Download as pptx, pdf, or txt
You might also like
- Protein Synthesis WorksheetDocument2 pagesProtein Synthesis WorksheetEderlyn Zate100% (1)
- Osmosis WSDocument2 pagesOsmosis WSSylva Sagita56% (9)
- Bio Factsheet: The Kidney: Excretion and OsmoregulationDocument4 pagesBio Factsheet: The Kidney: Excretion and OsmoregulationjesvinjesvinNo ratings yet
- Renal System AnatomyDocument7 pagesRenal System AnatomyAmbg GhalyNo ratings yet
- PHS RenalDocument44 pagesPHS Renaltewogbadeomobuwajo005No ratings yet
- Distal Convoluted Tubules, Counter Current Mechanism, MicturitionDocument94 pagesDistal Convoluted Tubules, Counter Current Mechanism, MicturitionSarah BirechNo ratings yet
- Renal Physiology BY Dr. Olasupo. S. AdeniyiDocument6 pagesRenal Physiology BY Dr. Olasupo. S. AdeniyiUloko ChristopherNo ratings yet
- L4 Regional Transport 2023Document4 pagesL4 Regional Transport 2023bgj9cddvxhNo ratings yet
- Distal Tubule Balance and Tubuloglomerular Feedback-Group 2Document42 pagesDistal Tubule Balance and Tubuloglomerular Feedback-Group 2Chuleha SethNo ratings yet
- Class11 Biology Unit19 NCERT TextBook EnglishEditionDocument12 pagesClass11 Biology Unit19 NCERT TextBook EnglishEditionUdit ChaudharyNo ratings yet
- Kidney Anatomy and PhysiologyDocument17 pagesKidney Anatomy and Physiologytemo chachanidzeNo ratings yet
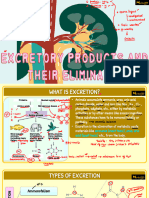
- Excretory Products and Their ElimnationDocument5 pagesExcretory Products and Their ElimnationSanskriti VermaNo ratings yet
- Tubular ReabsorptionDocument42 pagesTubular Reabsorptionmina mounirNo ratings yet
- Excretion IDocument27 pagesExcretion Ierinjoy77No ratings yet
- Excretory Organs in Different Organisms: Excretory Products and Their ElimnationDocument7 pagesExcretory Organs in Different Organisms: Excretory Products and Their ElimnationSreeyansu RajNo ratings yet
- Kidney NotesDocument5 pagesKidney Notesnad2samNo ratings yet
- 6-Drugs Acting On The Renal System - 2Document65 pages6-Drugs Acting On The Renal System - 2Hamid Hussain HamidNo ratings yet
- Reabsorption (Excretion Physiology)Document28 pagesReabsorption (Excretion Physiology)Ayesha IqbalNo ratings yet
- Kidney and OsmoregulationDocument25 pagesKidney and Osmoregulationsoyoung jinNo ratings yet
- Chapter-19 Excretory Products and Their Elimnation: Forms of Nitrogen ExcretionsDocument8 pagesChapter-19 Excretory Products and Their Elimnation: Forms of Nitrogen Excretionsmaryak3050No ratings yet
- Chapter 24. The Kidney.: 1. The Structure and Function of The NephronDocument8 pagesChapter 24. The Kidney.: 1. The Structure and Function of The NephronjeskevandiemenNo ratings yet
- Urine Formation - Human Excretory SystemDocument13 pagesUrine Formation - Human Excretory SystemRaj KumarNo ratings yet
- Excretory System 1Document51 pagesExcretory System 1Victoria TanNo ratings yet
- Excretory Products and EliminationDocument48 pagesExcretory Products and EliminationDivya AgarawalNo ratings yet
- APARATUL RenalDocument38 pagesAPARATUL RenalElena SosuNo ratings yet
- Unit 4: Excretion : Cbcs Third Sem GeneralDocument35 pagesUnit 4: Excretion : Cbcs Third Sem Generallegendhere121No ratings yet
- Renal PhysiologyDocument56 pagesRenal PhysiologyfinazkyaloNo ratings yet
- Role of The KIDNEYS in Homeostasis by D SiwaleDocument84 pagesRole of The KIDNEYS in Homeostasis by D Siwalenoahngoma41No ratings yet
- A Level Biology NotesDocument6 pagesA Level Biology NotesMira AluedeNo ratings yet
- Physio 2Document6 pagesPhysio 2Mohammad AlomariNo ratings yet
- Kidney Nephron Structure and FunctionDocument4 pagesKidney Nephron Structure and Functionxanxan4321No ratings yet
- M - 126 Structure of Nephron and Function of The Kidney PDFDocument4 pagesM - 126 Structure of Nephron and Function of The Kidney PDFDr. Tapan Kr. Dutta100% (1)
- Excretion in MammalsDocument17 pagesExcretion in MammalsKaynat JavedNo ratings yet
- Activity 36 - Urinary Tubular Reabsorption and SecretionDocument6 pagesActivity 36 - Urinary Tubular Reabsorption and SecretionKaren Joy MagbanuaNo ratings yet
- Urine Formation and Its CompositionDocument22 pagesUrine Formation and Its CompositionZahidKhanNo ratings yet
- Nephron 200328105815Document25 pagesNephron 200328105815Iph anyiNo ratings yet
- Untitled 1Document5 pagesUntitled 1YuliaAnggrainiNo ratings yet
- SHS.108.Lect-10 Tubular ReabsorptionDocument61 pagesSHS.108.Lect-10 Tubular ReabsorptionAzlan YasirNo ratings yet
- What Are AntibioticsDocument29 pagesWhat Are AntibioticsLouie BruanNo ratings yet
- 10.excretory SystemDocument16 pages10.excretory SystemLeena HassaninNo ratings yet
- +1 Kite Class 36 ExcretionDocument5 pages+1 Kite Class 36 Excretionsolamanmathew127No ratings yet
- Urinary Tract ReciewDocument5 pagesUrinary Tract ReciewRobert LotzerNo ratings yet
- Excretory Products and Its EliminationDocument2 pagesExcretory Products and Its Eliminationmariamfernandes6No ratings yet
- Excretory Products and Their EliminationDocument6 pagesExcretory Products and Their Eliminationkanth3012No ratings yet
- Blood Filtration and Nutrient and Water ReabsorptionDocument2 pagesBlood Filtration and Nutrient and Water ReabsorptionNadia SalwaniNo ratings yet
- Homeostasis NotesDocument5 pagesHomeostasis Notesaimee simarnoNo ratings yet
- Vipin Sir Biology 19. Excretory Products and Their EliminationDocument55 pagesVipin Sir Biology 19. Excretory Products and Their EliminationvanshpatelssisNo ratings yet
- 6 Renal PhysiologyDocument37 pages6 Renal PhysiologyD TekNo ratings yet
- Renal SystemDocument91 pagesRenal SystemKetheesaran LingamNo ratings yet
- Part 1 - US-Grade 4-BiochemistryDocument34 pagesPart 1 - US-Grade 4-BiochemistryFarah Bashar Al-RawachyNo ratings yet
- 11 Biology Notes ch19 Excretory Products and Their Elimination PDFDocument3 pages11 Biology Notes ch19 Excretory Products and Their Elimination PDFRamachandranPerumalNo ratings yet
- Drugs Affecting Renal FunctionDocument52 pagesDrugs Affecting Renal Functionliakot prantoNo ratings yet
- NephronDocument2 pagesNephronJohn SmithNo ratings yet
- The Collecting TubulesDocument1 pageThe Collecting TubulesMuhammad Naufal FadhillahNo ratings yet
- Ex Cert IonDocument11 pagesEx Cert IonVicky BhardwajNo ratings yet
- Topik 3Document29 pagesTopik 3AnnisNo ratings yet
- XQ WFHKLJW WWHAfu 0 DGWFDocument10 pagesXQ WFHKLJW WWHAfu 0 DGWFGiridharan & Balaji RNNo ratings yet
- Essential Anatomi and Physiologi of KidneyDocument36 pagesEssential Anatomi and Physiologi of KidneyБаттөр ОтгонбатNo ratings yet
- IM II - Fluids and Electrolytes (Lecture Trans)Document18 pagesIM II - Fluids and Electrolytes (Lecture Trans)Robert Francis DikioNo ratings yet
- UrinaryDocument87 pagesUrinaryJohn Paolo Dalida SalazarNo ratings yet
- Renal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledFrom EverandRenal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledNo ratings yet
- 296 2020 Article 4636Document12 pages296 2020 Article 4636thiago_eliseuNo ratings yet
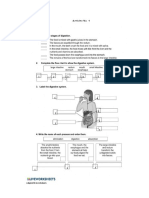
- Activity No. 1: Adapted LiveworksheetsDocument3 pagesActivity No. 1: Adapted LiveworksheetsBelinda I. IsugaNo ratings yet
- A-Level Biology Transport NotesDocument82 pagesA-Level Biology Transport NotesbirizimanabNo ratings yet
- L4-Effector Mechanisms of ImmunityDocument35 pagesL4-Effector Mechanisms of ImmunityFYMNo ratings yet
- M2-Post TaskDocument2 pagesM2-Post TaskmimiNo ratings yet
- ArticleDocument16 pagesArticleDanielNo ratings yet
- Digestion and Absorption of Lipids - MCQsDocument6 pagesDigestion and Absorption of Lipids - MCQswxyngtc4n9No ratings yet
- Cellphysiology 28129Document52 pagesCellphysiology 28129Rhed SedilloNo ratings yet
- Blood Anatomy and PhysiologyDocument28 pagesBlood Anatomy and PhysiologyPORTRAIT OF A NURSENo ratings yet
- UntitledDocument339 pagesUntitledJOS� FRANCISCO G�MEZ RODR�GUEZNo ratings yet
- Ascb Award Essay The Joy of A Career in Cell Biology: Zena WerbDocument3 pagesAscb Award Essay The Joy of A Career in Cell Biology: Zena Werbtosca206No ratings yet
- 5 SFB Bio Applications MRKDocument130 pages5 SFB Bio Applications MRKFatimaezzahra FaouziNo ratings yet
- Powerpoint To Accompany Concepts in Biology: Twelfth Edition Enger - Ross - BaileyDocument58 pagesPowerpoint To Accompany Concepts in Biology: Twelfth Edition Enger - Ross - Baileynishtha sahdevNo ratings yet
- Eabc6405 FullDocument12 pagesEabc6405 Fullvss2012No ratings yet
- Chapter 6 PhotosynthesisDocument18 pagesChapter 6 PhotosynthesisDaniel ChrysNo ratings yet
- IMMUNOLOGY AND SEROLOGY Exam Finalsb PDFDocument8 pagesIMMUNOLOGY AND SEROLOGY Exam Finalsb PDFMarcelino CalataNo ratings yet
- Biophysics-Lectures-2012-3 (Physiology) PDFDocument107 pagesBiophysics-Lectures-2012-3 (Physiology) PDFNedelcuGeorgeNo ratings yet
- Invited Review: Mechanisms of Normal and Tumor-Derived AngiogenesisDocument24 pagesInvited Review: Mechanisms of Normal and Tumor-Derived AngiogenesisDrMohit SharmaNo ratings yet
- (QUIZ) Animal Tissues 1Document1 page(QUIZ) Animal Tissues 1Karrel L. CollantesNo ratings yet
- Journal Pre-Proof: Cell Reports MedicineDocument39 pagesJournal Pre-Proof: Cell Reports MedicineErick RomeroNo ratings yet
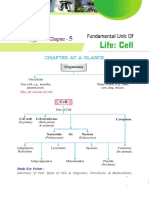
- Chapter at A Glance: Study Key PointsDocument14 pagesChapter at A Glance: Study Key PointssatishNo ratings yet
- Compare Mitosis and Meiosi1Document9 pagesCompare Mitosis and Meiosi1Reuben John AbalayanNo ratings yet
- General Biology 1 Second Quarter: LearningDocument4 pagesGeneral Biology 1 Second Quarter: Learningcheryl galletoNo ratings yet
- Ascorbic Acid-A Potential Oxidant Scavenger and Its Role in Plant Development and Abiotic Stress ToleranceDocument17 pagesAscorbic Acid-A Potential Oxidant Scavenger and Its Role in Plant Development and Abiotic Stress ToleranceNil Andreu ToseteNo ratings yet
- AIIMS Nov 2018 PDFDocument15 pagesAIIMS Nov 2018 PDFFatema AminNo ratings yet
- Clinical Pharmacology in PsychiatryDocument278 pagesClinical Pharmacology in Psychiatryanon_633561647No ratings yet
- Group 3 Prokaryotic Vs Eukaryotic Cells Activity Sheet ANSWER KEYDocument3 pagesGroup 3 Prokaryotic Vs Eukaryotic Cells Activity Sheet ANSWER KEYClaire Angelie RuayaNo ratings yet
- Inhibition of DNA Replication and TranscriptionDocument111 pagesInhibition of DNA Replication and TranscriptionPranav Kumar PrabhakarNo ratings yet