
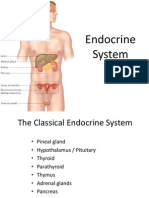
Endocrine System
Endocrine System
You might also like
- SCIENCE-10-Q3 WORKSHEET REVISED COPY-week-1-7Document46 pagesSCIENCE-10-Q3 WORKSHEET REVISED COPY-week-1-7Gian Evangelista67% (6)
- Boys and Puberty BookletDocument9 pagesBoys and Puberty Bookletఫణీంద్ర నర్సెట్టి50% (2)
- Endocrine SystemDocument96 pagesEndocrine SystemSandhya Kakkar100% (3)
- LECTURE 1 Endocrine Diseases Lecture 1 January 10-020Document68 pagesLECTURE 1 Endocrine Diseases Lecture 1 January 10-020aleen qawareetNo ratings yet
- endocrine فسيولوجياDocument49 pagesendocrine فسيولوجياAUDEH AHMADNo ratings yet
- Endocrine PhysiologyDocument98 pagesEndocrine PhysiologyMohan GuptaNo ratings yet
- ENDOCRINE SYSTEM DISORDERS PROPER BestDocument370 pagesENDOCRINE SYSTEM DISORDERS PROPER BestronaronixstheboyNo ratings yet
- Hormones 080623Document83 pagesHormones 080623Rao Asad MubeenNo ratings yet
- Hypothalamus and Pituitary GlandDocument62 pagesHypothalamus and Pituitary GlandphyMedza AppNo ratings yet
- Endocrinology Endocrinology: H. KibichoDocument370 pagesEndocrinology Endocrinology: H. KibichoMursal RashidNo ratings yet
- CBSE Quick Revision Notes (Class-11 Biology) Chapter-22 Chemical Coordination and IntegrationDocument3 pagesCBSE Quick Revision Notes (Class-11 Biology) Chapter-22 Chemical Coordination and IntegrationNANDAKUMAR BABUNo ratings yet
- CBSE Quick Revision Notes (Class-11 Biology) Chapter-22 Chemical Coordination and IntegrationDocument3 pagesCBSE Quick Revision Notes (Class-11 Biology) Chapter-22 Chemical Coordination and IntegrationNANDAKUMAR BABUNo ratings yet
- Ila College of Health: Endocrine PhysiologyDocument40 pagesIla College of Health: Endocrine PhysiologyDaniel DendaNo ratings yet
- Regulasi Endokrin 22 IntensifDocument25 pagesRegulasi Endokrin 22 IntensifWignes WarenNo ratings yet
- Hormonal BiochemistryDocument82 pagesHormonal BiochemistryRuthNo ratings yet
- Endocrine GlandsDocument36 pagesEndocrine GlandsnasyitahnorzlanNo ratings yet
- Hypothalamus & Pituitary GlandDocument39 pagesHypothalamus & Pituitary GlandVishal DodejaNo ratings yet
- Pituitary and ThyroidDocument54 pagesPituitary and ThyroidSaif AliNo ratings yet
- Endocrine SystemDocument30 pagesEndocrine SystemAkshat RastogiNo ratings yet
- Endocrine System: Endocrine: Which Have No Duct and ReleaseDocument36 pagesEndocrine System: Endocrine: Which Have No Duct and Releasedr_saleh77No ratings yet
- Hormones:: Signaling MoleculesDocument20 pagesHormones:: Signaling MoleculesSangeeta DwivediNo ratings yet
- EndocrineDocument94 pagesEndocrineHira NawazNo ratings yet
- Endo AnaphysioDocument9 pagesEndo AnaphysioShelley Jade MenorNo ratings yet
- Seminor On Hormons Slide2 by Prof - Dr.HariharDocument49 pagesSeminor On Hormons Slide2 by Prof - Dr.Hariharhariharb999_23960100No ratings yet
- HormonesDocument29 pagesHormonesCandy Chieng67% (3)
- Endocrine System - MorphophysiologyDocument88 pagesEndocrine System - MorphophysiologyKarina Bustillo100% (1)
- Metabolic & Endocrine DiseasesDocument280 pagesMetabolic & Endocrine DiseasesHussenNo ratings yet
- Hormones (Short Version)Document80 pagesHormones (Short Version)Vivek ChaudharyNo ratings yet
- HORMONESDocument65 pagesHORMONESsoumya palavalasaNo ratings yet
- Physiology 1STDocument10 pagesPhysiology 1STGW LEGENDNo ratings yet
- Endocrine PhysiologyDocument76 pagesEndocrine Physiologykidusabeje7No ratings yet
- Endocrine Anatomy and PhysiologyDocument10 pagesEndocrine Anatomy and PhysiologyJojo JustoNo ratings yet
- Hypothalamus and Pituitary GlandDocument48 pagesHypothalamus and Pituitary GlandMohsin AbbasNo ratings yet
- Endocrinology Apllied ScienceDocument44 pagesEndocrinology Apllied ScienceAdam PrabowoNo ratings yet
- The Endocrine System The Endocrine System: © 2018 Pearson Education, Ltd. 1Document12 pagesThe Endocrine System The Endocrine System: © 2018 Pearson Education, Ltd. 1lourd nabNo ratings yet
- Endocrine SystemDocument30 pagesEndocrine SystemBrenda Domaneo BaseNo ratings yet
- Endocrine Physiology For AnsthesiaDocument60 pagesEndocrine Physiology For AnsthesiaCHALIE MEQUNo ratings yet
- The Endocrine System PDFDocument27 pagesThe Endocrine System PDFpratiksha.bhattacharjeeNo ratings yet
- Endocrine SystemDocument22 pagesEndocrine SystemkwatsNo ratings yet
- Endocrine SystemDocument18 pagesEndocrine SystemDioh EmmanuelNo ratings yet
- Chemical Coordination and IntegrationDocument6 pagesChemical Coordination and IntegrationRonaldNo ratings yet
- Endocrine SystemDocument41 pagesEndocrine SystemMerrin EncarnacionNo ratings yet
- The Endocrine System: Endocrine Gland (Ductless Gland)Document50 pagesThe Endocrine System: Endocrine Gland (Ductless Gland)Mohammad AliNo ratings yet
- Quick Revision NotesDocument3 pagesQuick Revision NoteslinzihaoleoNo ratings yet
- Chemical Coordination and Integration Handwriten Notes For Neet and JeeDocument5 pagesChemical Coordination and Integration Handwriten Notes For Neet and JeetechnosonicindiaNo ratings yet
- PD22 Hap1 L03Document33 pagesPD22 Hap1 L03Ka Yan LAUNo ratings yet
- EndocrinologyDocument74 pagesEndocrinologysyedahaleemajunaidsNo ratings yet
- Biochemistry of Hormones (Part 1)Document31 pagesBiochemistry of Hormones (Part 1)arun231187100% (1)
- Endocrine System/socialDocument33 pagesEndocrine System/socialrpant3165No ratings yet
- Option D - Unit 5 - HormonesDocument28 pagesOption D - Unit 5 - Hormonesjanafahmy1211No ratings yet
- Unit IXDocument10 pagesUnit IXPreeti ChouhanNo ratings yet
- Anatomy and Physiology of The Endocrine System: Presenté ParDocument64 pagesAnatomy and Physiology of The Endocrine System: Presenté ParYackson Frank100% (1)
- UntitledDocument12 pagesUntitledDerrick kinyaNo ratings yet
- Endocrine System: Glands & HormonesDocument78 pagesEndocrine System: Glands & HormonesJerilee SoCute WattsNo ratings yet
- 4 Pituitary HormonesDocument18 pages4 Pituitary HormonesRana AbdullahNo ratings yet
- Functional Anatomy and PhysiologyDocument38 pagesFunctional Anatomy and PhysiologyNawalNo ratings yet
- EndocrinologyDocument37 pagesEndocrinologyKochaMsangiNo ratings yet
- Hormones: Mark Angelo R. Jacosalem Faye Bernadette O. Reyes Ma. Elizabeth VerteraDocument40 pagesHormones: Mark Angelo R. Jacosalem Faye Bernadette O. Reyes Ma. Elizabeth VerteraGelo Robin JacosalemNo ratings yet
- Principles of Hormonal Control SystemDocument25 pagesPrinciples of Hormonal Control SystemFAHEEM UD DINNo ratings yet
- Hormones SubtopicsDocument77 pagesHormones SubtopicsSulaiman UmraniNo ratings yet
- Balancing Hormones Naturally: A Woman's Guide to Hormonal Harmony: HealthFrom EverandBalancing Hormones Naturally: A Woman's Guide to Hormonal Harmony: HealthNo ratings yet
- Thyroid Health: The Thyroid Solution Diet ExposedFrom EverandThyroid Health: The Thyroid Solution Diet ExposedRating: 3 out of 5 stars3/5 (2)
- Nervous SystemDocument140 pagesNervous SystemDivya JaiswalNo ratings yet
- 1 General Anatomy - Levels of Organization EtcDocument36 pages1 General Anatomy - Levels of Organization EtcDivya JaiswalNo ratings yet
- General Anatomy - 4Document22 pagesGeneral Anatomy - 4Divya JaiswalNo ratings yet
- 6 Human Anatomy - Muscular SystemDocument34 pages6 Human Anatomy - Muscular SystemDivya JaiswalNo ratings yet
- Acute Interstitial NephritisDocument36 pagesAcute Interstitial NephritisosaqerNo ratings yet
- CHOLECYSTITIS CASE STUDY Version 2.0Document57 pagesCHOLECYSTITIS CASE STUDY Version 2.0Gabriel Arch100% (1)
- Cara Membaca Foto Thoraks Yang BaikDocument2 pagesCara Membaca Foto Thoraks Yang BaikIdi Nagan RayaNo ratings yet
- IBDP Biology Option - D - SummaryDocument5 pagesIBDP Biology Option - D - SummaryRafi FarhanNo ratings yet
- Case Pres HydronephrosisDocument39 pagesCase Pres HydronephrosisLouie Dela Cruz100% (3)
- Review Article: Relevant Biliary Anatomy During CholecystectomyDocument11 pagesReview Article: Relevant Biliary Anatomy During CholecystectomyAbrar SabawiNo ratings yet
- PHPY 303 - GI Lecture #1 - March 10Document30 pagesPHPY 303 - GI Lecture #1 - March 10smhallmobileNo ratings yet
- General Surgery: (Gallbladder Disease)Document1 pageGeneral Surgery: (Gallbladder Disease)Matt100% (1)
- PHYSIOLOGYDocument10 pagesPHYSIOLOGYapi-1986354875% (4)
- Chapter 13 - The Peripheral Nervous System and Reflex ActivityDocument53 pagesChapter 13 - The Peripheral Nervous System and Reflex Activityramadan100% (1)
- Science 8 - 3Document5 pagesScience 8 - 3Sherine Marianne IgnacioNo ratings yet
- Jurnal 2 (2019)Document11 pagesJurnal 2 (2019)Inryuu ZenNo ratings yet
- Mod 8 ZooDocument10 pagesMod 8 ZooLM Tricia T. DE LA CRUZNo ratings yet
- B - SC Nursing I Year SyllabusDocument159 pagesB - SC Nursing I Year SyllabusSusheelabaiNo ratings yet
- Heart, Nerve and Mucsle, Membrane Transport Mcqs With KeyDocument8 pagesHeart, Nerve and Mucsle, Membrane Transport Mcqs With KeyMudassar Roomi100% (7)
- Brain Computer InterfaceDocument11 pagesBrain Computer InterfaceNeha ArifNo ratings yet
- Acute GlomerulonephritisDocument18 pagesAcute GlomerulonephritisdanielaNo ratings yet
- Anatomia de Puntos Craneometricos PDFDocument35 pagesAnatomia de Puntos Craneometricos PDFAlberto SalazarNo ratings yet
- Chapter 39 AntihypertensivesDocument4 pagesChapter 39 AntihypertensivesErika Joy Cabison TamayoNo ratings yet
- Benign Thyroid DiseasesDocument138 pagesBenign Thyroid DiseasesAliNo ratings yet
- 07 Post Mortem Examination (Autopsy)Document48 pages07 Post Mortem Examination (Autopsy)ARIF-UR-REHMAN100% (5)
- Previous Year'S Questions (Excretion)Document1 pagePrevious Year'S Questions (Excretion)veeresh punjaniNo ratings yet
- Digestive System in Non-RuminantsDocument5 pagesDigestive System in Non-RuminantsTumisang TlhabanoNo ratings yet
- Bikram Yoga PosturesDocument4 pagesBikram Yoga PosturesMony SánchezNo ratings yet
- Science6 ST1 Q2Document4 pagesScience6 ST1 Q2Meriam LuatNo ratings yet
- Chapter 10 - Immune Responses Against Tumors and TransplantsDocument11 pagesChapter 10 - Immune Responses Against Tumors and TransplantsFYMNo ratings yet
- Li 1 Anatomy, Histology, PhysiologyDocument17 pagesLi 1 Anatomy, Histology, PhysiologysandyaadindaNo ratings yet
- Lipids Metabolism ReviewerDocument2 pagesLipids Metabolism RevieweroperanacireNo ratings yet

























































































Download as pptx, pdf, or txt
You might also like
- SCIENCE-10-Q3 WORKSHEET REVISED COPY-week-1-7Document46 pagesSCIENCE-10-Q3 WORKSHEET REVISED COPY-week-1-7Gian Evangelista67% (6)
- Boys and Puberty BookletDocument9 pagesBoys and Puberty Bookletఫణీంద్ర నర్సెట్టి50% (2)
- Endocrine SystemDocument96 pagesEndocrine SystemSandhya Kakkar100% (3)
- LECTURE 1 Endocrine Diseases Lecture 1 January 10-020Document68 pagesLECTURE 1 Endocrine Diseases Lecture 1 January 10-020aleen qawareetNo ratings yet
- endocrine فسيولوجياDocument49 pagesendocrine فسيولوجياAUDEH AHMADNo ratings yet
- Endocrine PhysiologyDocument98 pagesEndocrine PhysiologyMohan GuptaNo ratings yet
- ENDOCRINE SYSTEM DISORDERS PROPER BestDocument370 pagesENDOCRINE SYSTEM DISORDERS PROPER BestronaronixstheboyNo ratings yet
- Hormones 080623Document83 pagesHormones 080623Rao Asad MubeenNo ratings yet
- Hypothalamus and Pituitary GlandDocument62 pagesHypothalamus and Pituitary GlandphyMedza AppNo ratings yet
- Endocrinology Endocrinology: H. KibichoDocument370 pagesEndocrinology Endocrinology: H. KibichoMursal RashidNo ratings yet
- CBSE Quick Revision Notes (Class-11 Biology) Chapter-22 Chemical Coordination and IntegrationDocument3 pagesCBSE Quick Revision Notes (Class-11 Biology) Chapter-22 Chemical Coordination and IntegrationNANDAKUMAR BABUNo ratings yet
- CBSE Quick Revision Notes (Class-11 Biology) Chapter-22 Chemical Coordination and IntegrationDocument3 pagesCBSE Quick Revision Notes (Class-11 Biology) Chapter-22 Chemical Coordination and IntegrationNANDAKUMAR BABUNo ratings yet
- Ila College of Health: Endocrine PhysiologyDocument40 pagesIla College of Health: Endocrine PhysiologyDaniel DendaNo ratings yet
- Regulasi Endokrin 22 IntensifDocument25 pagesRegulasi Endokrin 22 IntensifWignes WarenNo ratings yet
- Hormonal BiochemistryDocument82 pagesHormonal BiochemistryRuthNo ratings yet
- Endocrine GlandsDocument36 pagesEndocrine GlandsnasyitahnorzlanNo ratings yet
- Hypothalamus & Pituitary GlandDocument39 pagesHypothalamus & Pituitary GlandVishal DodejaNo ratings yet
- Pituitary and ThyroidDocument54 pagesPituitary and ThyroidSaif AliNo ratings yet
- Endocrine SystemDocument30 pagesEndocrine SystemAkshat RastogiNo ratings yet
- Endocrine System: Endocrine: Which Have No Duct and ReleaseDocument36 pagesEndocrine System: Endocrine: Which Have No Duct and Releasedr_saleh77No ratings yet
- Hormones:: Signaling MoleculesDocument20 pagesHormones:: Signaling MoleculesSangeeta DwivediNo ratings yet
- EndocrineDocument94 pagesEndocrineHira NawazNo ratings yet
- Endo AnaphysioDocument9 pagesEndo AnaphysioShelley Jade MenorNo ratings yet
- Seminor On Hormons Slide2 by Prof - Dr.HariharDocument49 pagesSeminor On Hormons Slide2 by Prof - Dr.Hariharhariharb999_23960100No ratings yet
- HormonesDocument29 pagesHormonesCandy Chieng67% (3)
- Endocrine System - MorphophysiologyDocument88 pagesEndocrine System - MorphophysiologyKarina Bustillo100% (1)
- Metabolic & Endocrine DiseasesDocument280 pagesMetabolic & Endocrine DiseasesHussenNo ratings yet
- Hormones (Short Version)Document80 pagesHormones (Short Version)Vivek ChaudharyNo ratings yet
- HORMONESDocument65 pagesHORMONESsoumya palavalasaNo ratings yet
- Physiology 1STDocument10 pagesPhysiology 1STGW LEGENDNo ratings yet
- Endocrine PhysiologyDocument76 pagesEndocrine Physiologykidusabeje7No ratings yet
- Endocrine Anatomy and PhysiologyDocument10 pagesEndocrine Anatomy and PhysiologyJojo JustoNo ratings yet
- Hypothalamus and Pituitary GlandDocument48 pagesHypothalamus and Pituitary GlandMohsin AbbasNo ratings yet
- Endocrinology Apllied ScienceDocument44 pagesEndocrinology Apllied ScienceAdam PrabowoNo ratings yet
- The Endocrine System The Endocrine System: © 2018 Pearson Education, Ltd. 1Document12 pagesThe Endocrine System The Endocrine System: © 2018 Pearson Education, Ltd. 1lourd nabNo ratings yet
- Endocrine SystemDocument30 pagesEndocrine SystemBrenda Domaneo BaseNo ratings yet
- Endocrine Physiology For AnsthesiaDocument60 pagesEndocrine Physiology For AnsthesiaCHALIE MEQUNo ratings yet
- The Endocrine System PDFDocument27 pagesThe Endocrine System PDFpratiksha.bhattacharjeeNo ratings yet
- Endocrine SystemDocument22 pagesEndocrine SystemkwatsNo ratings yet
- Endocrine SystemDocument18 pagesEndocrine SystemDioh EmmanuelNo ratings yet
- Chemical Coordination and IntegrationDocument6 pagesChemical Coordination and IntegrationRonaldNo ratings yet
- Endocrine SystemDocument41 pagesEndocrine SystemMerrin EncarnacionNo ratings yet
- The Endocrine System: Endocrine Gland (Ductless Gland)Document50 pagesThe Endocrine System: Endocrine Gland (Ductless Gland)Mohammad AliNo ratings yet
- Quick Revision NotesDocument3 pagesQuick Revision NoteslinzihaoleoNo ratings yet
- Chemical Coordination and Integration Handwriten Notes For Neet and JeeDocument5 pagesChemical Coordination and Integration Handwriten Notes For Neet and JeetechnosonicindiaNo ratings yet
- PD22 Hap1 L03Document33 pagesPD22 Hap1 L03Ka Yan LAUNo ratings yet
- EndocrinologyDocument74 pagesEndocrinologysyedahaleemajunaidsNo ratings yet
- Biochemistry of Hormones (Part 1)Document31 pagesBiochemistry of Hormones (Part 1)arun231187100% (1)
- Endocrine System/socialDocument33 pagesEndocrine System/socialrpant3165No ratings yet
- Option D - Unit 5 - HormonesDocument28 pagesOption D - Unit 5 - Hormonesjanafahmy1211No ratings yet
- Unit IXDocument10 pagesUnit IXPreeti ChouhanNo ratings yet
- Anatomy and Physiology of The Endocrine System: Presenté ParDocument64 pagesAnatomy and Physiology of The Endocrine System: Presenté ParYackson Frank100% (1)
- UntitledDocument12 pagesUntitledDerrick kinyaNo ratings yet
- Endocrine System: Glands & HormonesDocument78 pagesEndocrine System: Glands & HormonesJerilee SoCute WattsNo ratings yet
- 4 Pituitary HormonesDocument18 pages4 Pituitary HormonesRana AbdullahNo ratings yet
- Functional Anatomy and PhysiologyDocument38 pagesFunctional Anatomy and PhysiologyNawalNo ratings yet
- EndocrinologyDocument37 pagesEndocrinologyKochaMsangiNo ratings yet
- Hormones: Mark Angelo R. Jacosalem Faye Bernadette O. Reyes Ma. Elizabeth VerteraDocument40 pagesHormones: Mark Angelo R. Jacosalem Faye Bernadette O. Reyes Ma. Elizabeth VerteraGelo Robin JacosalemNo ratings yet
- Principles of Hormonal Control SystemDocument25 pagesPrinciples of Hormonal Control SystemFAHEEM UD DINNo ratings yet
- Hormones SubtopicsDocument77 pagesHormones SubtopicsSulaiman UmraniNo ratings yet
- Balancing Hormones Naturally: A Woman's Guide to Hormonal Harmony: HealthFrom EverandBalancing Hormones Naturally: A Woman's Guide to Hormonal Harmony: HealthNo ratings yet
- Thyroid Health: The Thyroid Solution Diet ExposedFrom EverandThyroid Health: The Thyroid Solution Diet ExposedRating: 3 out of 5 stars3/5 (2)
- Nervous SystemDocument140 pagesNervous SystemDivya JaiswalNo ratings yet
- 1 General Anatomy - Levels of Organization EtcDocument36 pages1 General Anatomy - Levels of Organization EtcDivya JaiswalNo ratings yet
- General Anatomy - 4Document22 pagesGeneral Anatomy - 4Divya JaiswalNo ratings yet
- 6 Human Anatomy - Muscular SystemDocument34 pages6 Human Anatomy - Muscular SystemDivya JaiswalNo ratings yet
- Acute Interstitial NephritisDocument36 pagesAcute Interstitial NephritisosaqerNo ratings yet
- CHOLECYSTITIS CASE STUDY Version 2.0Document57 pagesCHOLECYSTITIS CASE STUDY Version 2.0Gabriel Arch100% (1)
- Cara Membaca Foto Thoraks Yang BaikDocument2 pagesCara Membaca Foto Thoraks Yang BaikIdi Nagan RayaNo ratings yet
- IBDP Biology Option - D - SummaryDocument5 pagesIBDP Biology Option - D - SummaryRafi FarhanNo ratings yet
- Case Pres HydronephrosisDocument39 pagesCase Pres HydronephrosisLouie Dela Cruz100% (3)
- Review Article: Relevant Biliary Anatomy During CholecystectomyDocument11 pagesReview Article: Relevant Biliary Anatomy During CholecystectomyAbrar SabawiNo ratings yet
- PHPY 303 - GI Lecture #1 - March 10Document30 pagesPHPY 303 - GI Lecture #1 - March 10smhallmobileNo ratings yet
- General Surgery: (Gallbladder Disease)Document1 pageGeneral Surgery: (Gallbladder Disease)Matt100% (1)
- PHYSIOLOGYDocument10 pagesPHYSIOLOGYapi-1986354875% (4)
- Chapter 13 - The Peripheral Nervous System and Reflex ActivityDocument53 pagesChapter 13 - The Peripheral Nervous System and Reflex Activityramadan100% (1)
- Science 8 - 3Document5 pagesScience 8 - 3Sherine Marianne IgnacioNo ratings yet
- Jurnal 2 (2019)Document11 pagesJurnal 2 (2019)Inryuu ZenNo ratings yet
- Mod 8 ZooDocument10 pagesMod 8 ZooLM Tricia T. DE LA CRUZNo ratings yet
- B - SC Nursing I Year SyllabusDocument159 pagesB - SC Nursing I Year SyllabusSusheelabaiNo ratings yet
- Heart, Nerve and Mucsle, Membrane Transport Mcqs With KeyDocument8 pagesHeart, Nerve and Mucsle, Membrane Transport Mcqs With KeyMudassar Roomi100% (7)
- Brain Computer InterfaceDocument11 pagesBrain Computer InterfaceNeha ArifNo ratings yet
- Acute GlomerulonephritisDocument18 pagesAcute GlomerulonephritisdanielaNo ratings yet
- Anatomia de Puntos Craneometricos PDFDocument35 pagesAnatomia de Puntos Craneometricos PDFAlberto SalazarNo ratings yet
- Chapter 39 AntihypertensivesDocument4 pagesChapter 39 AntihypertensivesErika Joy Cabison TamayoNo ratings yet
- Benign Thyroid DiseasesDocument138 pagesBenign Thyroid DiseasesAliNo ratings yet
- 07 Post Mortem Examination (Autopsy)Document48 pages07 Post Mortem Examination (Autopsy)ARIF-UR-REHMAN100% (5)
- Previous Year'S Questions (Excretion)Document1 pagePrevious Year'S Questions (Excretion)veeresh punjaniNo ratings yet
- Digestive System in Non-RuminantsDocument5 pagesDigestive System in Non-RuminantsTumisang TlhabanoNo ratings yet
- Bikram Yoga PosturesDocument4 pagesBikram Yoga PosturesMony SánchezNo ratings yet
- Science6 ST1 Q2Document4 pagesScience6 ST1 Q2Meriam LuatNo ratings yet
- Chapter 10 - Immune Responses Against Tumors and TransplantsDocument11 pagesChapter 10 - Immune Responses Against Tumors and TransplantsFYMNo ratings yet
- Li 1 Anatomy, Histology, PhysiologyDocument17 pagesLi 1 Anatomy, Histology, PhysiologysandyaadindaNo ratings yet
- Lipids Metabolism ReviewerDocument2 pagesLipids Metabolism RevieweroperanacireNo ratings yet