Download as pptx, pdf, or txt
You might also like
- Neurophysiology and AnaesthesiaDocument54 pagesNeurophysiology and AnaesthesiaBernard Panggabean100% (1)
- BILAG EnglishDocument2 pagesBILAG EnglishJohn Althom Aduna MendozaNo ratings yet
- Student Case Study Example Template Free Download PDFDocument14 pagesStudent Case Study Example Template Free Download PDFNana YaaNo ratings yet
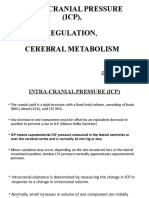
- Intra-Cranial Pressure (ICP), Regulation, Cerebral MetabolismDocument18 pagesIntra-Cranial Pressure (ICP), Regulation, Cerebral MetabolismPraveen RamasamyNo ratings yet
- Increased Intracranial PressureDocument48 pagesIncreased Intracranial PressureJulia Rae Delos SantosNo ratings yet
- Cerebral ProtectionDocument51 pagesCerebral ProtectionhanselMD100% (1)
- 3 - IcpDocument57 pages3 - IcpNathaniel BudayNo ratings yet
- Cerebral CirculationDocument16 pagesCerebral Circulationvarrakesh100% (1)
- Increased Intracranial PressureDocument20 pagesIncreased Intracranial Pressuremamiyo71No ratings yet
- Brainedema 160314142234Document39 pagesBrainedema 160314142234Lulu LuwiiNo ratings yet
- 4.3 Neuro - ICP (Student)Document39 pages4.3 Neuro - ICP (Student)EliMariICNo ratings yet
- Controlled Hypotension: Moderator: DR V. Y. Srinivas Presenter: Dr. Ann Susan MathewDocument49 pagesControlled Hypotension: Moderator: DR V. Y. Srinivas Presenter: Dr. Ann Susan MathewAnn Susan MathewNo ratings yet
- Lec 3 4 ICP EllenDocument61 pagesLec 3 4 ICP Ellenkatherinerance331No ratings yet
- Intracranial Pressure (Icp) : Mohd Roslee Bin Abd GhaniDocument25 pagesIntracranial Pressure (Icp) : Mohd Roslee Bin Abd GhaniSaha DirllahNo ratings yet
- Tekanan Intra KranialDocument31 pagesTekanan Intra KranialUtari DzayNo ratings yet
- Raised Intracranial Pressure: BY DR - Tallat Pervaiz AliDocument37 pagesRaised Intracranial Pressure: BY DR - Tallat Pervaiz AliCh Khurram HasnainNo ratings yet
- Head Trauma: Will/Grundy EMS 2009 2 Trimester May CMEDocument100 pagesHead Trauma: Will/Grundy EMS 2009 2 Trimester May CMESytrose Morales100% (1)
- Brain Edema & It's ManagementDocument26 pagesBrain Edema & It's ManagementMohammed FareedNo ratings yet
- Increased Intracranial PressureDocument10 pagesIncreased Intracranial Pressureapi-3822433100% (10)
- Blood Pressure: Dr. Dev K Shah Assistant Professor Dept of PhysiologyDocument23 pagesBlood Pressure: Dr. Dev K Shah Assistant Professor Dept of Physiologysapana shresthaNo ratings yet
- Cardiovascular Physiology: Dr. Roger Joseph Ii R. JecinoDocument17 pagesCardiovascular Physiology: Dr. Roger Joseph Ii R. JecinoFranz Earl Niño AlbesaNo ratings yet
- MNCHN Finals Coverage NEUROLOGIC DISORDERSDocument8 pagesMNCHN Finals Coverage NEUROLOGIC DISORDERSChryzl JoyNo ratings yet
- Effect of Anesthetic AgentsDocument26 pagesEffect of Anesthetic AgentsefrikoNo ratings yet
- Shock: Erdiansyah Zulyadaini, MD, FIHA FK Universitas Muhammadiyah Purwokerto/ RSUD Dr. Soeselo Kabupaten TegalDocument47 pagesShock: Erdiansyah Zulyadaini, MD, FIHA FK Universitas Muhammadiyah Purwokerto/ RSUD Dr. Soeselo Kabupaten TegalFarah AkhwanisNo ratings yet
- Persentation Anesthesia For Supratentorial TumorsDocument35 pagesPersentation Anesthesia For Supratentorial TumorsChalis NovrizaNo ratings yet
- 6.neurologic PathophysiologyDocument173 pages6.neurologic PathophysiologybekaluNo ratings yet
- Intracranial Pressure (ICP) : Causes, Concerns and ManagementDocument37 pagesIntracranial Pressure (ICP) : Causes, Concerns and ManagementGus LionsNo ratings yet
- Intracranial Pressure: Dr. Akhmad Imron, Spbs Dept. of NeurosurgeryDocument26 pagesIntracranial Pressure: Dr. Akhmad Imron, Spbs Dept. of Neurosurgeryandisti2323No ratings yet
- Intra-Cranial PressureDocument36 pagesIntra-Cranial PressureKapil LakhwaraNo ratings yet
- Intracranial Pressure 2015: Samir El AnsaryDocument76 pagesIntracranial Pressure 2015: Samir El AnsaryIkhsan FebriansyahNo ratings yet
- Paediatric Intracranial PressureDocument29 pagesPaediatric Intracranial PressuredratiqurNo ratings yet
- Selim Mahmoud Abdel-Hakim: by Professor DRDocument27 pagesSelim Mahmoud Abdel-Hakim: by Professor DRAhmed TarekNo ratings yet
- UNIT-5 Pharmacology of NeurosurgeryDocument12 pagesUNIT-5 Pharmacology of NeurosurgeryFaizan Mazhar100% (1)
- Central Nervous System: Zalak Patel, MBBSDocument25 pagesCentral Nervous System: Zalak Patel, MBBSMinaz PatelNo ratings yet
- Icp and Anaesthesia DrugsDocument56 pagesIcp and Anaesthesia DrugsKhawer MuneerNo ratings yet
- ShockDocument68 pagesShockseries recapNo ratings yet
- Traumatic Head InjuriesDocument50 pagesTraumatic Head InjuriesVasudha BuddyNo ratings yet
- PHS 213 Wk11 Cardiac output-BPDocument33 pagesPHS 213 Wk11 Cardiac output-BPPRINCE ADEWUMI JONATHANNo ratings yet
- 2.1 - Increased Intracranial PressureDocument45 pages2.1 - Increased Intracranial PressureRose AnnNo ratings yet
- Shock: Presenters-Selahadin Awol - Yohannes TekuDocument88 pagesShock: Presenters-Selahadin Awol - Yohannes TekuYaniNo ratings yet
- Cerebral PhysiologyDocument27 pagesCerebral PhysiologyArmaanjeet SinghNo ratings yet
- Rossalia Yuliana - Inhalation AnestheticsDocument24 pagesRossalia Yuliana - Inhalation Anestheticsputra syawalNo ratings yet
- Management of Client With Neurologic Trauma Anatomy of The CraniumDocument17 pagesManagement of Client With Neurologic Trauma Anatomy of The CraniumGoldie Reroma GelagaNo ratings yet
- Curs 3 ShockDocument78 pagesCurs 3 ShockIoana CNo ratings yet
- MS Lec IicpDocument4 pagesMS Lec IicpTrishia Camille GuillermoNo ratings yet
- Brunner Normal Intracranial Pressure 10-20 MMHGDocument16 pagesBrunner Normal Intracranial Pressure 10-20 MMHGlovely99_dyahNo ratings yet
- Increased Intracranial Pressure: DR - Muhammad Yusuf, Sps FinsDocument61 pagesIncreased Intracranial Pressure: DR - Muhammad Yusuf, Sps FinsFidhiyahR100% (1)
- Increased of Intracranial Pressure and Brain Herniation SyndromeDocument33 pagesIncreased of Intracranial Pressure and Brain Herniation SyndromeIda Benecia DeseNo ratings yet
- Elavated Intracranial Pressure: (Edema, Herniation, Hydrocephalus)Document8 pagesElavated Intracranial Pressure: (Edema, Herniation, Hydrocephalus)Aazril71No ratings yet
- IcpDocument30 pagesIcpalia nanohanoNo ratings yet
- Vas Opressor 233Document55 pagesVas Opressor 233songsokalinNo ratings yet
- Increased Intracranial Pressure Is A Rise in TheDocument3 pagesIncreased Intracranial Pressure Is A Rise in TheMark Anthony Dela CruzNo ratings yet
- L15-Shock & Resuscitation LectureDocument49 pagesL15-Shock & Resuscitation LectureYosra —No ratings yet
- Shock: Curs Studenti An ViDocument78 pagesShock: Curs Studenti An ViAnonymous dKiLqVS3L5No ratings yet
- Reponse of Brain Tissue To Trauma: Intracranial PressureDocument29 pagesReponse of Brain Tissue To Trauma: Intracranial Pressurevijaykadam_ndaNo ratings yet
- Diagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaDocument51 pagesDiagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaHilmaNo ratings yet
- Management of Shock in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sceinces Kochi, KeralaDocument77 pagesManagement of Shock in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sceinces Kochi, KeralaAETCM Emergency medicineNo ratings yet
- NeuroDocument16 pagesNeuroBrandon Goodman100% (3)
- The HeartDocument12 pagesThe HeartRafsae Iqbal AkbarNo ratings yet
- Drugs Acting in CVSDocument63 pagesDrugs Acting in CVSMeghan Norico Cristuta100% (1)
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- The Spectrum of Amniotic Fluid Embolism: Is Intralipid the solution ?From EverandThe Spectrum of Amniotic Fluid Embolism: Is Intralipid the solution ?No ratings yet
- FCPS Pulmonogy CPSP Course BookletDocument32 pagesFCPS Pulmonogy CPSP Course BookletQiblaHazoor100% (1)
- Basic Ecg: A Report By: Clinical Clerk Mary Hazel TeDocument74 pagesBasic Ecg: A Report By: Clinical Clerk Mary Hazel TeHazel Arcosa100% (1)
- Worksheet - Circulatory SystemDocument3 pagesWorksheet - Circulatory SystemAlireza KafaeiNo ratings yet
- 4 5827715801091672558Document903 pages4 5827715801091672558rvictorbrNo ratings yet
- Urinary Tract InfectionsDocument68 pagesUrinary Tract InfectionsYajjat GargNo ratings yet
- Pathophysiology Respiratory SystemDocument63 pagesPathophysiology Respiratory SystemAli Basha QudahNo ratings yet
- Bedside Cardiology (2012) (PDF)Document251 pagesBedside Cardiology (2012) (PDF)Loredana Dobrea100% (4)
- CV MECH - Final Exam Jan 14Document12 pagesCV MECH - Final Exam Jan 14Ibrahim Basar AkaNo ratings yet
- Jurnal CT Cardiac 3Document27 pagesJurnal CT Cardiac 3Kakhfi Gemah PNo ratings yet
- Massage and The Lymphatic SystemDocument9 pagesMassage and The Lymphatic Systemarmanious64No ratings yet
- Hematuria Treatment Management and Required ConsultationsDocument10 pagesHematuria Treatment Management and Required ConsultationsDiyana ZatyNo ratings yet
- Nurse Case StudyDocument25 pagesNurse Case StudyAlreem Alhajry100% (1)
- Heart AnatomyDocument7 pagesHeart AnatomyArjon BalaNo ratings yet
- List of AbreviationDocument44 pagesList of Abreviationdapsjen deadNo ratings yet
- Treatment of Ischemic StrokeDocument9 pagesTreatment of Ischemic Strokeka 66No ratings yet
- PDF Handbook of Cardiac Electrophysiology Second Edition Kalyanam Shivkumar Editor Ebook Full ChapterDocument63 pagesPDF Handbook of Cardiac Electrophysiology Second Edition Kalyanam Shivkumar Editor Ebook Full Chapterthomas.mitchell310100% (3)
- Krok 1 - 2015 (Physiology)Document28 pagesKrok 1 - 2015 (Physiology)mayna ynaNo ratings yet
- Daftar DiagnosaDocument6 pagesDaftar DiagnosaSr Immaculata SSpSNo ratings yet
- Chapter 31 Dyslipidemia UpdatedDocument37 pagesChapter 31 Dyslipidemia UpdatedMai TarekNo ratings yet
- Chronic Disease ManagementDocument46 pagesChronic Disease Managementpea_ciha05No ratings yet
- Congenital Lobar EmphysemaDocument3 pagesCongenital Lobar Emphysemamadimadi11No ratings yet
- hssb3001t SecquizDocument2 pageshssb3001t SecquizA7mad MomenNo ratings yet
- Surgery CaseDocument4 pagesSurgery CaseVincent SomidoNo ratings yet
- Bad Effects of SmokingDocument16 pagesBad Effects of SmokingMarko Papa Radman0% (1)
- Textbook Scleroderma From Pathogenesis To Comprehensive Management 2Nd Edition John Varga Ebook All Chapter PDFDocument53 pagesTextbook Scleroderma From Pathogenesis To Comprehensive Management 2Nd Edition John Varga Ebook All Chapter PDFjohn.wammack573100% (2)
- CPR Class QuestionnaireDocument4 pagesCPR Class QuestionnaireParikshit PekhaleNo ratings yet
- Product ListDocument2 pagesProduct ListErwin WinNo ratings yet
- Kode Kombinasi & Kode GandaDocument15 pagesKode Kombinasi & Kode GandaJuwitahasugianNo ratings yet