAtypical Antidepressants - Pharmacology, Administration, and Side Effects - UpToDateMelissandreNo ratings yet
- PhobiaDocument11 pagesPhobiaLegal Affairs OfficeNo ratings yet
- Psychiatry High Yield NotesDocument6 pagesPsychiatry High Yield Notesgregry2100% (3)



















































































































Download as pptx, pdf, or txt
You might also like
- Aa - LMR Georgette - Final VersionDocument47 pagesAa - LMR Georgette - Final Versionpickles.squad11No ratings yet
- PSYCH EOR EXAM QsDocument2 pagesPSYCH EOR EXAM Qskhalil bryant100% (1)
- Lab Monitoring For Psychiatric Medications: Reference TableDocument1 pageLab Monitoring For Psychiatric Medications: Reference TableTimothy Turscak100% (2)
- BTB Template Er-IntakeDocument3 pagesBTB Template Er-IntakeBoy MadNo ratings yet
- Second and Third Generation Antipsychotics: A Comprehensive HandbookFrom EverandSecond and Third Generation Antipsychotics: A Comprehensive HandbookRating: 5 out of 5 stars5/5 (1)
- Psychiatry HX TakingDocument4 pagesPsychiatry HX TakingP KasikrishnarajaNo ratings yet
- Psychotropic Medications During PregnancyDocument20 pagesPsychotropic Medications During PregnancyMaria Von ShaftNo ratings yet
- Psychopharmacologic Drugs: - Antipsychotic Agents - Antimanic Drugs - Antidepressant DrugsDocument18 pagesPsychopharmacologic Drugs: - Antipsychotic Agents - Antimanic Drugs - Antidepressant DrugsDrima EdiNo ratings yet
- Chronic Headache 2019 PDFDocument398 pagesChronic Headache 2019 PDFDaniel SisniegasNo ratings yet
- Laboratory Testing in PsychiatryDocument29 pagesLaboratory Testing in PsychiatrySera ChunNo ratings yet
- Antipsychotic DrugsDocument54 pagesAntipsychotic DrugsJackNo ratings yet
- PMHNP Case Study - EditedDocument7 pagesPMHNP Case Study - EditedSoumyadeep BoseNo ratings yet
- Laboratory Monitoring When Prescribing PsychotropicsDocument5 pagesLaboratory Monitoring When Prescribing PsychotropicswaleskacrzNo ratings yet
- Lab TestsDocument1 pageLab TestsnkivcNo ratings yet
- Shortened REM Latency and Increased REM: Previous AttemptDocument19 pagesShortened REM Latency and Increased REM: Previous AttemptActeen MyoseenNo ratings yet
- Final FY Presentation1Document45 pagesFinal FY Presentation1SamNo ratings yet
- The RX Files: QT Prolongation and Torsades de Pointes: Drugs and Sudden DeathDocument2 pagesThe RX Files: QT Prolongation and Torsades de Pointes: Drugs and Sudden DeathRahul RaiNo ratings yet
- Psychiatry Made EasyDocument14 pagesPsychiatry Made EasyD. W. S JayarathnaNo ratings yet
- 1: Adhd: Scientific Name Dose CommentsDocument4 pages1: Adhd: Scientific Name Dose CommentsSadiq Abdo92No ratings yet
- Varun Kumar, 2017 - Getting Started in PsychiatryDocument148 pagesVarun Kumar, 2017 - Getting Started in PsychiatryBernard FZ100% (1)
- AntipsychoticsDocument10 pagesAntipsychoticswawing16No ratings yet
- AnxietyDocument4 pagesAnxietyIT’S ME HAYLANo ratings yet
- Quick Reference Guide FallDocument62 pagesQuick Reference Guide FallKreshnik IdrizajNo ratings yet
- Antipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationDocument6 pagesAntipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationJaylord Verazon100% (1)
- Antidepressant Therapy AlgorithmDocument12 pagesAntidepressant Therapy AlgorithmZubair Mahmood KamalNo ratings yet
- HPI GuidelinesDocument5 pagesHPI GuidelinesHani NadiahNo ratings yet
- 504 - Pediatric Psychopharmacology - General PrinciplesDocument54 pages504 - Pediatric Psychopharmacology - General PrinciplesAlvaro HuidobroNo ratings yet
- Drugs For NeurolepticsDocument1 pageDrugs For Neurolepticssyamil_daudNo ratings yet
- Malingering NbiDocument5 pagesMalingering NbiPridina SyadirahNo ratings yet
- Risk Assessment Decision TreeDocument1 pageRisk Assessment Decision TreeHeather RamettaNo ratings yet
- Translate Kaplan Sadock Sinopsis Psikiatri Komprehensif Halaman 721 730 PDF FreeDocument76 pagesTranslate Kaplan Sadock Sinopsis Psikiatri Komprehensif Halaman 721 730 PDF FreeHadi GunaNo ratings yet
- B /G C U I R: Anti-PsychoticsDocument2 pagesB /G C U I R: Anti-PsychoticsErsy Sakti ilhamNo ratings yet
- Terms in The Field of Psychiatry and NeurologyDocument25 pagesTerms in The Field of Psychiatry and NeurologyMarlon SigfredNo ratings yet
- PsychopharmacologyDocument148 pagesPsychopharmacologyAsther Mantua100% (2)
- Pediatric Psychopharmacology: General PrinciplesDocument55 pagesPediatric Psychopharmacology: General PrinciplesAlvaro HuidobroNo ratings yet
- Psychotropic Drugs.Document15 pagesPsychotropic Drugs.Xiaoqing SongNo ratings yet
- Practical Notebook Adult PsychiatryDocument121 pagesPractical Notebook Adult PsychiatryCarly DyaNo ratings yet
- Structured Approach To Acute Psychiatry EmergenciesDocument41 pagesStructured Approach To Acute Psychiatry EmergenciesRaimondo RomanazziNo ratings yet
- Pharmacology - (5) Psychotic DrugsDocument8 pagesPharmacology - (5) Psychotic DrugsSamantha DiegoNo ratings yet
- Neuroleptic Advers ReactionDocument65 pagesNeuroleptic Advers Reactionayu yulianti100% (1)
- Antidepressant Use in Adults With Chronic Kidney DiseaseDocument1 pageAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- Pharmacological Management of DepressionDocument66 pagesPharmacological Management of DepressionPriyash JainNo ratings yet
- Psychiatric Interview (Autosaved)Document22 pagesPsychiatric Interview (Autosaved)Jana Victor100% (1)
- Psychiatric Visit1 - AaronVer3Document1 pagePsychiatric Visit1 - AaronVer3api-3764308No ratings yet
- Clozapine Care GuideDocument16 pagesClozapine Care GuideERWIN SUMARDINo ratings yet
- Psychiatry History & Suicide Risk Assessment TemplatesDocument32 pagesPsychiatry History & Suicide Risk Assessment TemplatesDuncan Jackson100% (2)
- MMP Handy Chart October 2011 V2Document69 pagesMMP Handy Chart October 2011 V2Icha IchaNo ratings yet
- SCTL NeurotransmitterDocument32 pagesSCTL Neurotransmitternur qistina humaira zulkarshamsiNo ratings yet
- Psychiatric Medications in Pregnancy and LactationDocument27 pagesPsychiatric Medications in Pregnancy and LactationSunija SelvamNo ratings yet
- The BrainDocument22 pagesThe BrainClae NapiNo ratings yet
- Handy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Document3 pagesHandy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Mariya ZhekovaNo ratings yet
- Week 2 (OSCE CASC Book II 2018-19) 03.09.2018Document48 pagesWeek 2 (OSCE CASC Book II 2018-19) 03.09.2018Andrew WdsmithNo ratings yet
- Psychiatry Notes Psychiatry Notes: Medicine (Queen Mary University of London) Medicine (Queen Mary University of London)Document28 pagesPsychiatry Notes Psychiatry Notes: Medicine (Queen Mary University of London) Medicine (Queen Mary University of London)Noman ButtNo ratings yet
- Study Guide Test 1Document11 pagesStudy Guide Test 1jwasylow13No ratings yet
- Psychiatry Grand NotesDocument10 pagesPsychiatry Grand NotesNathan T. CheungNo ratings yet
- BTB Template Er-IntakeDocument3 pagesBTB Template Er-IntakehectorNo ratings yet
- Adhd Toolkit MedicationsDocument1 pageAdhd Toolkit MedicationsreneezNo ratings yet
- Reviewer On PsychopharmacologyDocument28 pagesReviewer On PsychopharmacologyKristine Ann Hernandez100% (1)
- Long-Acting Injectable AntipsychoticsDocument18 pagesLong-Acting Injectable AntipsychoticsMia BlackattNo ratings yet
- Psychiatry Notes - Defenses MechanismsDocument2 pagesPsychiatry Notes - Defenses MechanismsLiSenNo ratings yet
- Mania: Carbamazepine, Valproic AcidDocument16 pagesMania: Carbamazepine, Valproic AcidKylie Elaine100% (1)
- Introduction To NeuropharmacologyDocument6 pagesIntroduction To Neuropharmacologyammarhafez78100% (1)
- Postpartum Psychiatric DisordersDocument55 pagesPostpartum Psychiatric DisordersAklile TsegaNo ratings yet
- Academic StressDocument5 pagesAcademic StressAklile TsegaNo ratings yet
- DeliriumDocument40 pagesDeliriumAklile TsegaNo ratings yet
- Quality of LifeDocument27 pagesQuality of LifeAklile TsegaNo ratings yet
- Nihms 446239Document9 pagesNihms 446239Aklile TsegaNo ratings yet
- Mubarek Aplied Neuroscience PPT Lecture NoteDocument50 pagesMubarek Aplied Neuroscience PPT Lecture NoteAklile TsegaNo ratings yet
- AssignmentDocument29 pagesAssignmentAklile TsegaNo ratings yet
- Psychiatric EmergencyDocument88 pagesPsychiatric EmergencyAklile TsegaNo ratings yet
- Country Focus Document Orange Knowledge ProgrammeDocument12 pagesCountry Focus Document Orange Knowledge ProgrammeAklile TsegaNo ratings yet
- Fpsyt 13 843984Document10 pagesFpsyt 13 843984Aklile TsegaNo ratings yet
- Higher Diploma Program A Centrally Initiated and Successfully Institutionalized Professional Development Program For Teachers in Ethiopian PublicDocument26 pagesHigher Diploma Program A Centrally Initiated and Successfully Institutionalized Professional Development Program For Teachers in Ethiopian PublicAklile TsegaNo ratings yet
- Almaz Mamaru Counseling Psychologist (BA, MA) Department of Psychiatry, Bahardar UniversityDocument39 pagesAlmaz Mamaru Counseling Psychologist (BA, MA) Department of Psychiatry, Bahardar UniversityAklile TsegaNo ratings yet
- NRR 328749 The Magnitude of Perceived Professionalism and Its AssociateDocument10 pagesNRR 328749 The Magnitude of Perceived Professionalism and Its AssociateAklile TsegaNo ratings yet
- Direct and Indirect Aggression in Intimate Relationships in Mexico and FinlandDocument1 pageDirect and Indirect Aggression in Intimate Relationships in Mexico and FinlandAklile TsegaNo ratings yet
- Conduct Disorder Diagnosis & TreatmentDocument13 pagesConduct Disorder Diagnosis & TreatmentAklile TsegaNo ratings yet
- Interpersonal Psychotherapy (IPT)Document39 pagesInterpersonal Psychotherapy (IPT)Aklile TsegaNo ratings yet
- Prevalence of Aggression, Antisocial Behaviors, and SuicideDocument18 pagesPrevalence of Aggression, Antisocial Behaviors, and SuicideAklile TsegaNo ratings yet
- Behavioral Therapies: Hailemariam Hailesilassie (Asst - Professor) Department of Psychiatry, FMS, JUDocument21 pagesBehavioral Therapies: Hailemariam Hailesilassie (Asst - Professor) Department of Psychiatry, FMS, JUAklile TsegaNo ratings yet
- Cognitive Behavior Therapy: Hailemariam Hailesilassie (Assist - Professor) Department of Psychiatry Jimma UniversityDocument109 pagesCognitive Behavior Therapy: Hailemariam Hailesilassie (Assist - Professor) Department of Psychiatry Jimma UniversityAklile TsegaNo ratings yet
- Eye Movement Desensitization Reprocessing Therapy (EMDR)Document48 pagesEye Movement Desensitization Reprocessing Therapy (EMDR)Aklile TsegaNo ratings yet
- Acceptance and Commitment Therapy (ACT)Document36 pagesAcceptance and Commitment Therapy (ACT)Aklile TsegaNo ratings yet
- Almaz Mamaru BA, MA (Counseling Psychology) Department of Psychiatry Collage of Medicine Health Science Bahardar UniversityDocument37 pagesAlmaz Mamaru BA, MA (Counseling Psychology) Department of Psychiatry Collage of Medicine Health Science Bahardar UniversityAklile TsegaNo ratings yet
- Bahirdar University College of Medicine and Health Science Department of Psychiatry Mood Disorder Assignment FEB 2020Document25 pagesBahirdar University College of Medicine and Health Science Department of Psychiatry Mood Disorder Assignment FEB 2020Aklile TsegaNo ratings yet
- Cognitive Behavioral Therapy Training in Core SkillsDocument65 pagesCognitive Behavioral Therapy Training in Core SkillsAklile TsegaNo ratings yet
- DoubleDocument25 pagesDoubleAklile TsegaNo ratings yet
- Nter-Ersonal HerapyDocument46 pagesNter-Ersonal HerapyAklile TsegaNo ratings yet
- Diversity Primer Chapter 04Document11 pagesDiversity Primer Chapter 04Aklile TsegaNo ratings yet
- Child and Adolescent Psychiatry AssignmentDocument3 pagesChild and Adolescent Psychiatry AssignmentAklile TsegaNo ratings yet
- Pharmacology Related To Psychiatric NursingDocument7 pagesPharmacology Related To Psychiatric NursingGlenn Daryll SantosNo ratings yet
- MCQS Dr. Aalia New 31 October 2008Document4 pagesMCQS Dr. Aalia New 31 October 2008rawalianNo ratings yet
- DigoxinDocument6 pagesDigoxinSEIYADU IBRAHIM KNo ratings yet
- Adult ADHD - What Do When Your First Drug Fails - Dr.-James-LazowskiDocument77 pagesAdult ADHD - What Do When Your First Drug Fails - Dr.-James-LazowskiJason WongNo ratings yet
- Falls in Older Persons - Risk Factors and Patient Evaluation - UpToDateDocument24 pagesFalls in Older Persons - Risk Factors and Patient Evaluation - UpToDateNhungVũNo ratings yet
- Basic Nursing PharmacologyDocument78 pagesBasic Nursing PharmacologyLloyd Rafael EstabilloNo ratings yet
- Mitral Valve Prolapse (MVP) : Auscultation of MurmursDocument55 pagesMitral Valve Prolapse (MVP) : Auscultation of MurmursYagyeshNo ratings yet
- Antihistamines: Author: Kimberly Mulcahy, Pharmd, Bcps Editor: Claudia Lee, RPH, MDDocument16 pagesAntihistamines: Author: Kimberly Mulcahy, Pharmd, Bcps Editor: Claudia Lee, RPH, MDHassan Ait YachouNo ratings yet
- Who MSD Mer 17.6 EngDocument656 pagesWho MSD Mer 17.6 Engnoto susantoNo ratings yet
- Diabetic Foot Pocketbook ColoplastDocument21 pagesDiabetic Foot Pocketbook ColoplastangienutterNo ratings yet
- 3 - Antidepressants DrugsDocument27 pages3 - Antidepressants DrugsHadeelNo ratings yet
- Mood Disorders StudentDocument32 pagesMood Disorders StudentRafly FernandaNo ratings yet
- Depression: SymptomsDocument12 pagesDepression: SymptomsSavio RebelloNo ratings yet
- Case Study No.4 The Telltale Heart: Group 2 Nuñez, Refuerzo, Abalos, Almonte, AlmueteDocument11 pagesCase Study No.4 The Telltale Heart: Group 2 Nuñez, Refuerzo, Abalos, Almonte, AlmueteRejeanne MonroyNo ratings yet
- Drug AbreviationDocument14 pagesDrug AbreviationGlenn Suerte100% (1)
- Determination of Packaging Efficiency of Norflu (Fluphenazine-Nortriptyline) in Case of Normal PackagingDocument74 pagesDetermination of Packaging Efficiency of Norflu (Fluphenazine-Nortriptyline) in Case of Normal PackagingRinta MoonNo ratings yet
- Jurnal DepresiDocument4 pagesJurnal DepresiBagus Ridho SetiadiNo ratings yet
- 800 Recalls With CorrectionDocument72 pages800 Recalls With CorrectionnancyNo ratings yet
- Pregabalin in Neurophatic Pain Related To DPN, Cancer and Back Pain Analysis of A 6 Week Observational StudyDocument11 pagesPregabalin in Neurophatic Pain Related To DPN, Cancer and Back Pain Analysis of A 6 Week Observational StudyadityaNo ratings yet
- Treating Panic Disorder: A Quick Reference GuideDocument23 pagesTreating Panic Disorder: A Quick Reference GuideAntónio MartinsNo ratings yet
- Psychiatric NursingDocument43 pagesPsychiatric NursingHaru100% (1)
- Drugs Affecting The Central Nervous SystemDocument22 pagesDrugs Affecting The Central Nervous Systemአብይ በላይነሽ ጥላሁንNo ratings yet
- Psychiatric MedicationsDocument1 pagePsychiatric MedicationspavanNo ratings yet
- Ibs JurnalDocument11 pagesIbs JurnalimuhammadfahmiNo ratings yet
- Atypical Antidepressants - Pharmacology, Administration, and Side Effects - UpToDateDocument16 pagesAtypical Antidepressants - Pharmacology, Administration, and Side Effects - UpToDateMelissandreNo ratings yet
- PhobiaDocument11 pagesPhobiaLegal Affairs OfficeNo ratings yet
- Psychiatry High Yield NotesDocument6 pagesPsychiatry High Yield Notesgregry2100% (3)