Download as ppt, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Concept of Child Friendly SchoolDocument23 pagesThe Concept of Child Friendly SchoolJussa Leilady AlberbaNo ratings yet
- Treatment: Visceral Leishmaniasis: Visceral Leishmaniasis (VL), Also Known As Kala-Azar, Black Fever, and Dumdum FeverDocument3 pagesTreatment: Visceral Leishmaniasis: Visceral Leishmaniasis (VL), Also Known As Kala-Azar, Black Fever, and Dumdum FeverbournvilleeaterNo ratings yet
- WHO-UMC Causality CategoriesDocument2 pagesWHO-UMC Causality CategoriesbournvilleeaterNo ratings yet
- Drugeluting StentDocument2 pagesDrugeluting StentbournvilleeaterNo ratings yet
- Vasoactive Intestinal PeptideDocument2 pagesVasoactive Intestinal PeptidebournvilleeaterNo ratings yet
- Creatinine ClearanceDocument2 pagesCreatinine Clearancebournvilleeater100% (1)
- The HPV Virus and TypesDocument8 pagesThe HPV Virus and TypesbournvilleeaterNo ratings yet
- Standard Treatment GuidelinesDocument5 pagesStandard Treatment Guidelinesbournvilleeater100% (1)
- Antimicrobial ProphylaxisDocument2 pagesAntimicrobial ProphylaxisbournvilleeaterNo ratings yet
- Tamil Nadu Common Admissions 2020: (TANCA 2020)Document36 pagesTamil Nadu Common Admissions 2020: (TANCA 2020)k.l yuvarajNo ratings yet
- Nuclear Medicine LogbookDocument26 pagesNuclear Medicine LogbookMayuran SaththianathanNo ratings yet
- PALSCourseDocument39 pagesPALSCourseMicki BurgerNo ratings yet
- Banana Nutrition Health BenefitsDocument9 pagesBanana Nutrition Health BenefitsUmar PervezNo ratings yet
- Haemonetics Cell Saver CS5Document8 pagesHaemonetics Cell Saver CS5zairmendesNo ratings yet
- Diagnostic Procedures in Respiratory DiseaseDocument41 pagesDiagnostic Procedures in Respiratory DiseaseVio Mincu50% (2)
- Taffix Scientific Story June 2021Document41 pagesTaffix Scientific Story June 2021Sanja IlićNo ratings yet
- Hemorrhagic StrokeDocument30 pagesHemorrhagic StrokeAstrina SupandyNo ratings yet
- Chandrashekhar LIC 1193406093228formsDocument12 pagesChandrashekhar LIC 1193406093228formsShahil KumarNo ratings yet
- Drugs Affecting The Body SystemDocument3 pagesDrugs Affecting The Body SystemKhzNo ratings yet
- Continuous Insulin InfusionDocument6 pagesContinuous Insulin Infusionbobobo22No ratings yet
- Clinical Review: Aphasia: An OverviewDocument31 pagesClinical Review: Aphasia: An OverviewRashid HussainNo ratings yet
- Clinical Manifestations, Pathologic Features, and Diagnosis of Peripheral T Cell Lymphoma, Not Otherwise Specified - UpToDateDocument16 pagesClinical Manifestations, Pathologic Features, and Diagnosis of Peripheral T Cell Lymphoma, Not Otherwise Specified - UpToDatePablo ZeregaNo ratings yet
- Yuwell Bpap User ManuelDocument25 pagesYuwell Bpap User Manuelsermed100% (1)
- Next-Generation SequencingDocument6 pagesNext-Generation SequencingvisiniNo ratings yet
- Hypo & Hyper ThermiaDocument55 pagesHypo & Hyper ThermiafmedicineNo ratings yet
- Anti-Acne Activity of Garcinia Mangostana L.: A ReviewDocument4 pagesAnti-Acne Activity of Garcinia Mangostana L.: A ReviewifaNo ratings yet
- Avandia - The Intimidation of Dr. John BuseDocument12 pagesAvandia - The Intimidation of Dr. John BuseVaccineInformation100% (1)
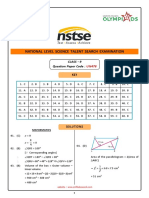
- CL 9 Nstse 2022 Paper 478 KeyDocument7 pagesCL 9 Nstse 2022 Paper 478 KeyVilas DewadeNo ratings yet
- RABIESDocument60 pagesRABIESJoice JosephNo ratings yet
- BN6209 NotesDocument3 pagesBN6209 NotesShaun BuxaniNo ratings yet
- Root, Prefix or Suffix Meaning ExamplesDocument18 pagesRoot, Prefix or Suffix Meaning ExamplesDikshant DahivaleyNo ratings yet
- Adult Assessment: Head To Toe Assessment Is The Baseline and Ongoing Data That Is Needed OnDocument2 pagesAdult Assessment: Head To Toe Assessment Is The Baseline and Ongoing Data That Is Needed OnAldrin NavarroNo ratings yet
- Varatika BhasmaDocument5 pagesVaratika Bhasmadrsa2No ratings yet
- Disposable Collection Tubes of Virus Samples: Instruction For UseDocument3 pagesDisposable Collection Tubes of Virus Samples: Instruction For Usemelly faisha rahmaNo ratings yet
- UNAS B.inggrisDocument6 pagesUNAS B.inggrisintan kartikaNo ratings yet
- Gat Exam 1Document16 pagesGat Exam 1snewemail1234No ratings yet
- Comprehensive Textbook of SurgeryDocument338 pagesComprehensive Textbook of SurgeryAdel Saleh100% (2)
- Ug DentalDocument4 pagesUg Dentaldeepak162162No ratings yet