Download as ppt, pdf, or txt
You might also like
- Dental Care For Patients With Heart Failure: An UpdateDocument9 pagesDental Care For Patients With Heart Failure: An UpdateGustavo A OrtegonNo ratings yet
- Cabin Crew Medical StandardsDocument5 pagesCabin Crew Medical StandardsCatalin Stelian-ShanksNo ratings yet
- Rheumatic Heart DiseaseDocument30 pagesRheumatic Heart DiseasejustinahorroNo ratings yet
- Communicable Diseasesp.170 199Document30 pagesCommunicable Diseasesp.170 199Gary Largosa GallardoNo ratings yet
- Patho Unit 5Document37 pagesPatho Unit 5Shafiya ShaikNo ratings yet
- Antibiotics For CssDocument38 pagesAntibiotics For CsstayyabsaifNo ratings yet
- Case Study of Most Common Communicable DiseasesDocument13 pagesCase Study of Most Common Communicable DiseasesnesjynNo ratings yet
- Antibiotics, Vaccines and Diseases-1Document38 pagesAntibiotics, Vaccines and Diseases-1Siraj Jan SoomroNo ratings yet
- Polio: Bacteria Clostridium TetaniDocument6 pagesPolio: Bacteria Clostridium TetaniLovelyn Joy Abubo CortezNo ratings yet
- Communicable DiseasesDocument101 pagesCommunicable DiseasesKira100% (4)
- Herpes ZosterDocument6 pagesHerpes ZosterRonan suhendraNo ratings yet
- Diseases PIDSRDocument25 pagesDiseases PIDSRaringkinking100% (1)
- Common Tropical DiseasesDocument19 pagesCommon Tropical DiseasesMarko TomicNo ratings yet
- Acute Febrile IllnessesDocument54 pagesAcute Febrile IllnessesfraolNo ratings yet
- Typhoid FeverDocument9 pagesTyphoid FeverValerrie NgenoNo ratings yet
- HIV InfectionDocument13 pagesHIV Infectionsun shineNo ratings yet
- Typhoid FeverDocument3 pagesTyphoid Feverdejay100No ratings yet
- BACTERIAL DISEASES AND LABORATORY DIAGNOSIS 200LDocument8 pagesBACTERIAL DISEASES AND LABORATORY DIAGNOSIS 200Ladetuaduramigba12No ratings yet
- Locally Endemic DiseasesDocument23 pagesLocally Endemic DiseasesERMIAS, ZENDY I.No ratings yet
- Symptoms, Complications and Prevention of Typhoid FeverDocument3 pagesSymptoms, Complications and Prevention of Typhoid Feverhasandsome100% (1)
- Feco-Orally Transmitted Diseases: (Diseases Transmitted by Contaminated Water, Food, and Others)Document133 pagesFeco-Orally Transmitted Diseases: (Diseases Transmitted by Contaminated Water, Food, and Others)TekletsadikNo ratings yet
- Chapter-8-Human Health (SM)Document24 pagesChapter-8-Human Health (SM)zahraababy123No ratings yet
- Viral Infection: NAME-Rahul Pawar (Roll No.17) Sanket Joshi (Roll No.25)Document25 pagesViral Infection: NAME-Rahul Pawar (Roll No.17) Sanket Joshi (Roll No.25)aditya_aditya_mayekar199No ratings yet
- COMMUNICABLE DISEASES - Power Point PDFDocument143 pagesCOMMUNICABLE DISEASES - Power Point PDFGel Marie LobatonNo ratings yet
- Vaccines and Target DiseasesDocument43 pagesVaccines and Target Diseaseszedregga2No ratings yet
- Typhus Fever SetDocument3 pagesTyphus Fever SetIra TadikaNo ratings yet
- Human Health and Disease What Is Health?Document40 pagesHuman Health and Disease What Is Health?JANE ONGNo ratings yet
- Typhoid Fever PPT 30-3-10Document97 pagesTyphoid Fever PPT 30-3-10Anonymous hYMWbA100% (1)
- ExplanationDocument6 pagesExplanationLerma PagcaliwanganNo ratings yet
- Typhoid FeverDocument8 pagesTyphoid FeverKomang Mery100% (1)
- Rheumatic Fever Small Group DiscussionDocument13 pagesRheumatic Fever Small Group DiscussionLyca Mae AurelioNo ratings yet
- Rheumatic FeverDocument6 pagesRheumatic FeverSam AraNo ratings yet
- Typhoid Fever: by Dr. Bambang SN, SP - PD Department of Internal Medicine, General Hospital of Dr. Soedarso, PontianakDocument32 pagesTyphoid Fever: by Dr. Bambang SN, SP - PD Department of Internal Medicine, General Hospital of Dr. Soedarso, PontianakTriponiaNo ratings yet
- 伤寒英文教案 Typhoid Fever-应若素Document36 pages伤寒英文教案 Typhoid Fever-应若素Wai Kwong ChiuNo ratings yet
- Dengue Fever Health TeachingDocument9 pagesDengue Fever Health TeachingChris Tine CaccamNo ratings yet
- Communicable Diseases HandoutsDocument15 pagesCommunicable Diseases HandoutsLloyd LozanoNo ratings yet
- PBL 1 InfectiousDocument9 pagesPBL 1 InfectiousHassaan-e MuhammedNo ratings yet
- A. Infectious ProcessDocument22 pagesA. Infectious ProcessKyla Malapit GarvidaNo ratings yet
- PediatricsDocument31 pagesPediatricsLuai Tuma KhouryNo ratings yet
- Vaccine Preventable Communicable DiseasesDocument7 pagesVaccine Preventable Communicable DiseasesmadmarycashNo ratings yet
- CHN211 Week 7 PPT - National Immunization ProgramDocument85 pagesCHN211 Week 7 PPT - National Immunization ProgramZEPHANNY ANNE TABBAYNo ratings yet
- Presented By: Gayramara Arben John ZDocument36 pagesPresented By: Gayramara Arben John ZgoykicoshenNo ratings yet
- 1-Rheumatic Heart Disease and EndocarditisDocument69 pages1-Rheumatic Heart Disease and EndocarditisHamzehNo ratings yet
- RNA Non Enveloped VirusesDocument35 pagesRNA Non Enveloped VirusesRPh Krishna Chandra JagritNo ratings yet
- Inf MononucleosysDocument46 pagesInf MononucleosysStefan MarinNo ratings yet
- Vaccination Chart: National Immunization Schedule For New BornDocument20 pagesVaccination Chart: National Immunization Schedule For New BornsmilealwplzNo ratings yet
- Crux 05Document8 pagesCrux 05Rajkishor YadavNo ratings yet
- Gram + DiseasesDocument30 pagesGram + DiseasesveerdedajiNo ratings yet
- 1.2 Leptospirosis Dengue Fever Malaria Filariais EncephalitisDocument95 pages1.2 Leptospirosis Dengue Fever Malaria Filariais Encephalitisesbercinio8528valNo ratings yet
- Communicable DiseasesDocument7 pagesCommunicable DiseasesRaisa Robelle Quicho100% (1)
- Typhoid FeverDocument37 pagesTyphoid FeverMuqtadir “The Ruler” KuchikiNo ratings yet
- Meningitis Pathophysiology PDFDocument59 pagesMeningitis Pathophysiology PDFpaswordnyalupa100% (1)
- IMMS Viruses. Basics: A-And A-Interferon A-InterferonDocument4 pagesIMMS Viruses. Basics: A-And A-Interferon A-Interferonrosanna_hildersleyNo ratings yet
- Systemic Infections From GiDocument10 pagesSystemic Infections From GiJake MillerNo ratings yet
- Vaccine PreventableDocument89 pagesVaccine PreventableMohammad Doctor CabdiraxmanNo ratings yet
- CH 8 - Human Health and Diseases - NottesDocument61 pagesCH 8 - Human Health and Diseases - NottesGopalNo ratings yet
- Enteric FeverDocument7 pagesEnteric FeverkudzaimuregidubeNo ratings yet
- Haepatitis - EDocument5 pagesHaepatitis - ERatnaPrasadNalamNo ratings yet
- Diseases of Nervous SystemDocument30 pagesDiseases of Nervous SystemBangtan SonyeondanNo ratings yet
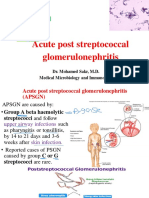
- Micro PSGNDocument32 pagesMicro PSGNMahmoud hilmyNo ratings yet
- Female Urinary Tract Infections in Clinical PracticeFrom EverandFemale Urinary Tract Infections in Clinical PracticeBob YangNo ratings yet
- EthergineDocument3 pagesEthergineVictor CondeNo ratings yet
- Essay QuestionsDocument3 pagesEssay QuestionsAxsa AlexNo ratings yet
- WhatsApp Infographic2 PDFDocument1 pageWhatsApp Infographic2 PDFRevanth TNo ratings yet
- Mix Questions PDFDocument40 pagesMix Questions PDFZazo RawashdehNo ratings yet
- Gout Part 1 ACR-12-0014-1Document16 pagesGout Part 1 ACR-12-0014-1vitauxianaNo ratings yet
- Case Study: Treating Hypertension in Patients With DiabetesDocument10 pagesCase Study: Treating Hypertension in Patients With Diabetesfirda rydNo ratings yet
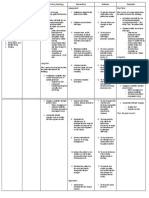
- NCP Preeclampsia and EclampsiaDocument16 pagesNCP Preeclampsia and EclampsiaBiway Regala100% (1)
- A Technical Report On Towobola 4Document18 pagesA Technical Report On Towobola 4obakuromicheal4199No ratings yet
- Pathophysiology of Portal Hypertension: Dr. Eeman At-Taras Dr. Mohamed Al-Saeid SulimanDocument29 pagesPathophysiology of Portal Hypertension: Dr. Eeman At-Taras Dr. Mohamed Al-Saeid SulimanDenata Prabhasiwi100% (1)
- 8 Laws of Health: Streams of Light MinistryDocument9 pages8 Laws of Health: Streams of Light Ministryanjani kumarNo ratings yet
- Pregnancy Induced Hypertension Case StudyDocument75 pagesPregnancy Induced Hypertension Case StudyJing CruzNo ratings yet
- Comprehensive Nursing ProcessDocument17 pagesComprehensive Nursing Processm100% (1)
- Department of Education: Republic of The PhilippinesDocument4 pagesDepartment of Education: Republic of The PhilippinesJeane Pineda ReyesNo ratings yet
- Lifestyle Diseases Affecting The Nursing Faculty at Tarlac State University During Covid 19 PandemicDocument19 pagesLifestyle Diseases Affecting The Nursing Faculty at Tarlac State University During Covid 19 PandemicDeinielle Magdangal RomeroNo ratings yet
- Hypertension (Hypertensive Urgency)Document2 pagesHypertension (Hypertensive Urgency)itsmeayaNo ratings yet
- Manuskrip: Oleh: Dias Syaima Husniyah NIM. 1501009Document12 pagesManuskrip: Oleh: Dias Syaima Husniyah NIM. 1501009elsaNo ratings yet
- AMARACHI WORK FinalizedDocument67 pagesAMARACHI WORK FinalizedocNo ratings yet
- Jurnal Biokimia KalsiumDocument5 pagesJurnal Biokimia KalsiumdimitriprawiraNo ratings yet
- HypertensionDocument2 pagesHypertensionsigit_riyantono100% (1)
- PQCNC: Hypertension in PregnancyDocument79 pagesPQCNC: Hypertension in PregnancykcochranNo ratings yet
- CG241 2011-08 Common Ground MagazineDocument36 pagesCG241 2011-08 Common Ground MagazineCommonGroundBCNo ratings yet
- Cardiovascular Disease in PregnancyDocument6 pagesCardiovascular Disease in Pregnancyneeta rajesh bhideNo ratings yet
- NCM 0114 Module 3 - Nursing Care Management of The Older Person With Chronic IllnessDocument84 pagesNCM 0114 Module 3 - Nursing Care Management of The Older Person With Chronic IllnessKristine Kim100% (1)
- Wa0027Document20 pagesWa0027Ahmed ElshiekhNo ratings yet
- Renal Case StudyDocument4 pagesRenal Case Studydsaitta108No ratings yet
- NCP Decreased Cardiac Output 1Document2 pagesNCP Decreased Cardiac Output 1Arnel MacabalitaoNo ratings yet
- Kaigo Prometric Lesson (Eng)Document108 pagesKaigo Prometric Lesson (Eng)Ysmech SalazarNo ratings yet
- EpistaxisDocument12 pagesEpistaxisalputraNo ratings yet