Download as pptx, pdf, or txt
You might also like
- Community-Led Health Equity Impact Assessment - Save Burdett CoalitionDocument32 pagesCommunity-Led Health Equity Impact Assessment - Save Burdett CoalitionRachel SilbersteinNo ratings yet
- Nicu DesignDocument29 pagesNicu Designkowsi0% (1)
- Second TrimesterDocument11 pagesSecond Trimestermardsz100% (2)
- Multimodal Analgesia: Yusni Puspita Department of Anaesthesiology and Intensive Care Sriwijaya UniversityDocument23 pagesMultimodal Analgesia: Yusni Puspita Department of Anaesthesiology and Intensive Care Sriwijaya Universitydmandatari7327No ratings yet
- Management NyeriDocument49 pagesManagement NyeriYuke ArmikaNo ratings yet
- Manajemen Nyeri Dengan DexketoprofenDocument27 pagesManajemen Nyeri Dengan Dexketoprofenmaya santiNo ratings yet
- Neuropathic PainDocument40 pagesNeuropathic PainHasmirahNo ratings yet
- Fo Analgetik Opioid - Blok6Document65 pagesFo Analgetik Opioid - Blok6Rhena Fitria KhairunnisaNo ratings yet
- Lisa Johnson, Ba, SRS, Latg Certification Review Session 2010 Asr Annual Meeting Clearwater Beach, FLDocument33 pagesLisa Johnson, Ba, SRS, Latg Certification Review Session 2010 Asr Annual Meeting Clearwater Beach, FLAnonymous cCMY2pNo ratings yet
- Drugs Used in The Treatment of Pain and Affecting The Musculoskeletal SystemDocument34 pagesDrugs Used in The Treatment of Pain and Affecting The Musculoskeletal SystemAnna Lin YeeNo ratings yet
- Pain Dr. HenryDocument36 pagesPain Dr. Henryreagan setiawanNo ratings yet
- Acute Postoperative Pain Manila Relef.Document134 pagesAcute Postoperative Pain Manila Relef.Muchtar Luthfi100% (1)
- PAiN SYnDrOmEs (Reviewer)Document19 pagesPAiN SYnDrOmEs (Reviewer)Agum, Philip James P.No ratings yet
- Pain Assessment & ManagementDocument36 pagesPain Assessment & ManagementremeroseNo ratings yet
- Gastrits PDFDocument47 pagesGastrits PDFAnas kareemNo ratings yet
- Pain Management AulDocument23 pagesPain Management AulauliaulfaNo ratings yet
- Nyeri Dan TatalaksananyaDocument61 pagesNyeri Dan TatalaksananyaTatyana SianiparNo ratings yet
- Acute Pain Management, TIR Jakarta 20 April 2013Document47 pagesAcute Pain Management, TIR Jakarta 20 April 2013fajar alatasNo ratings yet
- Pain Management in Burn PatientsDocument17 pagesPain Management in Burn PatientsAlaa AlibrahimNo ratings yet
- PainDocument124 pagesPainWinno Pradana UtomoNo ratings yet
- A. Prof. Husni - Slide Reducing The Use of Opioid by IV Ibuprofen As Part of ERASDocument47 pagesA. Prof. Husni - Slide Reducing The Use of Opioid by IV Ibuprofen As Part of ERASharisNo ratings yet
- Pain ManagementDocument68 pagesPain Managementapi-734449276No ratings yet
- 5 Pain ManagementDocument28 pages5 Pain ManagementJANINE SEBASTIANNo ratings yet
- 2021 Update Management Pain (Dokter & Medical)Document30 pages2021 Update Management Pain (Dokter & Medical)Andri MuliaNo ratings yet
- MOD014 Nyeri KankerDocument23 pagesMOD014 Nyeri KankerMien Dwi CahyaniNo ratings yet
- Acute Periopertive Pain Management (Sby)Document87 pagesAcute Periopertive Pain Management (Sby)Adam KurniaNo ratings yet
- Balanced AnalgesicDocument37 pagesBalanced AnalgesicGia Bảo Thụy NguyễnNo ratings yet
- Mechanisms, Classification and Assesment: Departemen Neurologi Fakutas Kedokteran Universitas Islam Sumatera UtaraDocument49 pagesMechanisms, Classification and Assesment: Departemen Neurologi Fakutas Kedokteran Universitas Islam Sumatera UtaraDea indah damayantiNo ratings yet
- 4.opioids - CC - 28.10.21, 5.11.21Document70 pages4.opioids - CC - 28.10.21, 5.11.217qjyn4jtc6No ratings yet
- Can Medical Marijuana HelpDocument34 pagesCan Medical Marijuana HelpDukeNo ratings yet
- Manajemen NyeriDocument27 pagesManajemen Nyerivera100% (1)
- E PaediatricsfordoctorsDocument53 pagesE PaediatricsfordoctorsJimmy RahuNo ratings yet
- Analgesics Agents ZJDocument37 pagesAnalgesics Agents ZJDanial HassanNo ratings yet
- Pain - Nyeri Kronik Non KankerDocument25 pagesPain - Nyeri Kronik Non Kankerpowerpoint hajNo ratings yet
- Neuropathic Pain English ClassDocument38 pagesNeuropathic Pain English Classmulyaok285No ratings yet
- Analgesics N Opioids-IDocument26 pagesAnalgesics N Opioids-IshikhaNo ratings yet
- Pain Daily PracticeDocument30 pagesPain Daily Practicesukasuka azaNo ratings yet
- Peran Akupunktur Medik Pada Kasus NyeriDocument155 pagesPeran Akupunktur Medik Pada Kasus NyeriSilvia HandikaNo ratings yet
- CH12AnalgesiaLabor (9 AgustuDocument27 pagesCH12AnalgesiaLabor (9 AgustuAnonymous FX2NVrd4c2No ratings yet
- M2 PPT Treating PainDocument44 pagesM2 PPT Treating PainMeena CtNo ratings yet
- 2012-04-24 FK PainDocument49 pages2012-04-24 FK PainYanis Widhiya NingrumNo ratings yet
- Pain MGMTDocument21 pagesPain MGMTTulsi DhidhiNo ratings yet
- Tutorial Pain Management ChogaDocument26 pagesTutorial Pain Management ChogaChoga ArlandoNo ratings yet
- Pain Management - KARS Juni2021Document39 pagesPain Management - KARS Juni2021Ardian Wahyu WijayantoNo ratings yet
- Manajemen Nyeri Motik RS BhinaDocument36 pagesManajemen Nyeri Motik RS Bhinayn_faisalNo ratings yet
- Post Operative Pain Management: Dr. Golam Mursalin Phase A Cvts Dr. Rushdah Mariam Phase A Paediatric SurgeryDocument48 pagesPost Operative Pain Management: Dr. Golam Mursalin Phase A Cvts Dr. Rushdah Mariam Phase A Paediatric SurgeryRun HajNo ratings yet
- ChoosePT - Electrotherapy, Effective Alternative For Opioid Reduction? (PDFDrive)Document118 pagesChoosePT - Electrotherapy, Effective Alternative For Opioid Reduction? (PDFDrive)kk2483697No ratings yet
- Manajemen NyeriDocument33 pagesManajemen NyeriEL SHITANo ratings yet
- Physiology of Pain and Nociception IRFDocument49 pagesPhysiology of Pain and Nociception IRFZobayer AhmedNo ratings yet
- Duloxetine in The Treatment of Diabetic Peripheral Neuropathic Pain (DPNP)Document43 pagesDuloxetine in The Treatment of Diabetic Peripheral Neuropathic Pain (DPNP)gjgibson2784No ratings yet
- DR - Shinta Neuropati DiabetikDocument32 pagesDR - Shinta Neuropati DiabetikHamdan Muarifin PutraNo ratings yet
- Pain ManagementDocument78 pagesPain Managementjefri banjarnahorNo ratings yet
- Alur Manajemen Nyeri Rumah SakitDocument45 pagesAlur Manajemen Nyeri Rumah SakitRadit NasillaNo ratings yet
- Management Acute PainDocument110 pagesManagement Acute PainjohannesNo ratings yet
- DR Tommy - Cancer PainDocument60 pagesDR Tommy - Cancer Painrisalbalu100% (1)
- Acute Pain: I. Definition of TermsDocument7 pagesAcute Pain: I. Definition of TermsIsabel Castillo100% (1)
- Adjuvant Analgesics: Oxford American Pain LibraryDocument29 pagesAdjuvant Analgesics: Oxford American Pain LibraryRey AlwiwikhNo ratings yet
- Manajemen NyeriDocument30 pagesManajemen NyeriEL SHITANo ratings yet
- Bahan SharingDocument40 pagesBahan SharingkfcrajanyaayamNo ratings yet
- Mixed Pain DR Novi Irawan SPSDocument25 pagesMixed Pain DR Novi Irawan SPSnovi irawanNo ratings yet
- Fast Facts: Perioperative Pain: Effective management has numerous benefitsFrom EverandFast Facts: Perioperative Pain: Effective management has numerous benefitsNo ratings yet
- Pain Free 1-2-3: A Proven Program for Eliminating Chronic Pain NowFrom EverandPain Free 1-2-3: A Proven Program for Eliminating Chronic Pain NowRating: 1 out of 5 stars1/5 (1)
- Peripheral Receptor Targets for Analgesia: Novel Approaches to Pain ManagementFrom EverandPeripheral Receptor Targets for Analgesia: Novel Approaches to Pain ManagementNo ratings yet
- USMLE StepDocument1 pageUSMLE StepAscend KannanNo ratings yet
- Competence in Health and Mental Health: SSS 3084 Professional DevelopmentDocument35 pagesCompetence in Health and Mental Health: SSS 3084 Professional DevelopmentNurul ShahirahNo ratings yet
- Drug Study: (Celecoxib)Document11 pagesDrug Study: (Celecoxib)Princess Brigitte R. PATE�ANo ratings yet
- Alex Hardin Resume 2015Document3 pagesAlex Hardin Resume 2015api-306883462No ratings yet
- CholesteatomaDocument9 pagesCholesteatomasergeantchai068No ratings yet
- Drug Study (Case Pre)Document6 pagesDrug Study (Case Pre)Denice Fayne Amid TahiyamNo ratings yet
- Authorization To Walk HomeDocument50 pagesAuthorization To Walk HomeAidan FranciscoNo ratings yet
- Retinal DetachmentDocument6 pagesRetinal DetachmentNader Smadi100% (3)
- Ayahuasca's Antidepressant Effects Covary With Behavioral Activation As Well As MindfulnessDocument9 pagesAyahuasca's Antidepressant Effects Covary With Behavioral Activation As Well As Mindfulnesssam_rastuNo ratings yet
- Exoplan Supported Libraries @exocadDocument65 pagesExoplan Supported Libraries @exocadRaffa MarquesNo ratings yet
- Stem Cell TransplantationDocument12 pagesStem Cell Transplantationmao5074No ratings yet
- Cagayan State University College of Medicine Carig CampusDocument11 pagesCagayan State University College of Medicine Carig CampusIsabel CastilloNo ratings yet
- Gastropharm PDFDocument2 pagesGastropharm PDFKawa OmarNo ratings yet
- Links para Baixar Livros VeterináriosDocument14 pagesLinks para Baixar Livros VeterináriosBrunaFernandes33% (9)
- Anger Disorder Among Us TeensDocument3 pagesAnger Disorder Among Us TeensChristine See de BelenNo ratings yet
- Nurse To Nurse Bedside Shift Report LB 5th WeekDocument12 pagesNurse To Nurse Bedside Shift Report LB 5th Weekapi-527286440No ratings yet
- Implementing Improvement Strategies To Prevent Unplanned Extubation in Neonatal Intensive Care Units - SLIDE DECKDocument19 pagesImplementing Improvement Strategies To Prevent Unplanned Extubation in Neonatal Intensive Care Units - SLIDE DECKeman hamzaNo ratings yet
- Case Analysis SchizophreniaDocument2 pagesCase Analysis Schizophreniamark OrpillaNo ratings yet
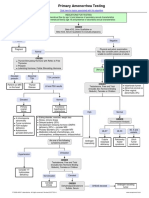
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet
- Brugada SyndromeDocument5 pagesBrugada SyndromevitriaNo ratings yet
- Terapi Cairan Resusitasi: DR Arief Munandar, Span, Kic Bagian Anestesi - Icu Rsud BrebesDocument34 pagesTerapi Cairan Resusitasi: DR Arief Munandar, Span, Kic Bagian Anestesi - Icu Rsud BrebesWistha MiyakiNo ratings yet
- Family Nursing Care PlanDocument3 pagesFamily Nursing Care PlanJarda DacuagNo ratings yet
- PPDDocument2 pagesPPDMaheen KalwarNo ratings yet
- Kupit 1Document16 pagesKupit 1wayan sudarsanaNo ratings yet
- Homeopathy: 1 HistoryDocument32 pagesHomeopathy: 1 HistoryslowdogNo ratings yet
- Cosmetic AcupunctureDocument3 pagesCosmetic Acupuncturejanachidambaram100% (1)
- Ealing - Directory of Services For Older PeopleDocument132 pagesEaling - Directory of Services For Older PeopleFaty AbdjaNo ratings yet