Download as pptx, pdf, or txt
You might also like
- Gender Identity DisorderDocument2 pagesGender Identity DisorderAngelaTrinidadNo ratings yet
- Case Study 416Document8 pagesCase Study 416wbmark67% (6)
- Health Promotion For ElderlyDocument37 pagesHealth Promotion For ElderlyAmr IbrahimNo ratings yet
- 2/25/22 Medical Surgical Nursing-Ii 1Document13 pages2/25/22 Medical Surgical Nursing-Ii 1Salman KhanNo ratings yet
- NCM 114 Physiologic Changes HandoutsDocument31 pagesNCM 114 Physiologic Changes HandoutsHeavenNo ratings yet
- Elderly 170825043248Document46 pagesElderly 170825043248enam professorNo ratings yet
- Mental Health and Psychiatric AssessmentDocument182 pagesMental Health and Psychiatric AssessmentJanine Mae MacaraigNo ratings yet
- Understanding Low Blood Pressure - The BasicsDocument6 pagesUnderstanding Low Blood Pressure - The BasicsRajeev Nechiyil100% (1)
- GOITERDocument4 pagesGOITERJerika Shane MañosoNo ratings yet
- Kaposis SarcomaDocument15 pagesKaposis SarcomaAlvic Dy KowNo ratings yet
- Anatomy of The KidneysDocument7 pagesAnatomy of The KidneysSanthu SuNo ratings yet
- AnemiaDocument71 pagesAnemiaAnsu MaliyakalNo ratings yet
- CholeraDocument4 pagesCholeraBeth AvelinoNo ratings yet
- PancreatitisDocument12 pagesPancreatitismardsz100% (5)
- Infections of The Urinary TractDocument41 pagesInfections of The Urinary TractGiri DharanNo ratings yet
- Pathophysiology Tia VS CvaDocument6 pagesPathophysiology Tia VS CvaRobby Nur Zam ZamNo ratings yet
- Tension Headaches: What Is A Tension Headache? HighlightsDocument9 pagesTension Headaches: What Is A Tension Headache? HighlightsIndryNo ratings yet
- Geriatric Giants Iwal 1 2020Document58 pagesGeriatric Giants Iwal 1 2020selymariaNo ratings yet
- Alcohol Dependance SyndromeDocument25 pagesAlcohol Dependance SyndromeRex RobbyNo ratings yet
- AnaemiaDocument40 pagesAnaemiaNaveen Kumar100% (1)
- Lesson Plan On Age-Related-Geriatrics-ProblemDocument11 pagesLesson Plan On Age-Related-Geriatrics-Problemmohamad dildarNo ratings yet
- Depression PP FVDocument62 pagesDepression PP FVSharmela Brijmohan100% (1)
- Normocytic Anemia'sDocument14 pagesNormocytic Anemia'sbrown_chocolate87643No ratings yet
- Health AssessmentsDocument76 pagesHealth AssessmentsAtashia Rain GaguiNo ratings yet
- 8nutritional AssessmentDocument59 pages8nutritional AssessmentMikki lor PuaganNo ratings yet
- Adrenal Hormone 2018 PDFDocument66 pagesAdrenal Hormone 2018 PDFrosyidafiaNo ratings yet
- Physiologic Changes in ElderlyDocument6 pagesPhysiologic Changes in ElderlyAngelie PantajoNo ratings yet
- 20-Chronic Kidney FailureDocument16 pages20-Chronic Kidney Failureمصطفى محمد جواد كاظمNo ratings yet
- Identification and Diagnosis: Compulsive Alcoholic BeveragesDocument3 pagesIdentification and Diagnosis: Compulsive Alcoholic BeveragesKaren JulaoNo ratings yet
- IV Infusion: Purpose of Starting IV'sDocument6 pagesIV Infusion: Purpose of Starting IV'sKiara Denise TamayoNo ratings yet
- Fluid Electrolyte Imbalance n132 160210135651Document100 pagesFluid Electrolyte Imbalance n132 160210135651Shahan FarooqNo ratings yet
- Diabetes Insipidus, Siadh and Cerebral Salt-WastingDocument33 pagesDiabetes Insipidus, Siadh and Cerebral Salt-WastingEuphrasiaNo ratings yet
- Neurological Manifestations of HIVDocument34 pagesNeurological Manifestations of HIVashuNo ratings yet
- Geron NclexDocument53 pagesGeron NclexGodfrey FrancoNo ratings yet
- CholeraDocument5 pagesCholerabishnu011978No ratings yet
- TBI FinalDocument28 pagesTBI Finalawais mpNo ratings yet
- Diabetes ComplicationsDocument29 pagesDiabetes ComplicationsTom ThomasNo ratings yet
- Surgical Management:: Nursing CareDocument3 pagesSurgical Management:: Nursing CareVarsha Net CafeNo ratings yet
- Hyporeninemic HypoaldosteronismDocument12 pagesHyporeninemic HypoaldosteronismCésar Augusto Sánchez SolisNo ratings yet
- UrolithiasisDocument29 pagesUrolithiasis143bb100% (1)
- CKDDocument35 pagesCKDgailNo ratings yet
- Dementia & DeliriumDocument170 pagesDementia & Deliriummengaku0% (1)
- Fluid Electrolytes and Acid Base BalanceDocument108 pagesFluid Electrolytes and Acid Base BalancesayednourNo ratings yet
- Fluid and ElyctrolyteDocument49 pagesFluid and Elyctrolyteuuuhbnb lplhghNo ratings yet
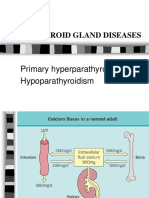
- Parathyroid Gland Diseases: Primary Hyperparathyroidism HypoparathyroidismDocument25 pagesParathyroid Gland Diseases: Primary Hyperparathyroidism HypoparathyroidismZahrah El FaradisaNo ratings yet
- Healthtalk On HEDocument8 pagesHealthtalk On HENoor HashmeeNo ratings yet
- CardiotonicsDocument21 pagesCardiotonicsmohsen mirdamadiNo ratings yet
- Liver DiseasesDocument29 pagesLiver DiseasesRicaneth TaanNo ratings yet
- DeliriumDocument27 pagesDeliriumBushra EjazNo ratings yet
- MNT in Diseases of Kidney and UrinaryDocument38 pagesMNT in Diseases of Kidney and UrinaryJosephine A. Bertulfo100% (1)
- Alzheimer Disease: Petra Nowotny, Jennifer M Kwon, Alison M GoateDocument6 pagesAlzheimer Disease: Petra Nowotny, Jennifer M Kwon, Alison M GoatedineshhissarNo ratings yet
- Spinal Cord and Head InjuryDocument31 pagesSpinal Cord and Head InjuryRiris SutrisnoNo ratings yet
- AlcoholDocument20 pagesAlcoholrecklesspeshal2058100% (1)
- Blood Donation Camp: A Humble Initiative of Dan Mitra Mandal (DMM) To Save LivesDocument26 pagesBlood Donation Camp: A Humble Initiative of Dan Mitra Mandal (DMM) To Save LivesMAHESH KOUJALAGINo ratings yet
- Constipation: Stools ExplainedDocument4 pagesConstipation: Stools ExplainedArun MuralidharanNo ratings yet
- Nephrotic and Nephritic SyndromesDocument27 pagesNephrotic and Nephritic SyndromesJoshua Smith100% (1)
- Diabetes: Causes, Symptoms and TreatmentsDocument4 pagesDiabetes: Causes, Symptoms and TreatmentsAbdullah BazryNo ratings yet
- Introduction To Management of Pneumothorax, Chest Drains & BoxesDocument96 pagesIntroduction To Management of Pneumothorax, Chest Drains & BoxesflissxloveNo ratings yet
- Promoting Personal Hygiene & Promoting Rest & SleepDocument26 pagesPromoting Personal Hygiene & Promoting Rest & SleepYousef JafarNo ratings yet
- Sweet’s Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSweet’s Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Night Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandNight Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Status ReportDocument2 pagesStatus ReportStanly stephenNo ratings yet
- Grievance RedressalDocument1 pageGrievance RedressalStanly stephenNo ratings yet
- Shiva CateringDocument3 pagesShiva CateringStanly stephenNo ratings yet
- Readme FirstDocument3 pagesReadme FirstStanly stephenNo ratings yet
- Size Max. Retail Price (Incl. of Al Plane ( ) 16x12 660 18 x12 715 20x14 935 24x16 1180 24x18 1350 30x20 1850Document4 pagesSize Max. Retail Price (Incl. of Al Plane ( ) 16x12 660 18 x12 715 20x14 935 24x16 1180 24x18 1350 30x20 1850Stanly stephenNo ratings yet
- Fshne V (Kma) ©MB V: Izt J T/M OkvDocument1 pageFshne V (Kma) ©MB V: Izt J T/M OkvStanly stephenNo ratings yet
- Physical Fitness Form Employment CertificateDocument1 pagePhysical Fitness Form Employment CertificateStanly stephenNo ratings yet
- GARCIA, JESSIE POCHOLO - JournalAnalysisDocument8 pagesGARCIA, JESSIE POCHOLO - JournalAnalysisJojo GarciaNo ratings yet
- Nutrition of Adolescent Girls in Low and Middle Income CountriesDocument12 pagesNutrition of Adolescent Girls in Low and Middle Income CountriesmanalNo ratings yet
- Iron Deficiency Without Anaemia: A Diagnosis That Matters: Authors: Abdulrahman Al-NaseemDocument7 pagesIron Deficiency Without Anaemia: A Diagnosis That Matters: Authors: Abdulrahman Al-NaseemPaulHerreraNo ratings yet
- Drug Study Baby and MotherDocument9 pagesDrug Study Baby and MotherLyra Mae E. MendozaNo ratings yet
- 29 Iron Zinc and Vitamin D Protocol EnglishDocument7 pages29 Iron Zinc and Vitamin D Protocol Englishد.شروق الهيتمىNo ratings yet
- Ectopic Pregnancy Drug Study (Vizcodne, Ehreiz Raiden C. BSN2-A)Document23 pagesEctopic Pregnancy Drug Study (Vizcodne, Ehreiz Raiden C. BSN2-A)Raiden VizcondeNo ratings yet
- Clinical ExaminationsDocument1,596 pagesClinical ExaminationsmdasNo ratings yet
- AnaemiaDocument40 pagesAnaemiaNaveen Kumar100% (1)
- Guidelines & Protocols: Advisory CommitteeDocument9 pagesGuidelines & Protocols: Advisory CommitteeeddcitoNo ratings yet
- Jurnal Buah NagaDocument6 pagesJurnal Buah NagaDian Novita AprillianaNo ratings yet
- Medicines List Medicines List: Ghana EssentialDocument37 pagesMedicines List Medicines List: Ghana EssentialportosinNo ratings yet
- RCTs in Child and Adolescent Health in Developing Countries 2021-2022Document129 pagesRCTs in Child and Adolescent Health in Developing Countries 2021-2022Sowdatu Abdullah-SandyNo ratings yet
- Physiological C-WPS OfficeDocument15 pagesPhysiological C-WPS OfficeGwagsiGlennNo ratings yet
- Drug Study 1 Ferrous SulfateDocument2 pagesDrug Study 1 Ferrous SulfateKrizzia Mae ColladoNo ratings yet
- Anemia in PregnancyDocument11 pagesAnemia in PregnancyIcetea KokomNo ratings yet
- Anemia: Iron Deficiency Vit B12 Folate DeficiencyDocument33 pagesAnemia: Iron Deficiency Vit B12 Folate DeficiencymoosaicqNo ratings yet
- LWT Nutrition 2005Document22 pagesLWT Nutrition 2005pawxblazerNo ratings yet
- Anemia of Chronic DiseaseDocument5 pagesAnemia of Chronic DiseaseGufront MustofaNo ratings yet
- Oral and Parenteral Iron Preparations in PregnancyDocument45 pagesOral and Parenteral Iron Preparations in PregnancyArun George100% (3)
- Deficiency Iron AnemiaDocument9 pagesDeficiency Iron AnemiaNadia Puspita DewiNo ratings yet
- Nursing Process Assessment (Revised Jones Criteria (American Heart Association)Document32 pagesNursing Process Assessment (Revised Jones Criteria (American Heart Association)Mamot MotNo ratings yet
- AnemiaDocument40 pagesAnemiaRajaNo ratings yet
- Discusi V Iron Deficiency AnemiaDocument34 pagesDiscusi V Iron Deficiency AnemiaErika KusumawatiNo ratings yet
- Iron Deficiency Aneamia in Adults Gutjnl 2021 325210Document22 pagesIron Deficiency Aneamia in Adults Gutjnl 2021 325210Bookgeek23No ratings yet
- A Study To Assess The Effectiveness of Massage Therapy On Respiratory Status AmongDocument28 pagesA Study To Assess The Effectiveness of Massage Therapy On Respiratory Status AmongRicha AgrawalNo ratings yet
- Commentary: Iron Deficiency of Pregnancy - A New Approach Involving Intravenous IronDocument7 pagesCommentary: Iron Deficiency of Pregnancy - A New Approach Involving Intravenous IronRaluca StaiculescuNo ratings yet
- 1471 4676 1 SMDocument5 pages1471 4676 1 SMAhmad AinurofiqNo ratings yet
- Complications of PregnancyDocument27 pagesComplications of PregnancyPatricia Anne Nicole CuaresmaNo ratings yet
- An Approach To Anemic PatientDocument79 pagesAn Approach To Anemic PatientHussain AzharNo ratings yet