Download as pptx, pdf, or txt
You might also like
- Atls Questions and AnswersDocument14 pagesAtls Questions and AnswersAgil Rumboko Sumitro50% (6)
- NURS612 Exam 1 Review-Chen Walta - Week1-3Document15 pagesNURS612 Exam 1 Review-Chen Walta - Week1-3A Marie100% (1)
- Critical Decisions in Periodontology 4th Ed. 2003 - Hall (BC DECKER) PDFDocument378 pagesCritical Decisions in Periodontology 4th Ed. 2003 - Hall (BC DECKER) PDFkharida100% (1)
- Diseases and Peculiarities of The Negro Race - CartwrightDocument2 pagesDiseases and Peculiarities of The Negro Race - CartwrightReaganmonNo ratings yet
- Lecture 24 Part 1 - Nutritional Suppliment Part-1-2 PDFDocument25 pagesLecture 24 Part 1 - Nutritional Suppliment Part-1-2 PDFSYED ALI AHMED KAZMI TMANo ratings yet
- Lower Respi and TraumaDocument169 pagesLower Respi and TraumaTin tinNo ratings yet
- Woman With PneumoniaDocument9 pagesWoman With PneumoniaNohaira SADANGNo ratings yet
- Noninvasive Ventilation in Acute Respiratory Failure in AdultsDocument12 pagesNoninvasive Ventilation in Acute Respiratory Failure in AdultsferrevNo ratings yet
- Cell-Based Therapy To Reduce Mortality From COVID-19Document16 pagesCell-Based Therapy To Reduce Mortality From COVID-19Chelsea Shannen Marie CarreonNo ratings yet
- ARDSDocument27 pagesARDSChloie Marie RosalejosNo ratings yet
- ARDS Lecture Notes - StudentDocument4 pagesARDS Lecture Notes - StudentMary MarshNo ratings yet
- Bronchial AsthmaDocument34 pagesBronchial AsthmaFabb NelsonNo ratings yet
- Pulmonary Education Manual (PDFDrive)Document118 pagesPulmonary Education Manual (PDFDrive)Богдана ВацебаNo ratings yet
- Bronchitis in ChildrenDocument3 pagesBronchitis in ChildrenVibhaSingh1No ratings yet
- Ca Copd (Emphysema)Document42 pagesCa Copd (Emphysema)Charisse CaydanNo ratings yet
- Acute Dyspnea First RevisionDocument56 pagesAcute Dyspnea First RevisionAradhanaRamchandaniNo ratings yet
- Lung AbscessDocument30 pagesLung AbscessArmoured SpartanNo ratings yet
- COPD ExacerbationsDocument57 pagesCOPD ExacerbationsÁýáFáŕőúgNo ratings yet
- Respiratory DiseaseDocument27 pagesRespiratory Diseaseعبدالسلام الأسمرNo ratings yet
- 605 Nursing Care Plan 29-1: Patient With AsthmaDocument1 page605 Nursing Care Plan 29-1: Patient With AsthmaJonathonNo ratings yet
- Lung Abscess - Review - 2015Document13 pagesLung Abscess - Review - 2015Jonathan AiresNo ratings yet
- TVU Nursing Care PlanDocument19 pagesTVU Nursing Care Planjyoti singhNo ratings yet
- Occupational DZDocument102 pagesOccupational DZRamon MonchoNo ratings yet
- Immunology: QuestionsDocument41 pagesImmunology: Questionsgamelat Official100% (1)
- Việtnam s Sovereignty Over the Paracels Spratlys a History in DocumentsDocument579 pagesViệtnam s Sovereignty Over the Paracels Spratlys a History in DocumentsKhanh NguyenNo ratings yet
- Copd Omc Class - BB PDFDocument29 pagesCopd Omc Class - BB PDFafaq alismailiNo ratings yet
- Stridor & Stertor: by Dr. Baseem N. AbdulhadiDocument20 pagesStridor & Stertor: by Dr. Baseem N. AbdulhadiAli Abd AlrezaqNo ratings yet
- Ards 2Document7 pagesArds 2LUCIBELLOT1No ratings yet
- Typhoid FeverDocument15 pagesTyphoid FeverCherry Ann DomingoNo ratings yet
- Laringomalacia - Nursing CareDocument9 pagesLaringomalacia - Nursing CareRirin Muthia ZukhraNo ratings yet
- Berylliosis: IncurableDocument13 pagesBerylliosis: Incurablerahaf qatawnehNo ratings yet
- 2 Atrophic RhinitisDocument30 pages2 Atrophic RhinitissaleeNo ratings yet
- Hepatic EncephalopathyDocument65 pagesHepatic Encephalopathyvishal padwaleNo ratings yet
- Surviving Sepsis Campaign Guidelines 2021 Highlights For The Practicing ClinicianDocument8 pagesSurviving Sepsis Campaign Guidelines 2021 Highlights For The Practicing ClinicianMariah BrownNo ratings yet
- 2021 Lecture COPD & Asthma Full Size NotesDocument73 pages2021 Lecture COPD & Asthma Full Size NotesChelsea JiangNo ratings yet
- Bronchial AsthmaDocument20 pagesBronchial AsthmaJuliet De GuzmanNo ratings yet
- BRONCHIECTASISDocument36 pagesBRONCHIECTASISVince Peliño De MesaNo ratings yet
- Drug File SupriyaDocument36 pagesDrug File SupriyaSalim MinjNo ratings yet
- Lung Abscess: BackgroundDocument12 pagesLung Abscess: BackgroundTaufik TiasNo ratings yet
- Group Case Study - Pulmonary TBDocument8 pagesGroup Case Study - Pulmonary TBCj NiñalNo ratings yet
- Aulia Putri - Case SNNTDocument29 pagesAulia Putri - Case SNNTAulia P NurjannahNo ratings yet
- Bronchial AsthmaDocument45 pagesBronchial Asthmamuluken mulatieNo ratings yet
- COPDDocument15 pagesCOPDUmapreethi Kumar100% (1)
- Acute Respiratory Distress SyndromeDocument10 pagesAcute Respiratory Distress Syndromealina abu rumiNo ratings yet
- Infective EndocarditisDocument8 pagesInfective EndocarditisAiman Arifin100% (1)
- Oxygenation NCM 103Document10 pagesOxygenation NCM 103Richmond LacadenNo ratings yet
- Oxygen InsufficiencyDocument24 pagesOxygen InsufficiencyRatna VimalNo ratings yet
- 1.0 Upper Airway InfectionsDocument45 pages1.0 Upper Airway InfectionsMariahNo ratings yet
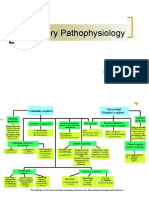
- Respiratory Pathophysiology: B. Pimentel, M.D. University of Makati College of NursingDocument12 pagesRespiratory Pathophysiology: B. Pimentel, M.D. University of Makati College of NursingDoc JacqueNo ratings yet
- Respiratory Failure (Aan) PDFDocument19 pagesRespiratory Failure (Aan) PDFYudionoNo ratings yet
- Acute Respiratory Distress SyndromDocument38 pagesAcute Respiratory Distress SyndrompatriaindraNo ratings yet
- Asthma Presentation by EkeneDocument52 pagesAsthma Presentation by Ekenegoldenmiebaka.mgNo ratings yet
- Respiratory Failure: Barry WardleDocument28 pagesRespiratory Failure: Barry Wardleapi-19826220No ratings yet
- TUBERCULOSISDocument9 pagesTUBERCULOSISAndra BauerNo ratings yet
- Hepatic Encephalopathy: DR Sadath HussainDocument32 pagesHepatic Encephalopathy: DR Sadath Hussain966342No ratings yet
- Pulmonary EdemaDocument50 pagesPulmonary EdemaStacy LuceroNo ratings yet
- Dengue FeverDocument8 pagesDengue FeverJay MagsaysayNo ratings yet
- The Effect of Obesity On Lung FunctionDocument25 pagesThe Effect of Obesity On Lung FunctionharvardboyNo ratings yet
- ARDSDocument55 pagesARDSSandhya HarbolaNo ratings yet
- RenalDocument62 pagesRenalDardarConstantinoNo ratings yet
- Viral Respiratory Diseases2Document21 pagesViral Respiratory Diseases2Paveethrah ChandranNo ratings yet
- Nippv Revisi Final Picu Nicu MaretDocument51 pagesNippv Revisi Final Picu Nicu MaretJulian Ammar Zaidan GunawanNo ratings yet
- Case Pres - PneumoniaDocument39 pagesCase Pres - Pneumoniafortunelobster100% (1)
- BronchiectasisDocument40 pagesBronchiectasisyana jaeNo ratings yet
- Franco ProfileDocument46 pagesFranco ProfileSumit SharmaNo ratings yet
- A Journal Report of Receipt of Mrna Covid-19 Vaccines and Risk of Spontaneous AbortionDocument11 pagesA Journal Report of Receipt of Mrna Covid-19 Vaccines and Risk of Spontaneous AbortionNica Joy DesquitadoNo ratings yet
- Relationship Between Endogenous Hydrogen Sulfide and Blood Stasis Syndrome Based On The Qi-Blood Theory of Chinese MedicineDocument6 pagesRelationship Between Endogenous Hydrogen Sulfide and Blood Stasis Syndrome Based On The Qi-Blood Theory of Chinese MedicineleonieNo ratings yet
- Placenta Previa Case Study: Adefuin, Jay Rovillos, Noemie MDocument40 pagesPlacenta Previa Case Study: Adefuin, Jay Rovillos, Noemie MMikes CastroNo ratings yet
- Antimicrobial Resistance Animal Production: Drivers, Dynamics and Epidemiology of INDocument68 pagesAntimicrobial Resistance Animal Production: Drivers, Dynamics and Epidemiology of INkrishna brahmbhattNo ratings yet
- Leaf Litter 3.1Document64 pagesLeaf Litter 3.1Drosera Capensis CapensisNo ratings yet
- STEMI GuidelinesDocument32 pagesSTEMI GuidelinesNurul FadhilahNo ratings yet
- Army Reserve Information BookletDocument32 pagesArmy Reserve Information Bookletyana33No ratings yet
- MSDS ExxonMobil PDFDocument12 pagesMSDS ExxonMobil PDFNurul MukhlisahNo ratings yet
- Structural Violence Essay FinalDocument6 pagesStructural Violence Essay FinalCharmaine NcubeNo ratings yet
- Amniodarone (Norvasc) Drug SummDocument1 pageAmniodarone (Norvasc) Drug SummWarrenNo ratings yet
- Biocredit Kores PDFDocument8 pagesBiocredit Kores PDFHeru SubrotoNo ratings yet
- Health Benefits of LycheeDocument24 pagesHealth Benefits of LycheeMD AbdullahNo ratings yet
- Cat Forklift Nr4500 36v Schematic Operation Maintenance ManualDocument27 pagesCat Forklift Nr4500 36v Schematic Operation Maintenance Manualfrankstewart270488qny100% (85)
- Neftali de La Cruz EmeterioDocument2 pagesNeftali de La Cruz EmeterioNeftali EmeterioNo ratings yet
- Harvard SchoolDocument24 pagesHarvard SchoolChariss Pacaldo ParungaoNo ratings yet
- Chapter #5 - Summary Abnormal Psychology: An Integrative Approach Chapter #5 - Summary Abnormal Psychology: An Integrative ApproachDocument13 pagesChapter #5 - Summary Abnormal Psychology: An Integrative Approach Chapter #5 - Summary Abnormal Psychology: An Integrative ApproachDjane VillarinNo ratings yet
- Radiology in ENTDocument56 pagesRadiology in ENTThomas Chapel100% (1)
- Soumya S Nair Biodata 4-07Document24 pagesSoumya S Nair Biodata 4-07ElizabethNo ratings yet
- ChemotherapyDocument253 pagesChemotherapyalmskein100% (1)
- BCM CPX Orientation 2016Document30 pagesBCM CPX Orientation 2016Chan ChanNo ratings yet
- 4 Brunnstrom ApproachDocument18 pages4 Brunnstrom ApproachHabibieNaufal ChannelNo ratings yet
- Trace Elements and Contaminants PDFDocument19 pagesTrace Elements and Contaminants PDFRahul Kumar MíšhřâNo ratings yet
- Multiple Sclerosis - A Review - EAN 2018Document14 pagesMultiple Sclerosis - A Review - EAN 2018Habib G. Moutran BarrosoNo ratings yet
- 10 1016@j Jiac 2017 02 014Document12 pages10 1016@j Jiac 2017 02 014Achmad YunusNo ratings yet
- Fungal Hyphae: Type # 1. Plectenchyma (Fig. 1.12)Document5 pagesFungal Hyphae: Type # 1. Plectenchyma (Fig. 1.12)vineetvishal73No ratings yet