
2 SUPPOSITORIES&PESSARIEs 1 1
2 SUPPOSITORIES&PESSARIEs 1 1
You might also like
- To Perforasi GasterDocument27 pagesTo Perforasi GasterPuthu BelegugNo ratings yet
- Lecturenote - 445494777p'cal SUPPOSITORIES&PESSARIEsDocument80 pagesLecturenote - 445494777p'cal SUPPOSITORIES&PESSARIEsAsnakeNo ratings yet
- Lecture 5 (Suppositories Part 1)Document17 pagesLecture 5 (Suppositories Part 1)mheni4979No ratings yet
- Suppositiry HandoutDocument31 pagesSuppositiry HandoutTesfaye GabrielNo ratings yet
- Suppositories IUB NSDocument44 pagesSuppositories IUB NSNowfal Hasan SiamNo ratings yet
- Suppositories and EnemasDocument35 pagesSuppositories and EnemasMr.ShazNo ratings yet
- Drug Ders 3Document27 pagesDrug Ders 3nadyamelekavciNo ratings yet
- Suppositories and PessariesDocument61 pagesSuppositories and PessariesAbera JamboNo ratings yet
- SuppositoriesDocument12 pagesSuppositoriesJAKE BENZYN TENo ratings yet
- IPPP-II (Supp)Document85 pagesIPPP-II (Supp)Tinsaye HayileNo ratings yet
- ADME & Principle of Drug ActionDocument103 pagesADME & Principle of Drug ActionInshaNo ratings yet
- Study Guide 1 Assessment of Digestive and Gastrointestinal Function and Treatment ModalitiesDocument10 pagesStudy Guide 1 Assessment of Digestive and Gastrointestinal Function and Treatment ModalitiesKc Cabanilla LizardoNo ratings yet
- Anatomic and Physiological Consideration in Oral Drug AbsorptionDocument34 pagesAnatomic and Physiological Consideration in Oral Drug AbsorptionTataNo ratings yet
- Anatomic and Physiological Consideration in Oral Drug AbsorptionDocument34 pagesAnatomic and Physiological Consideration in Oral Drug AbsorptionLina WinartiNo ratings yet
- PHMD 444 - GIT Pharmacology - Prof Banga - FinalDocument88 pagesPHMD 444 - GIT Pharmacology - Prof Banga - FinalJEPHTHAH KWASI DANSONo ratings yet
- Physiological Factors Affecting Drug AbsorptionDocument6 pagesPhysiological Factors Affecting Drug AbsorptionMuhammad AbbasNo ratings yet
- ANATOMICAL AND PHYSIOLOGICAL Factors Affecting DRUG ABSORPTIONDocument8 pagesANATOMICAL AND PHYSIOLOGICAL Factors Affecting DRUG ABSORPTIONMuhammad AbbasNo ratings yet
- Dyspepsia and Homeopathic TreatmentDocument62 pagesDyspepsia and Homeopathic Treatmentdrmsupriya100% (1)
- GIDocument7 pagesGIiheart musicNo ratings yet
- Grdds ReviewDocument33 pagesGrdds ReviewvaibhavbpatelNo ratings yet
- Pharmacology Transes - Unit 1Document13 pagesPharmacology Transes - Unit 1venturaphoenixNo ratings yet
- GROUP 1 - Digestive SystemDocument76 pagesGROUP 1 - Digestive SystemMa. Therese CampoNo ratings yet
- Major Organs of Digestion and AbsorptionDocument104 pagesMajor Organs of Digestion and Absorptionalyssa1230100% (2)
- Gastro Retentive Drug Delivery System: Presented By: Dr. M. Waqas IlyasDocument25 pagesGastro Retentive Drug Delivery System: Presented By: Dr. M. Waqas IlyasQA Dhq OkaraNo ratings yet
- ConstipationDocument30 pagesConstipationBareera NudratNo ratings yet
- Lesson 1. Let's Engage Types of Enemas PurposesDocument4 pagesLesson 1. Let's Engage Types of Enemas PurposesJewel BerbanoNo ratings yet
- Phases of Drug Action: Pharmaceutic Pharmacokinetic PharmacodynamicDocument153 pagesPhases of Drug Action: Pharmaceutic Pharmacokinetic PharmacodynamicNicole NipasNo ratings yet
- Intestinal ObstructionDocument16 pagesIntestinal ObstructionPdianghunNo ratings yet
- Plenary 5B Group 13Document163 pagesPlenary 5B Group 13Obet Agung 天No ratings yet
- Alterations in Nutrition and GastrointestinalDocument7 pagesAlterations in Nutrition and GastrointestinalChriszanie CruzNo ratings yet
- Course Topic Cu11 DigestionDocument14 pagesCourse Topic Cu11 DigestionMichelle MallareNo ratings yet
- Digestive System Anatomy and Physiology - NurseslabsDocument33 pagesDigestive System Anatomy and Physiology - NurseslabsMari FeNo ratings yet
- Drug Delivery On Rectal Absorption: Suppositories: Review ArticleDocument7 pagesDrug Delivery On Rectal Absorption: Suppositories: Review ArticleNindah IkaNo ratings yet
- 12 Tra - Gastrointestinall SystemDocument20 pages12 Tra - Gastrointestinall SystemJoshua DelantarNo ratings yet
- NCM 116 W1 Reading HandoutDocument13 pagesNCM 116 W1 Reading Handoutriza sarmientoNo ratings yet
- Unit 6 Targeted Drug DeliveryDocument42 pagesUnit 6 Targeted Drug Deliveryabdullah2020100% (1)
- Ryles - Jejunostomy Tube FeedingDocument12 pagesRyles - Jejunostomy Tube FeedingM senNo ratings yet
- Learning Objectives:: at The End of This Lecture, You Will Be Able ToDocument119 pagesLearning Objectives:: at The End of This Lecture, You Will Be Able ToMaica LectanaNo ratings yet
- Lecture 2, Introduction To Pharmacology Continued. (Script)Document11 pagesLecture 2, Introduction To Pharmacology Continued. (Script)JustDen0950% (2)
- GRDDSDocument31 pagesGRDDSMuhammad Azam TahirNo ratings yet
- Raft Forming System - Gastroretentive Drug Delivery SystemDocument5 pagesRaft Forming System - Gastroretentive Drug Delivery SystemIjaems JournalNo ratings yet
- Case Presentation (NCM 102)Document26 pagesCase Presentation (NCM 102)Ibs LimNo ratings yet
- Human Body Digestive SystemDocument6 pagesHuman Body Digestive SystemMaria SibauNo ratings yet
- Week1 UgitDocument119 pagesWeek1 UgitriverabeanicoNo ratings yet
- ContentsDocument35 pagesContentsMukesh GamiNo ratings yet
- Advantages and Disadvantages of Rectal Dosage FormsDocument4 pagesAdvantages and Disadvantages of Rectal Dosage FormsNurawaliaNo ratings yet
- Nursing Pharmacology 2023Document355 pagesNursing Pharmacology 2023jaizamaeenriquez59No ratings yet
- GRDDS and EvaluationDocument54 pagesGRDDS and Evaluationgayatri maldhureNo ratings yet
- Pharmacology of Gastrointestinal SystemDocument4 pagesPharmacology of Gastrointestinal SystemZaira KimNo ratings yet
- AppendicitisDocument6 pagesAppendicitisNathalie L. RaquelNo ratings yet
- Gastroretentive Drug Delivery SystemDocument33 pagesGastroretentive Drug Delivery SystemSaid Muhammad WazirNo ratings yet
- NCM116 Prelim Week 1Document15 pagesNCM116 Prelim Week 1Loungayvan BatuyogNo ratings yet
- 16 Digestive SystemDocument4 pages16 Digestive SystemOribello, Athenna Jae W.No ratings yet
- GRDDS 2021Document94 pagesGRDDS 2021Shubh AgarwalNo ratings yet
- Anatomy & Physiology - October 2-4Document15 pagesAnatomy & Physiology - October 2-4Ayessa Camelle DumileNo ratings yet
- Suppository Definitions: Rectum Vagina Urethra Medicine Pharmaceutical PessaryDocument5 pagesSuppository Definitions: Rectum Vagina Urethra Medicine Pharmaceutical PessarySugar CabelNo ratings yet
- Drug Administration With BlanksDocument15 pagesDrug Administration With BlanksJONALYN REGACHONo ratings yet
- Hirschprung DiseaseDocument61 pagesHirschprung DiseaseAdditi Satyal100% (1)
- Gastrointestinalsystem 160329122856Document77 pagesGastrointestinalsystem 160329122856Putti AnnisaNo ratings yet
- Force and WindTunnel BalanceDocument19 pagesForce and WindTunnel BalanceTHE BOISNo ratings yet
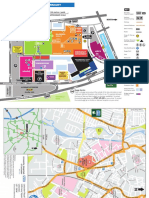
- Leicester Royal Infirmary: M1 M69 Football Stadium KEYDocument2 pagesLeicester Royal Infirmary: M1 M69 Football Stadium KEYpdhoppyNo ratings yet
- A Study Financial Behavior: Bottlers Nepal Limited Dabur Nepal LimitedDocument10 pagesA Study Financial Behavior: Bottlers Nepal Limited Dabur Nepal LimitedAarju PoudelNo ratings yet
- CIBIL Consent FormDocument4 pagesCIBIL Consent FormKuldeep BatraNo ratings yet
- LTE Performance and Optimization ConsultantDocument6 pagesLTE Performance and Optimization ConsultantmalikmdnuraniNo ratings yet
- Universiti Teknologi Mara: Analytical Chemistry (Chm421) AS/TEST 3/JUNE 2020Document2 pagesUniversiti Teknologi Mara: Analytical Chemistry (Chm421) AS/TEST 3/JUNE 2020Erna HamidNo ratings yet
- What Is Bacteria - What Are BacteriaDocument15 pagesWhat Is Bacteria - What Are BacteriaFernando OssNo ratings yet
- FTII Acting Entance EXAM Notes - JET 2019Document61 pagesFTII Acting Entance EXAM Notes - JET 2019Vipul ShankarNo ratings yet
- Smart Inverters: Ul 1741 Sa and Advanced Inverter Testing: Haiwen (Howard) Liu, PH.DDocument19 pagesSmart Inverters: Ul 1741 Sa and Advanced Inverter Testing: Haiwen (Howard) Liu, PH.DZennia VillanuevaNo ratings yet
- Struktol RP 17 MSDS PDFDocument7 pagesStruktol RP 17 MSDS PDFSimonNo ratings yet
- Designing and Implementing A Datawarehousing (Step1) : Chapter-4Document8 pagesDesigning and Implementing A Datawarehousing (Step1) : Chapter-4Mohamoud Farah Abdilahi AliNo ratings yet
- The Coinage of The Mamlūk Sultan Baybars I: Additions and Corrections / Michael L. BatesDocument25 pagesThe Coinage of The Mamlūk Sultan Baybars I: Additions and Corrections / Michael L. BatesDigital Library Numis (DLN)No ratings yet
- Co2 04Document16 pagesCo2 04Poojitha BondalapatiNo ratings yet
- FSI-000020509 - Packing List 20315Document1 pageFSI-000020509 - Packing List 20315Mangesh KadamNo ratings yet
- Mémoire AI For The Recognition and Classification of Catastrophic ScenariosDocument116 pagesMémoire AI For The Recognition and Classification of Catastrophic ScenariosMohamed TekoukNo ratings yet
- Unit-2: Linear Data Structure StackDocument37 pagesUnit-2: Linear Data Structure StackDivyes P100% (1)
- Api 575Document37 pagesApi 575Sakthi Pk100% (3)
- Rototherm Group Product Catalogue 2016Document40 pagesRototherm Group Product Catalogue 2016Charles OnyechereNo ratings yet
- 10 Total Mark: 10 X 1 10: NPTEL Online Certification Courses Indian Institute of Technology KharagpurDocument6 pages10 Total Mark: 10 X 1 10: NPTEL Online Certification Courses Indian Institute of Technology KharagpurvitNo ratings yet
- Opengl Es Common/Common-Lite Profile Specification: Version 1.1.12 (Difference Specification) (Annotated)Document128 pagesOpengl Es Common/Common-Lite Profile Specification: Version 1.1.12 (Difference Specification) (Annotated)bitNo ratings yet
- LP 1 Music Q3Document4 pagesLP 1 Music Q3Hazel Rubas SamsonNo ratings yet
- 6023 - STD - Digital Gauges - EDocument16 pages6023 - STD - Digital Gauges - EJános KovácsNo ratings yet
- HT Turorial Question BankDocument16 pagesHT Turorial Question BankA. AnsarNo ratings yet
- Experiment 6 Kirchhoff and PowerDocument13 pagesExperiment 6 Kirchhoff and PowerVenus IlaganNo ratings yet
- Nitesh CVDocument2 pagesNitesh CVpatil.nitesh9211No ratings yet
- Unit 4 NotesDocument45 pagesUnit 4 Notesvamsi kiran100% (1)
- Discussion Assignment Unit 1 EDUC 5240-01Document5 pagesDiscussion Assignment Unit 1 EDUC 5240-01Javier ToyNo ratings yet
- Apti 4,5Document66 pagesApti 4,5727822TPMB139 SIVAPRIYA.MNo ratings yet
- Airway PositioningDocument34 pagesAirway PositioningAsep PurnomosidiNo ratings yet
- Food Industry JFCDocument31 pagesFood Industry JFCJheanniver Nablo-PeñaNo ratings yet
























































































Download as pptx, pdf, or txt
You might also like
- To Perforasi GasterDocument27 pagesTo Perforasi GasterPuthu BelegugNo ratings yet
- Lecturenote - 445494777p'cal SUPPOSITORIES&PESSARIEsDocument80 pagesLecturenote - 445494777p'cal SUPPOSITORIES&PESSARIEsAsnakeNo ratings yet
- Lecture 5 (Suppositories Part 1)Document17 pagesLecture 5 (Suppositories Part 1)mheni4979No ratings yet
- Suppositiry HandoutDocument31 pagesSuppositiry HandoutTesfaye GabrielNo ratings yet
- Suppositories IUB NSDocument44 pagesSuppositories IUB NSNowfal Hasan SiamNo ratings yet
- Suppositories and EnemasDocument35 pagesSuppositories and EnemasMr.ShazNo ratings yet
- Drug Ders 3Document27 pagesDrug Ders 3nadyamelekavciNo ratings yet
- Suppositories and PessariesDocument61 pagesSuppositories and PessariesAbera JamboNo ratings yet
- SuppositoriesDocument12 pagesSuppositoriesJAKE BENZYN TENo ratings yet
- IPPP-II (Supp)Document85 pagesIPPP-II (Supp)Tinsaye HayileNo ratings yet
- ADME & Principle of Drug ActionDocument103 pagesADME & Principle of Drug ActionInshaNo ratings yet
- Study Guide 1 Assessment of Digestive and Gastrointestinal Function and Treatment ModalitiesDocument10 pagesStudy Guide 1 Assessment of Digestive and Gastrointestinal Function and Treatment ModalitiesKc Cabanilla LizardoNo ratings yet
- Anatomic and Physiological Consideration in Oral Drug AbsorptionDocument34 pagesAnatomic and Physiological Consideration in Oral Drug AbsorptionTataNo ratings yet
- Anatomic and Physiological Consideration in Oral Drug AbsorptionDocument34 pagesAnatomic and Physiological Consideration in Oral Drug AbsorptionLina WinartiNo ratings yet
- PHMD 444 - GIT Pharmacology - Prof Banga - FinalDocument88 pagesPHMD 444 - GIT Pharmacology - Prof Banga - FinalJEPHTHAH KWASI DANSONo ratings yet
- Physiological Factors Affecting Drug AbsorptionDocument6 pagesPhysiological Factors Affecting Drug AbsorptionMuhammad AbbasNo ratings yet
- ANATOMICAL AND PHYSIOLOGICAL Factors Affecting DRUG ABSORPTIONDocument8 pagesANATOMICAL AND PHYSIOLOGICAL Factors Affecting DRUG ABSORPTIONMuhammad AbbasNo ratings yet
- Dyspepsia and Homeopathic TreatmentDocument62 pagesDyspepsia and Homeopathic Treatmentdrmsupriya100% (1)
- GIDocument7 pagesGIiheart musicNo ratings yet
- Grdds ReviewDocument33 pagesGrdds ReviewvaibhavbpatelNo ratings yet
- Pharmacology Transes - Unit 1Document13 pagesPharmacology Transes - Unit 1venturaphoenixNo ratings yet
- GROUP 1 - Digestive SystemDocument76 pagesGROUP 1 - Digestive SystemMa. Therese CampoNo ratings yet
- Major Organs of Digestion and AbsorptionDocument104 pagesMajor Organs of Digestion and Absorptionalyssa1230100% (2)
- Gastro Retentive Drug Delivery System: Presented By: Dr. M. Waqas IlyasDocument25 pagesGastro Retentive Drug Delivery System: Presented By: Dr. M. Waqas IlyasQA Dhq OkaraNo ratings yet
- ConstipationDocument30 pagesConstipationBareera NudratNo ratings yet
- Lesson 1. Let's Engage Types of Enemas PurposesDocument4 pagesLesson 1. Let's Engage Types of Enemas PurposesJewel BerbanoNo ratings yet
- Phases of Drug Action: Pharmaceutic Pharmacokinetic PharmacodynamicDocument153 pagesPhases of Drug Action: Pharmaceutic Pharmacokinetic PharmacodynamicNicole NipasNo ratings yet
- Intestinal ObstructionDocument16 pagesIntestinal ObstructionPdianghunNo ratings yet
- Plenary 5B Group 13Document163 pagesPlenary 5B Group 13Obet Agung 天No ratings yet
- Alterations in Nutrition and GastrointestinalDocument7 pagesAlterations in Nutrition and GastrointestinalChriszanie CruzNo ratings yet
- Course Topic Cu11 DigestionDocument14 pagesCourse Topic Cu11 DigestionMichelle MallareNo ratings yet
- Digestive System Anatomy and Physiology - NurseslabsDocument33 pagesDigestive System Anatomy and Physiology - NurseslabsMari FeNo ratings yet
- Drug Delivery On Rectal Absorption: Suppositories: Review ArticleDocument7 pagesDrug Delivery On Rectal Absorption: Suppositories: Review ArticleNindah IkaNo ratings yet
- 12 Tra - Gastrointestinall SystemDocument20 pages12 Tra - Gastrointestinall SystemJoshua DelantarNo ratings yet
- NCM 116 W1 Reading HandoutDocument13 pagesNCM 116 W1 Reading Handoutriza sarmientoNo ratings yet
- Unit 6 Targeted Drug DeliveryDocument42 pagesUnit 6 Targeted Drug Deliveryabdullah2020100% (1)
- Ryles - Jejunostomy Tube FeedingDocument12 pagesRyles - Jejunostomy Tube FeedingM senNo ratings yet
- Learning Objectives:: at The End of This Lecture, You Will Be Able ToDocument119 pagesLearning Objectives:: at The End of This Lecture, You Will Be Able ToMaica LectanaNo ratings yet
- Lecture 2, Introduction To Pharmacology Continued. (Script)Document11 pagesLecture 2, Introduction To Pharmacology Continued. (Script)JustDen0950% (2)
- GRDDSDocument31 pagesGRDDSMuhammad Azam TahirNo ratings yet
- Raft Forming System - Gastroretentive Drug Delivery SystemDocument5 pagesRaft Forming System - Gastroretentive Drug Delivery SystemIjaems JournalNo ratings yet
- Case Presentation (NCM 102)Document26 pagesCase Presentation (NCM 102)Ibs LimNo ratings yet
- Human Body Digestive SystemDocument6 pagesHuman Body Digestive SystemMaria SibauNo ratings yet
- Week1 UgitDocument119 pagesWeek1 UgitriverabeanicoNo ratings yet
- ContentsDocument35 pagesContentsMukesh GamiNo ratings yet
- Advantages and Disadvantages of Rectal Dosage FormsDocument4 pagesAdvantages and Disadvantages of Rectal Dosage FormsNurawaliaNo ratings yet
- Nursing Pharmacology 2023Document355 pagesNursing Pharmacology 2023jaizamaeenriquez59No ratings yet
- GRDDS and EvaluationDocument54 pagesGRDDS and Evaluationgayatri maldhureNo ratings yet
- Pharmacology of Gastrointestinal SystemDocument4 pagesPharmacology of Gastrointestinal SystemZaira KimNo ratings yet
- AppendicitisDocument6 pagesAppendicitisNathalie L. RaquelNo ratings yet
- Gastroretentive Drug Delivery SystemDocument33 pagesGastroretentive Drug Delivery SystemSaid Muhammad WazirNo ratings yet
- NCM116 Prelim Week 1Document15 pagesNCM116 Prelim Week 1Loungayvan BatuyogNo ratings yet
- 16 Digestive SystemDocument4 pages16 Digestive SystemOribello, Athenna Jae W.No ratings yet
- GRDDS 2021Document94 pagesGRDDS 2021Shubh AgarwalNo ratings yet
- Anatomy & Physiology - October 2-4Document15 pagesAnatomy & Physiology - October 2-4Ayessa Camelle DumileNo ratings yet
- Suppository Definitions: Rectum Vagina Urethra Medicine Pharmaceutical PessaryDocument5 pagesSuppository Definitions: Rectum Vagina Urethra Medicine Pharmaceutical PessarySugar CabelNo ratings yet
- Drug Administration With BlanksDocument15 pagesDrug Administration With BlanksJONALYN REGACHONo ratings yet
- Hirschprung DiseaseDocument61 pagesHirschprung DiseaseAdditi Satyal100% (1)
- Gastrointestinalsystem 160329122856Document77 pagesGastrointestinalsystem 160329122856Putti AnnisaNo ratings yet
- Force and WindTunnel BalanceDocument19 pagesForce and WindTunnel BalanceTHE BOISNo ratings yet
- Leicester Royal Infirmary: M1 M69 Football Stadium KEYDocument2 pagesLeicester Royal Infirmary: M1 M69 Football Stadium KEYpdhoppyNo ratings yet
- A Study Financial Behavior: Bottlers Nepal Limited Dabur Nepal LimitedDocument10 pagesA Study Financial Behavior: Bottlers Nepal Limited Dabur Nepal LimitedAarju PoudelNo ratings yet
- CIBIL Consent FormDocument4 pagesCIBIL Consent FormKuldeep BatraNo ratings yet
- LTE Performance and Optimization ConsultantDocument6 pagesLTE Performance and Optimization ConsultantmalikmdnuraniNo ratings yet
- Universiti Teknologi Mara: Analytical Chemistry (Chm421) AS/TEST 3/JUNE 2020Document2 pagesUniversiti Teknologi Mara: Analytical Chemistry (Chm421) AS/TEST 3/JUNE 2020Erna HamidNo ratings yet
- What Is Bacteria - What Are BacteriaDocument15 pagesWhat Is Bacteria - What Are BacteriaFernando OssNo ratings yet
- FTII Acting Entance EXAM Notes - JET 2019Document61 pagesFTII Acting Entance EXAM Notes - JET 2019Vipul ShankarNo ratings yet
- Smart Inverters: Ul 1741 Sa and Advanced Inverter Testing: Haiwen (Howard) Liu, PH.DDocument19 pagesSmart Inverters: Ul 1741 Sa and Advanced Inverter Testing: Haiwen (Howard) Liu, PH.DZennia VillanuevaNo ratings yet
- Struktol RP 17 MSDS PDFDocument7 pagesStruktol RP 17 MSDS PDFSimonNo ratings yet
- Designing and Implementing A Datawarehousing (Step1) : Chapter-4Document8 pagesDesigning and Implementing A Datawarehousing (Step1) : Chapter-4Mohamoud Farah Abdilahi AliNo ratings yet
- The Coinage of The Mamlūk Sultan Baybars I: Additions and Corrections / Michael L. BatesDocument25 pagesThe Coinage of The Mamlūk Sultan Baybars I: Additions and Corrections / Michael L. BatesDigital Library Numis (DLN)No ratings yet
- Co2 04Document16 pagesCo2 04Poojitha BondalapatiNo ratings yet
- FSI-000020509 - Packing List 20315Document1 pageFSI-000020509 - Packing List 20315Mangesh KadamNo ratings yet
- Mémoire AI For The Recognition and Classification of Catastrophic ScenariosDocument116 pagesMémoire AI For The Recognition and Classification of Catastrophic ScenariosMohamed TekoukNo ratings yet
- Unit-2: Linear Data Structure StackDocument37 pagesUnit-2: Linear Data Structure StackDivyes P100% (1)
- Api 575Document37 pagesApi 575Sakthi Pk100% (3)
- Rototherm Group Product Catalogue 2016Document40 pagesRototherm Group Product Catalogue 2016Charles OnyechereNo ratings yet
- 10 Total Mark: 10 X 1 10: NPTEL Online Certification Courses Indian Institute of Technology KharagpurDocument6 pages10 Total Mark: 10 X 1 10: NPTEL Online Certification Courses Indian Institute of Technology KharagpurvitNo ratings yet
- Opengl Es Common/Common-Lite Profile Specification: Version 1.1.12 (Difference Specification) (Annotated)Document128 pagesOpengl Es Common/Common-Lite Profile Specification: Version 1.1.12 (Difference Specification) (Annotated)bitNo ratings yet
- LP 1 Music Q3Document4 pagesLP 1 Music Q3Hazel Rubas SamsonNo ratings yet
- 6023 - STD - Digital Gauges - EDocument16 pages6023 - STD - Digital Gauges - EJános KovácsNo ratings yet
- HT Turorial Question BankDocument16 pagesHT Turorial Question BankA. AnsarNo ratings yet
- Experiment 6 Kirchhoff and PowerDocument13 pagesExperiment 6 Kirchhoff and PowerVenus IlaganNo ratings yet
- Nitesh CVDocument2 pagesNitesh CVpatil.nitesh9211No ratings yet
- Unit 4 NotesDocument45 pagesUnit 4 Notesvamsi kiran100% (1)
- Discussion Assignment Unit 1 EDUC 5240-01Document5 pagesDiscussion Assignment Unit 1 EDUC 5240-01Javier ToyNo ratings yet
- Apti 4,5Document66 pagesApti 4,5727822TPMB139 SIVAPRIYA.MNo ratings yet
- Airway PositioningDocument34 pagesAirway PositioningAsep PurnomosidiNo ratings yet
- Food Industry JFCDocument31 pagesFood Industry JFCJheanniver Nablo-PeñaNo ratings yet