Download as pptx, pdf, or txt
You might also like
- Pharmacology in Rehabilitation 4th Edition Ciccone Test BankDocument25 pagesPharmacology in Rehabilitation 4th Edition Ciccone Test BankRyanRoseJrbden98% (56)
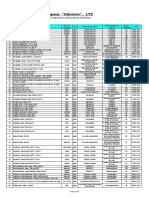
- Pharmaceutical Company "Zdorovye", LTD: Price-List (USD) 03.09.2019Document10 pagesPharmaceutical Company "Zdorovye", LTD: Price-List (USD) 03.09.2019Laura Del valleNo ratings yet
- Medical Emergencies in The Dental OfficeDocument100 pagesMedical Emergencies in The Dental OfficeSaleh Ahmed Saleh Ahmed100% (1)
- Respiratory ManagementDocument61 pagesRespiratory ManagementAjimsha ShoukathNo ratings yet
- Procedural Sedation in EDDocument41 pagesProcedural Sedation in EDadam NoheNo ratings yet
- Medical Emergencies: Sobia RubabDocument31 pagesMedical Emergencies: Sobia RubabNigam SattarNo ratings yet
- Intravenous Parenteral Sedation 1Document77 pagesIntravenous Parenteral Sedation 1yousra qadiNo ratings yet
- Sedation & General Anesthesia: SMF Anestesiologi & Reanimasi, Intensive Care Rsud JayapuraDocument50 pagesSedation & General Anesthesia: SMF Anestesiologi & Reanimasi, Intensive Care Rsud JayapuraubayyumrNo ratings yet
- Conscious Sedation: A Brief Overview Janette Lafroscia, Rces, Rcis, RcsDocument26 pagesConscious Sedation: A Brief Overview Janette Lafroscia, Rces, Rcis, RcsrnvisNo ratings yet
- Pharmacological Behavior Management in Pediatric Dentistry: MSC - Bds. Belkays M. Omran AbubakrDocument32 pagesPharmacological Behavior Management in Pediatric Dentistry: MSC - Bds. Belkays M. Omran AbubakrFafe ElNo ratings yet
- Rapid Sequence IntubationDocument58 pagesRapid Sequence IntubationArya VikneshNo ratings yet
- Conscious Sedation: Hayel Gharaibeh, MD. Anesthesia ConsultantDocument84 pagesConscious Sedation: Hayel Gharaibeh, MD. Anesthesia ConsultantKhaled GharaibehNo ratings yet
- Procedural AnesthesiaDocument40 pagesProcedural AnesthesiaJovian LutfiNo ratings yet
- Anesthesia and Analgesia: Far Eastern UniversityDocument59 pagesAnesthesia and Analgesia: Far Eastern UniversityAlexandra Duque-DavidNo ratings yet
- Day Care AnesthesiaDocument68 pagesDay Care AnesthesiaSri Sruthi PichikaNo ratings yet
- Conscious Sedation: Prof - Med. Nabil H. Mohyeddin Intensive Care &anesthesiologyDocument84 pagesConscious Sedation: Prof - Med. Nabil H. Mohyeddin Intensive Care &anesthesiologyKhaled GharaibehNo ratings yet
- Procedural Sedation and AnalgesiaDocument30 pagesProcedural Sedation and AnalgesiashoibyNo ratings yet
- Medical Emergencies in Dental OfficeDocument150 pagesMedical Emergencies in Dental OfficeSudeep DkNo ratings yet
- Advanced Emergency Airway ManagementDocument26 pagesAdvanced Emergency Airway ManagementcencenNo ratings yet
- PoisoningDocument97 pagesPoisoningmaruf47774No ratings yet
- Sedation and Analgesia in ICU (FJT) 2Document56 pagesSedation and Analgesia in ICU (FJT) 2Franz TariganNo ratings yet
- Pre-Medication and Anaesthesia in Dogs and Cats: Summary of Recommendations From 2009 Expert Round Table DiscussionDocument15 pagesPre-Medication and Anaesthesia in Dogs and Cats: Summary of Recommendations From 2009 Expert Round Table DiscussionEvaldo MamedesNo ratings yet
- Kanker Pelvis RenalisDocument12 pagesKanker Pelvis Renalissintadevi puspitsariNo ratings yet
- Drugs Affecting The Respiratory SystemDocument34 pagesDrugs Affecting The Respiratory SystemNeisha Halil VillarealNo ratings yet
- Postanesthesia Care: Muhamad Chairul FadhilDocument28 pagesPostanesthesia Care: Muhamad Chairul FadhilMuhammad Chairul Fadhil100% (1)
- Procedural AnesthesiaDocument40 pagesProcedural AnesthesiaHaris TanNo ratings yet
- Anesthesia For Cesarean SectionDocument60 pagesAnesthesia For Cesarean Sectionmaheralrwimi100% (1)
- Procedural AnesthesiaDocument40 pagesProcedural AnesthesiaJovian LutfiNo ratings yet
- Awake Craniotomy - MonchaiDocument50 pagesAwake Craniotomy - Monchaiอี๊ด โสภิต PizzyNo ratings yet
- Sedation and Analgesia in PicuDocument37 pagesSedation and Analgesia in PicubhoopendraNo ratings yet
- Epinephrine Classifications: Therapeutic: Antiasthmatics, Bronchodilators, Vasopressors Pharmacologic: Adrenergics IndicationsDocument14 pagesEpinephrine Classifications: Therapeutic: Antiasthmatics, Bronchodilators, Vasopressors Pharmacologic: Adrenergics IndicationsLindy Shane BoncalesNo ratings yet
- Pediatric AnesthesiaDocument70 pagesPediatric AnesthesiaAdel Taradji100% (1)
- Anesthesia in Pregnancy and ChildbirthDocument10 pagesAnesthesia in Pregnancy and ChildbirthNurul AiniNo ratings yet
- High Alert MedicationsDocument17 pagesHigh Alert MedicationsJoanna Marie Datahan EstomoNo ratings yet
- Understanding Breathlessness in 10'ish Minutes!Document25 pagesUnderstanding Breathlessness in 10'ish Minutes!ناصر كشلافNo ratings yet
- Analgesic & Anesthetic: Dr. Yunita Sari Pane, MsiDocument92 pagesAnalgesic & Anesthetic: Dr. Yunita Sari Pane, Msiqori fadillahNo ratings yet
- PharmacologyDocument27 pagesPharmacologyKyla CastroNo ratings yet
- Drugs Used in ObstertricsDocument58 pagesDrugs Used in ObstertricsDeborah AmpongNo ratings yet
- Exam 5 (Final Exam 23-25)Document19 pagesExam 5 (Final Exam 23-25)DoctorDrapionNo ratings yet
- Pharmacological Management of Child BehaviorDocument41 pagesPharmacological Management of Child BehaviorAsmaa RagabNo ratings yet
- Sedative and Myorelaxation Agents-03.04.20 PDFDocument25 pagesSedative and Myorelaxation Agents-03.04.20 PDFSarper Hikmet TAZENo ratings yet
- Meniere's Disease.Document30 pagesMeniere's Disease.June Yasa HacheroNo ratings yet
- Procedural Sedation in The ED: - Myths and MethodsDocument37 pagesProcedural Sedation in The ED: - Myths and MethodsSteven RossNo ratings yet
- Document DRUG 4Document4 pagesDocument DRUG 4Linda AdamsonNo ratings yet
- General AnasthesiaDocument131 pagesGeneral AnasthesiaRawan AlahehabNo ratings yet
- Management of Critically Ill Patients in The ICUDocument55 pagesManagement of Critically Ill Patients in The ICUkader abdiNo ratings yet
- Propofol 2Document22 pagesPropofol 2Bhaskar PendyalaNo ratings yet
- DruggggggDocument43 pagesDruggggggmonesabiancaNo ratings yet
- Medical Emergencies in OSDocument62 pagesMedical Emergencies in OSAditi RapriyaNo ratings yet
- EpilepsyDocument73 pagesEpilepsyabenezer g/kirstosNo ratings yet
- Regional Anaesthesia IN Paediatrics: Dr. P. Narasimha ReddyDocument83 pagesRegional Anaesthesia IN Paediatrics: Dr. P. Narasimha ReddydennyramdhanNo ratings yet
- Critical Care Nursing For ARDSDocument13 pagesCritical Care Nursing For ARDSanchemeysNo ratings yet
- Anesthesia For Day Care Dental ProceduresDocument20 pagesAnesthesia For Day Care Dental Proceduresramanrajesh83No ratings yet
- Emergency in DentistryDocument45 pagesEmergency in DentistryIyad Abou-RabiiNo ratings yet
- Indication Contra Sedation UpdatedDocument40 pagesIndication Contra Sedation UpdatedRegina SantosoNo ratings yet
- 2 Drugs For General AnaesthesiaDocument27 pages2 Drugs For General Anaesthesiaihtisham1No ratings yet
- Parenteral TherapyDocument18 pagesParenteral TherapyaloutolentinoNo ratings yet
- Child Management 3Document82 pagesChild Management 3j6r4qvkrkzNo ratings yet
- Awareness Under AnesthesiaDocument27 pagesAwareness Under AnesthesiaagatakassaNo ratings yet
- Differentiating Anesthesia Equipment: Identify and Understand Anesthesia Equipment in 1 Hour (Including the most popular manufacturers and suppliers to buy Anesthesia Equipment)From EverandDifferentiating Anesthesia Equipment: Identify and Understand Anesthesia Equipment in 1 Hour (Including the most popular manufacturers and suppliers to buy Anesthesia Equipment)No ratings yet
- Local Anesthesia Made Easy: Complete Guide on How to make your Local Anesthetic Procedure a Success (Including a List of Anesthetic Equipment and their Uses)From EverandLocal Anesthesia Made Easy: Complete Guide on How to make your Local Anesthetic Procedure a Success (Including a List of Anesthetic Equipment and their Uses)No ratings yet
- Paediatric SepsisDocument15 pagesPaediatric Sepsishailemichael chekolNo ratings yet
- Gyno... PTL & PRODocument30 pagesGyno... PTL & PROhailemichael chekolNo ratings yet
- 2 Paediatrics and Neonatal AnesthesiaDocument87 pages2 Paediatrics and Neonatal Anesthesiahailemichael chekolNo ratings yet
- 11-Reproductive SystemDocument56 pages11-Reproductive Systemhailemichael chekolNo ratings yet
- Oxytocin, Dinoprostone, Cefuroxime Drug StudyDocument3 pagesOxytocin, Dinoprostone, Cefuroxime Drug StudyMary Shane MoraldeNo ratings yet
- Drugs Acting On UterusDocument45 pagesDrugs Acting On UterusMohd ShoaibNo ratings yet
- Propofol Maintenance TIVA Infusions Kgs-Lbs 03-12-11 LockedDocument1 pagePropofol Maintenance TIVA Infusions Kgs-Lbs 03-12-11 LockedCasandra TudoracheNo ratings yet
- Daftar Stock Rutin TGL 23 Juni 2022Document22 pagesDaftar Stock Rutin TGL 23 Juni 2022Instalasi Farmasi RSUD HanauNo ratings yet
- Jaha 116 004909 PDFDocument8 pagesJaha 116 004909 PDFLisbeth MarbunNo ratings yet
- NovartisVsUnion LAB Team1 Pulkit Apoorva DebayudhDocument11 pagesNovartisVsUnion LAB Team1 Pulkit Apoorva DebayudhApoorva GoelNo ratings yet
- Pharmacy Practice ReportDocument22 pagesPharmacy Practice Report31.Rutuja KakadeNo ratings yet
- Pain andDocument18 pagesPain andShalem. KNo ratings yet
- Nose Drops FlyerDocument2 pagesNose Drops FlyermoniraNo ratings yet
- 2019-03-19 - MoH GSR 227 - New Drugs and Clinical Trial Approval Regulations 2019-147-264Document118 pages2019-03-19 - MoH GSR 227 - New Drugs and Clinical Trial Approval Regulations 2019-147-264go downNo ratings yet
- HyperlipidemiaDocument38 pagesHyperlipidemiaAadhan ArveeNo ratings yet
- Modifications in Drug Adherence After Switch To Fixed Dose Combination of Perindopril Amlodipine in Clinical Practice Results of A Large ScaleDocument8 pagesModifications in Drug Adherence After Switch To Fixed Dose Combination of Perindopril Amlodipine in Clinical Practice Results of A Large ScalenembutalNo ratings yet
- Membranous GlomerulopathyDocument376 pagesMembranous GlomerulopathylguerreroNo ratings yet
- List of TherapiesDocument3 pagesList of TherapiesAK KJNo ratings yet
- Handbook of Surgical Care For House OfficersDocument20 pagesHandbook of Surgical Care For House OfficersCharity AtsuNo ratings yet
- Revised BiopharmaceuticsDocument34 pagesRevised BiopharmaceuticsYuppie RajNo ratings yet
- Dams Crs - Psychiatry - DamsDocument250 pagesDams Crs - Psychiatry - DamsAbhisek Chatterjee100% (1)
- Numericals of ElectrochemistryDocument7 pagesNumericals of ElectrochemistryRudra Pratap SinghNo ratings yet
- HerbalDocument65 pagesHerbalShaz RizwanNo ratings yet
- Co AmoxiclavDocument7 pagesCo Amoxiclavbum817No ratings yet
- Botanicals For Mental Wellbeing Reference Sheet: NoticeDocument3 pagesBotanicals For Mental Wellbeing Reference Sheet: NoticelouisaNo ratings yet
- HIV Infection - Opportunistic InfectionsDocument21 pagesHIV Infection - Opportunistic InfectionszawadiNo ratings yet
- COVID-19 Cytokine Storm Syndrome: Identification and TreatmentDocument13 pagesCOVID-19 Cytokine Storm Syndrome: Identification and TreatmentIoana PelinNo ratings yet
- Dossier Structure enDocument29 pagesDossier Structure enKarim HefnyNo ratings yet
- Medicine in Drug Discovery: Anshuly Tiwari, Kakasaheb R. Mahadik, Satish Y. GabheDocument21 pagesMedicine in Drug Discovery: Anshuly Tiwari, Kakasaheb R. Mahadik, Satish Y. GabheSenda NovitaNo ratings yet
- ALERGI OBAT Prof. Dr. HardyantoDocument51 pagesALERGI OBAT Prof. Dr. HardyantoTimothy supitNo ratings yet
- TopicalsDocument1 pageTopicalsfaith2rescoberNo ratings yet
- Neutropenic Sepsis-Tls-Anaphylaxis-ExtravasationDocument40 pagesNeutropenic Sepsis-Tls-Anaphylaxis-ExtravasationSA NodeNo ratings yet