Download as pptx, pdf, or txt
You might also like
- ProActive Training Case Study 4Document8 pagesProActive Training Case Study 4danthemanyvr100% (1)
- The Shoulder and Shoulder GirdleDocument43 pagesThe Shoulder and Shoulder GirdleMuhammad UsmanNo ratings yet
- ICD-9-CM Codes: ICF Codes:: d4452 Reaching (Using The Hands and Arms To ExtendDocument13 pagesICD-9-CM Codes: ICF Codes:: d4452 Reaching (Using The Hands and Arms To ExtendAbdul Wahid ShaikhNo ratings yet
- Scapular Stabilization ExercisesDocument2 pagesScapular Stabilization ExercisesnimitrisNo ratings yet
- Arthroscopic Shoulder Anterior Stabilisation Rehabilitation Protocol by TENDAYI MUTSOPOTSI MSc. ORTHO-MEDDocument8 pagesArthroscopic Shoulder Anterior Stabilisation Rehabilitation Protocol by TENDAYI MUTSOPOTSI MSc. ORTHO-MEDPhysiotherapy Care SpecialistsNo ratings yet
- Nonsurgical Shoulder Impingement Rehabilitation Protocol: Ramin R. Tabaddor, MD Arlene D. Kavanagh, PA-CDocument4 pagesNonsurgical Shoulder Impingement Rehabilitation Protocol: Ramin R. Tabaddor, MD Arlene D. Kavanagh, PA-CRiaz KhanNo ratings yet
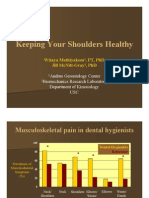
- Keeping Your Shoulders HealthyDocument38 pagesKeeping Your Shoulders Healthyxyz84No ratings yet
- Upper Limb Fractures - Physiotherapy PDFDocument52 pagesUpper Limb Fractures - Physiotherapy PDFaliprasanna85% (13)
- Slap Lesion Repair Rehabilitation ProtocolDocument5 pagesSlap Lesion Repair Rehabilitation ProtocolNadine RomeroNo ratings yet
- Frozen ShoulderDocument18 pagesFrozen ShoulderChitra ChauhanNo ratings yet
- Rot at or Cuff TendonitisDocument4 pagesRot at or Cuff Tendonitisreo1910No ratings yet
- Physical Therapy After Rotator Cuff RepairDocument19 pagesPhysical Therapy After Rotator Cuff RepairMaria RosmaNo ratings yet
- Physiotherapy Rotator Cuff RepairDocument2 pagesPhysiotherapy Rotator Cuff Repairjohn hagisNo ratings yet
- Scoliosis ManagementDocument17 pagesScoliosis ManagementNeha DhobaleNo ratings yet
- Meniscus Injury: Khairul Nizam Abdul Rahman 4262143008Document22 pagesMeniscus Injury: Khairul Nizam Abdul Rahman 4262143008Soumashree MondalNo ratings yet
- Rehabilitation Protocol For Acromioclavicular Joint ReconstructionDocument3 pagesRehabilitation Protocol For Acromioclavicular Joint ReconstructionGeorge MagarakisNo ratings yet
- IVDP: Inter Vertebral Disc ProlapseDocument34 pagesIVDP: Inter Vertebral Disc ProlapseShibinNo ratings yet
- AC Dislocation RehabDocument8 pagesAC Dislocation Rehabandrea.miruna1999No ratings yet
- Supervised Clinical Practice-III: AssignmentDocument12 pagesSupervised Clinical Practice-III: Assignmentzainab siddiqueNo ratings yet
- Management of Elbow Common Injuries: Functional Anatomy Mechanics Epicondylitis Post Immobilization Capsular TightnessDocument31 pagesManagement of Elbow Common Injuries: Functional Anatomy Mechanics Epicondylitis Post Immobilization Capsular TightnessAmany Abd ELfatah HassanNo ratings yet
- Bicipital TendinitisDocument19 pagesBicipital TendinitisRonak PatelNo ratings yet
- I. Etiology Primary Adhesive Capsulitis Secondary Adhesive CapsulitisDocument8 pagesI. Etiology Primary Adhesive Capsulitis Secondary Adhesive CapsulitisVanessa Yvonne Gurtiza100% (1)
- Shoulder Impinge MentDocument26 pagesShoulder Impinge MentkotraeNo ratings yet
- Mitland For Cevical SpineDocument52 pagesMitland For Cevical SpineMohamed RamadanNo ratings yet
- Functional Reeducation Techniques: Presenter by Arambam Meiteileima Chanu 1 Year, MPT (Neuro)Document38 pagesFunctional Reeducation Techniques: Presenter by Arambam Meiteileima Chanu 1 Year, MPT (Neuro)deepuphysio94% (18)
- AC ReconstructionDocument3 pagesAC Reconstructionryanbroad82No ratings yet
- ORIF Proximal Humerus FracturesDocument2 pagesORIF Proximal Humerus FracturesAdriano Luiz BarbosaNo ratings yet
- Joint MobilizationDocument42 pagesJoint MobilizationSérgio Xavier Silva100% (1)
- McKenzie LumbarDocument51 pagesMcKenzie LumbarRouqia HamedNo ratings yet
- Rotator-Cuff-Repair Eggert 1015Document3 pagesRotator-Cuff-Repair Eggert 1015Sorin IordacheNo ratings yet
- Ankylosing SpondylytisDocument6 pagesAnkylosing SpondylytisMurad KurdiNo ratings yet
- Cervical Spondylosis With RadiculopathyDocument26 pagesCervical Spondylosis With RadiculopathyKashish SahotaNo ratings yet
- Acl PCL PresentationDocument17 pagesAcl PCL PresentationSafwan Idham RamlanNo ratings yet
- PE046 Proximal Hamstring Tendinopathy With Tom Goom HandoutDocument5 pagesPE046 Proximal Hamstring Tendinopathy With Tom Goom Handoutmajd.rezkallahNo ratings yet
- Rehabilitation Protocol For Posterior Cruciate Ligament PCLRDocument7 pagesRehabilitation Protocol For Posterior Cruciate Ligament PCLRrahul sharmaNo ratings yet
- Kinetics & Kinematics Od ADLDocument26 pagesKinetics & Kinematics Od ADLPriyanka kedare100% (1)
- Sport Traumatology-III Knee Complex-10Document26 pagesSport Traumatology-III Knee Complex-10kamran aliNo ratings yet
- Physio Protocol Anterior Shoulder Dislocation NEW ADD 1Document2 pagesPhysio Protocol Anterior Shoulder Dislocation NEW ADD 1Abner SánchezNo ratings yet
- Clinical Presentation 2.0Document61 pagesClinical Presentation 2.0Danial AdliNo ratings yet
- Trunk Stability by Calvin Morriss, PHD.: What Exactly Is Trunk Stability For A Rugby Player?Document9 pagesTrunk Stability by Calvin Morriss, PHD.: What Exactly Is Trunk Stability For A Rugby Player?Justice Man100% (1)
- PHTH 302 Exercises For Lumbar Instability PresentationDocument21 pagesPHTH 302 Exercises For Lumbar Instability Presentationmanx100% (1)
- نسخة light blue creative modern medical clinic presentationDocument33 pagesنسخة light blue creative modern medical clinic presentationFaresNo ratings yet
- Epicondylitis Repair - Rehab ProtocolDocument2 pagesEpicondylitis Repair - Rehab ProtocolKiara BrownNo ratings yet
- Rehabilitation Protocol For ACLDocument9 pagesRehabilitation Protocol For ACLgb tradeNo ratings yet
- ACL ReconstructionDocument4 pagesACL Reconstructionredbull227No ratings yet
- Lumbar Strain: Dr. Lipy Bhat PT Faculty, Physiotherapy SrhuDocument38 pagesLumbar Strain: Dr. Lipy Bhat PT Faculty, Physiotherapy SrhuKapil LakhwaraNo ratings yet
- Rehabilitation Protocol For Meniscus RepairDocument16 pagesRehabilitation Protocol For Meniscus RepairAnonymous ecI8GUbaNo ratings yet
- An Introduction To The Mckenzie Method: Treating Your Own BackDocument24 pagesAn Introduction To The Mckenzie Method: Treating Your Own BackR HariNo ratings yet
- Kine 2nd YearDocument21 pagesKine 2nd YearzeeshanNo ratings yet
- MPFL PDFDocument12 pagesMPFL PDFFydananda NPNo ratings yet
- Total Hip Arthroplasty PDFDocument10 pagesTotal Hip Arthroplasty PDFWindy ZeniccNo ratings yet
- Brunnstorm ApproachDocument70 pagesBrunnstorm Approachkomal khannaNo ratings yet
- Physical Therapy ProtocolsDocument33 pagesPhysical Therapy ProtocolsdrprasantNo ratings yet
- Arthroscopic Rotator Cuff Repair Protocol:: Peter J. Millett, MD, MSCDocument4 pagesArthroscopic Rotator Cuff Repair Protocol:: Peter J. Millett, MD, MSCPhooi Yee LauNo ratings yet
- Case 1Document19 pagesCase 1jagdish030798No ratings yet
- Evaluating Shoulder InjuriesDocument37 pagesEvaluating Shoulder InjuriesEmily EresumaNo ratings yet
- Lect. 3 (Test 2) - 2023Document22 pagesLect. 3 (Test 2) - 2023nagyrashad123No ratings yet
- Run With No Pain: A Step-by-Step Exercise Solution for Eliminating Low Back Pain in AthletesFrom EverandRun With No Pain: A Step-by-Step Exercise Solution for Eliminating Low Back Pain in AthletesNo ratings yet
- Holistic Home Remedies for Acute Low Back Pain: Incorporating Stretching and the McKenzie MethodFrom EverandHolistic Home Remedies for Acute Low Back Pain: Incorporating Stretching and the McKenzie MethodNo ratings yet
- How to Get Rid of Back Pain: A Comprehensive Technique that Will Help Get Rid of Lower Back Pain, in the Upper Back and NeckFrom EverandHow to Get Rid of Back Pain: A Comprehensive Technique that Will Help Get Rid of Lower Back Pain, in the Upper Back and NeckNo ratings yet
- DiksaDocument19 pagesDiksaDeepak SharmaNo ratings yet
- ArticleDocument7 pagesArticleKiran AbidNo ratings yet
- Comparacion de Kaltenborn Versus Mulligan InglesDocument6 pagesComparacion de Kaltenborn Versus Mulligan Inglesmauricio castroNo ratings yet
- Schwerla 2020Document8 pagesSchwerla 2020João Paulo Vila Nova GomesNo ratings yet
- Frozen Shoulder: By: Denise Dela CruzDocument44 pagesFrozen Shoulder: By: Denise Dela CruzDenise De la Cruz100% (1)
- MET Vs ConventionalDocument6 pagesMET Vs ConventionalPoorvin ShahNo ratings yet
- Adhesive Capsulitis: Braddom's ClassificationDocument2 pagesAdhesive Capsulitis: Braddom's ClassificationJJ DdNo ratings yet
- Manipulation Under Anesthesia For Periarthritis ShoulderDocument3 pagesManipulation Under Anesthesia For Periarthritis ShoulderasclepiuspdfsNo ratings yet
- Lalitha Ps Lalithas Reiki and Sujok AcupressureDocument204 pagesLalitha Ps Lalithas Reiki and Sujok AcupressureElif Atasayan100% (1)
- 8 Proses Fisioterpi Anggota Gerak, Temu 8Document61 pages8 Proses Fisioterpi Anggota Gerak, Temu 8oetari putriNo ratings yet
- The Effectiveness of The Combination of Neuromuscular Taping (NMT) and Codman Pendulum Exercise To Improve The Functional Ability of The Shoulder in Patients With Frozen ShouldersDocument3 pagesThe Effectiveness of The Combination of Neuromuscular Taping (NMT) and Codman Pendulum Exercise To Improve The Functional Ability of The Shoulder in Patients With Frozen ShouldersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Frozen Shoulder JurnalDocument10 pagesFrozen Shoulder JurnalShiba MiyukiNo ratings yet
- IontophoresisDocument6 pagesIontophoresisNamrathaThalatoti ywSSAmHsULNo ratings yet
- Frozen Shoulder - Adhesive CapsulitisDocument8 pagesFrozen Shoulder - Adhesive CapsulitisfriskaNo ratings yet
- VenkateshDocument94 pagesVenkateshpriya selvarajNo ratings yet
- Bowen Therapy: A Good Move For Every BodyDocument12 pagesBowen Therapy: A Good Move For Every BodyLiviaNo ratings yet
- Frozen Shoulder FinalDocument3 pagesFrozen Shoulder FinalRatnaPrasadNalamNo ratings yet
- Management of Frozen Shoulder by Leech Therapy and Adjuvant Phytotherapy: A Case StudyDocument12 pagesManagement of Frozen Shoulder by Leech Therapy and Adjuvant Phytotherapy: A Case StudyNealNo ratings yet
- Effectiveness of Maitland vs. Mulligan Mobilization Techniques in (Ingles)Document4 pagesEffectiveness of Maitland vs. Mulligan Mobilization Techniques in (Ingles)mauricio castroNo ratings yet
- Frozen ShoulderDocument110 pagesFrozen ShoulderAchmad ZulfikarNo ratings yet
- Koding Tindakan FisioterapiDocument5 pagesKoding Tindakan Fisioterapifisioterapi pelamoniaNo ratings yet
- Frozen ShoulderDocument18 pagesFrozen ShoulderChitra ChauhanNo ratings yet
- Bone and Joint Infection: Dr. Zainab AbdulwahabDocument89 pagesBone and Joint Infection: Dr. Zainab Abdulwahabzen.maree6No ratings yet
- The Role of Occupational TherapyDocument27 pagesThe Role of Occupational TherapyPa T EthiopiaNo ratings yet
- Frozen Shoulder (Buku Komplit Etiologi DLL)Document7 pagesFrozen Shoulder (Buku Komplit Etiologi DLL)Ricky Diah Ayu AnggrainiNo ratings yet
- Treatment of Adhesive Capsulitis of The Shoulder-1Document12 pagesTreatment of Adhesive Capsulitis of The Shoulder-1JONATHAN IVANNo ratings yet
- Frozen Shoulder RevisedDocument17 pagesFrozen Shoulder Revisednerissa arvianaNo ratings yet
- Jeremy Lewis Shoulder T and P 22nd EdDocument3 pagesJeremy Lewis Shoulder T and P 22nd EdDr Abdallah BahaaNo ratings yet
- Frozen Shoulder DessertationDocument61 pagesFrozen Shoulder DessertationPoorvin ShahNo ratings yet