
Pasteurellaceae
Pasteurellaceae
You might also like
- Adult Infectious Diseases Over 200 Case Studies: Intended For: Medical Students, Ambulists, Hospitalists, Nurse Practitioners, Physician AssistantsFrom EverandAdult Infectious Diseases Over 200 Case Studies: Intended For: Medical Students, Ambulists, Hospitalists, Nurse Practitioners, Physician AssistantsRating: 4.5 out of 5 stars4.5/5 (7)
- Week 1 - Burton'S - LWW Introduction To MicrobiologyDocument21 pagesWeek 1 - Burton'S - LWW Introduction To MicrobiologyCathy Lago100% (1)
- Haemophilus and Other Fastidious Gram-Negative Bacilli General Characteristics Growth PatternsDocument14 pagesHaemophilus and Other Fastidious Gram-Negative Bacilli General Characteristics Growth PatternsAnna Charisa HernandezNo ratings yet
- Haemophilus and BordetellaDocument12 pagesHaemophilus and BordetellaDaiki AomineNo ratings yet
- Gram Negative CocciDocument21 pagesGram Negative CocciAyeshaNo ratings yet
- StreptococciDocument43 pagesStreptococciAyeshaNo ratings yet
- Kuliah Respi Bakteri TDK Lazim Revisi TambahanDocument23 pagesKuliah Respi Bakteri TDK Lazim Revisi TambahanIzza Ayudia HakimNo ratings yet
- Haemo Phil UsDocument11 pagesHaemo Phil UsDayana PrasanthNo ratings yet
- Lec No (4) - Viral Respiratory Tract InfectionsDocument60 pagesLec No (4) - Viral Respiratory Tract InfectionsMohammedu IhthishamNo ratings yet
- Diagnostic Testing For Community-Acquired Pneumonia (CAP) and InfluenzaDocument48 pagesDiagnostic Testing For Community-Acquired Pneumonia (CAP) and InfluenzaKartika RezkyNo ratings yet
- Fastidious Organisms: Brett Crawley MASM, MACTM, MAIMS Reference: Manual of Clinical Microbiology, 11 Ed. ASM PressDocument128 pagesFastidious Organisms: Brett Crawley MASM, MACTM, MAIMS Reference: Manual of Clinical Microbiology, 11 Ed. ASM Pressnur100% (1)
- Apicomplexa 2023Document39 pagesApicomplexa 2023Ming YanNo ratings yet
- Disclaimer: Christian Medical College Networked HospitalsDocument44 pagesDisclaimer: Christian Medical College Networked HospitalsJohn DorNo ratings yet
- It 38 Microbiology in Obgyn 24Document146 pagesIt 38 Microbiology in Obgyn 24dhjekwkwNo ratings yet
- SEPTICEMIA in Neonatal Period in FMCDocument40 pagesSEPTICEMIA in Neonatal Period in FMCIghodaro IsokenNo ratings yet
- BDS - Corynebacterium (Autosaved)Document35 pagesBDS - Corynebacterium (Autosaved)Just a PersonNo ratings yet
- DR Anil Sabharwal MDDocument57 pagesDR Anil Sabharwal MDsaump3No ratings yet
- ANAPLASMOSISDocument19 pagesANAPLASMOSISAshfaq Ahmad KhanNo ratings yet
- Family Spirochaetaceae AND LeptospiraceaeDocument33 pagesFamily Spirochaetaceae AND Leptospiraceaeyosef awokeNo ratings yet
- 2 PneumoniaDocument53 pages2 PneumoniaLucyellowOttemoesoeNo ratings yet
- Gram +/-Cocci: Thao Nguyen, PHD Thao - Nguyen@Ttu - Edu.VnDocument98 pagesGram +/-Cocci: Thao Nguyen, PHD Thao - Nguyen@Ttu - Edu.VnNguyen Phan TrongNo ratings yet
- Foundations in Microbiology: TalaroDocument71 pagesFoundations in Microbiology: Talaromertx013No ratings yet
- Fastidious Gram Negative RodsDocument74 pagesFastidious Gram Negative RodsMaria ClaraNo ratings yet
- Pharyngitis 0104 SlidesDocument144 pagesPharyngitis 0104 SlidesZammira MutiaNo ratings yet
- Microbial Diseases of The Cardiovascular and Lymphatic SystemsDocument27 pagesMicrobial Diseases of The Cardiovascular and Lymphatic SystemsAbhishek Isaac MathewNo ratings yet
- Micro Bio Disease ListDocument168 pagesMicro Bio Disease Listspiff spacemanNo ratings yet
- H.influenzae Modified 2012Document12 pagesH.influenzae Modified 2012MoonAIRNo ratings yet
- 3 Bacterial PneumoniaDocument30 pages3 Bacterial PneumoniaAP ShrivastavNo ratings yet
- Meningitis LectureDocument20 pagesMeningitis LectureIDIOVWA PRINCENo ratings yet
- MalariaDocument49 pagesMalaria2253010837No ratings yet
- VaccinationDocument64 pagesVaccinationnancymhd99No ratings yet
- Therapy 2 ch4Document74 pagesTherapy 2 ch4Emad MustafaNo ratings yet
- Pneumonia DR M ManiDocument69 pagesPneumonia DR M ManimaniNo ratings yet
- Malaria FalciparumDocument35 pagesMalaria FalciparumAboubakar Moalim Mahad moh'dNo ratings yet
- Foundations in Microbiology: The Cocci of Medical Importance TalaroDocument71 pagesFoundations in Microbiology: The Cocci of Medical Importance TalaroOdurNo ratings yet
- Practical Seminar1.13Document35 pagesPractical Seminar1.13chrisibinuNo ratings yet
- Yesinia and PasturellaDocument25 pagesYesinia and PasturellaThefatRatNo ratings yet
- Pediatric NotesDocument61 pagesPediatric NotesMatusala BafaNo ratings yet
- L - 2 - GR (-) CocciDocument82 pagesL - 2 - GR (-) CocciFahim NadvyNo ratings yet
- DiphtheriaDocument40 pagesDiphtheriaAP ShrivastavNo ratings yet
- MD PPTDocument105 pagesMD PPTtoxiczarrar.pubgNo ratings yet
- 13ffd1fa Eda0 4eb8 Bb3a 7802feec40daDocument40 pages13ffd1fa Eda0 4eb8 Bb3a 7802feec40daapi-26938624No ratings yet
- Respiratory Tract Infection 8Document66 pagesRespiratory Tract Infection 8JusticeNo ratings yet
- Aerobic Non-Spore Forming Gram-Positive BacilliDocument31 pagesAerobic Non-Spore Forming Gram-Positive BacilliCagar Irwin TaufanNo ratings yet
- Malaria PresentationDocument56 pagesMalaria PresentationMuhammad Shiddiq DwisuryaNo ratings yet
- Gram-Negative Rods Related To TheDocument28 pagesGram-Negative Rods Related To ThekebaridukeNo ratings yet
- Patologi Penyakit Infeksi: Willy Sandhika, Dr. M.Si. SP - PA Bagian Patologi Anatomi FK - Unair - SurabayaDocument38 pagesPatologi Penyakit Infeksi: Willy Sandhika, Dr. M.Si. SP - PA Bagian Patologi Anatomi FK - Unair - SurabayaArum Rasyiidta Windi SumbogoNo ratings yet
- Bacterial Infection On Upper Respiratory Tract Hemofillus Moraxella Fusobacterium Ed 1Document29 pagesBacterial Infection On Upper Respiratory Tract Hemofillus Moraxella Fusobacterium Ed 1Cintya Risti MawarniNo ratings yet
- Common Childhood Infections For CIDocument89 pagesCommon Childhood Infections For CIBeamlak Getachew WoldeselassieNo ratings yet
- 40 MalariaDocument68 pages40 MalariaShiv SharmaNo ratings yet
- Plasmodium Ovale: Phylum Subphylum Class Subclass Family Genes Species:Plasmodium OvaleDocument36 pagesPlasmodium Ovale: Phylum Subphylum Class Subclass Family Genes Species:Plasmodium OvaleAditya MuchayatsyahNo ratings yet
- Presentation 2Document18 pagesPresentation 2Shaafici MahamudNo ratings yet
- Malaria MB CHB January 2018-FinalDocument36 pagesMalaria MB CHB January 2018-Finalokwadha simionNo ratings yet
- Espiratory Infections BitseatDocument90 pagesEspiratory Infections BitseatAhmed KitawNo ratings yet
- Pneumonia: Martianus P, S.Farm.,M.Farm - Klin.,AptDocument30 pagesPneumonia: Martianus P, S.Farm.,M.Farm - Klin.,AptmadewikewirantiNo ratings yet
- 10 Anti InfectivesDocument29 pages10 Anti InfectivesFrançoise BNo ratings yet
- MeaslesDocument33 pagesMeaslesObi EmereuwaNo ratings yet
- Malaria: Charis Segeritz and Jo-Ann Osei-TwumDocument30 pagesMalaria: Charis Segeritz and Jo-Ann Osei-TwumzaheerbdsNo ratings yet
- ORTHOMYXOVIRUSES Inflenza Viruses A, B & CDocument16 pagesORTHOMYXOVIRUSES Inflenza Viruses A, B & CRandy BerryNo ratings yet
- Rhinoorbital MucormycosisDocument2 pagesRhinoorbital MucormycosisrgumralNo ratings yet
- Mucormycosis of The Hard Palate A Case ReportDocument3 pagesMucormycosis of The Hard Palate A Case ReportrgumralNo ratings yet
- 108 Orbitorhinocerebral MucormycosisDocument10 pages108 Orbitorhinocerebral MucormycosisrgumralNo ratings yet
- Epidemiology and Outcome ofDocument20 pagesEpidemiology and Outcome ofrgumralNo ratings yet
- 491 PDFDocument7 pages491 PDFrgumralNo ratings yet
- JBT 97Document6 pagesJBT 97rgumralNo ratings yet
- Vdocuments - MX - Intestinal Parasites Helminths Cestodes Protozoa Intestinal Parasites HelminthsDocument55 pagesVdocuments - MX - Intestinal Parasites Helminths Cestodes Protozoa Intestinal Parasites HelminthsrgumralNo ratings yet
- ParasitologyDocument31 pagesParasitologyrgumralNo ratings yet
- Bioorganic & Medicinal Chemistry Letters: Shaoyi Sun, Qi Jia, Zaihui Zhang TDocument16 pagesBioorganic & Medicinal Chemistry Letters: Shaoyi Sun, Qi Jia, Zaihui Zhang TjulianaNo ratings yet
- The Immune System and Lymphoid OrgansDocument68 pagesThe Immune System and Lymphoid OrgansAbraham Dawson machachaNo ratings yet
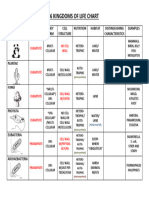
- 2017 6 KINGDOMS OF LIFE CHART AnswersDocument1 page2017 6 KINGDOMS OF LIFE CHART AnswersOliver ChantNo ratings yet
- Harmful Effect by MicroorganismsDocument2 pagesHarmful Effect by MicroorganismsKhairun NisaNo ratings yet
- Micros Very Small Bios Life Logos Study of : Introduction To Microbiology Microbiology "Micrographia" (Book)Document7 pagesMicros Very Small Bios Life Logos Study of : Introduction To Microbiology Microbiology "Micrographia" (Book)YayoNo ratings yet
- Manuscript-Ikmo LeavesDocument79 pagesManuscript-Ikmo LeavesQuebec GC RPhNo ratings yet
- Complement: Kathleen Basa Kris Nicole de Guzman Jessica Mae Ong 3HmtDocument70 pagesComplement: Kathleen Basa Kris Nicole de Guzman Jessica Mae Ong 3HmtCherry Reyes-Principe100% (1)
- Worksheet 1 (Before Lec 1) PDFDocument4 pagesWorksheet 1 (Before Lec 1) PDFLei Zaira BiendimaNo ratings yet
- Nejm 2016:374:562Document9 pagesNejm 2016:374:562Piya TangNo ratings yet
- Development of A QPCR Assay For Quantification of SaccharibacteriaDocument15 pagesDevelopment of A QPCR Assay For Quantification of SaccharibacteriaJLinNo ratings yet
- SULFOSALICYLIC ACID - Confirmatory Test For Urine Protein: PrincipleDocument5 pagesSULFOSALICYLIC ACID - Confirmatory Test For Urine Protein: Principlemezuniga1No ratings yet
- Pediatricobesity: Etiologyandtreatment: Melissa K. Crocker,, Jack A. YanovskiDocument24 pagesPediatricobesity: Etiologyandtreatment: Melissa K. Crocker,, Jack A. YanovskiAyline Araceli AlavaNo ratings yet
- Effect of Clarithromycin in Patients With Suspected Gram-Negative Sepsis: Results of A Randomized Controlled TrialDocument8 pagesEffect of Clarithromycin in Patients With Suspected Gram-Negative Sepsis: Results of A Randomized Controlled TrialH Yudi IriantoNo ratings yet
- Renin - Angiotensin System RAS Renin - Angiotensin-Aldosterone System RaasDocument3 pagesRenin - Angiotensin System RAS Renin - Angiotensin-Aldosterone System RaasReynaKatNo ratings yet
- Turkish Health Exam Basci-April 2016Document56 pagesTurkish Health Exam Basci-April 2016Ali Jama100% (2)
- Ent 25 ExamDocument8 pagesEnt 25 ExamAbd Alsalihi100% (1)
- FRACP Recall Paper 2002: Part A - 70 Questions, 2 HoursDocument43 pagesFRACP Recall Paper 2002: Part A - 70 Questions, 2 HoursZH. omg sarNo ratings yet
- D0685 Biology Paper2Document9 pagesD0685 Biology Paper2Aryan SinghNo ratings yet
- Next-Generation Vaccines: Nanoparticle-Mediated DNA and mRNA DeliveryDocument17 pagesNext-Generation Vaccines: Nanoparticle-Mediated DNA and mRNA DeliveryKaren BurgosNo ratings yet
- Global Covid Report PDFDocument73 pagesGlobal Covid Report PDFmunirjssipgkperlisgm100% (3)
- Methods of Classification and Identifying MicroorganismsDocument3 pagesMethods of Classification and Identifying MicroorganismsBecca TayNo ratings yet
- Pancreas: Anatomy & Physiology: Sanjay Munireddy Sinai Hospital 11/21/2006Document35 pagesPancreas: Anatomy & Physiology: Sanjay Munireddy Sinai Hospital 11/21/2006pedros43No ratings yet
- Airway Sensory Nerves in Asthma-Targets For TherapyDocument18 pagesAirway Sensory Nerves in Asthma-Targets For TherapySaraNo ratings yet
- Skenario IDocument12 pagesSkenario IRajasa FathahilllahNo ratings yet
- Annex 3: Recommendations To Assure The Quality, Safety and Efficacy of BCG VaccinesDocument50 pagesAnnex 3: Recommendations To Assure The Quality, Safety and Efficacy of BCG VaccinesDemo 1002No ratings yet
- Consumables RequiredDocument7 pagesConsumables RequiredSiva ShankarNo ratings yet
- Pharmacology AssignmentDocument3 pagesPharmacology AssignmentmorphimistNo ratings yet
- Catalog - SPC Alcohol Wipes 2020Document4 pagesCatalog - SPC Alcohol Wipes 2020aduan.ictzon8No ratings yet
- Lecture 2Document32 pagesLecture 2alizeh amanNo ratings yet
































































































Download as ppt, pdf, or txt
You might also like
- Adult Infectious Diseases Over 200 Case Studies: Intended For: Medical Students, Ambulists, Hospitalists, Nurse Practitioners, Physician AssistantsFrom EverandAdult Infectious Diseases Over 200 Case Studies: Intended For: Medical Students, Ambulists, Hospitalists, Nurse Practitioners, Physician AssistantsRating: 4.5 out of 5 stars4.5/5 (7)
- Week 1 - Burton'S - LWW Introduction To MicrobiologyDocument21 pagesWeek 1 - Burton'S - LWW Introduction To MicrobiologyCathy Lago100% (1)
- Haemophilus and Other Fastidious Gram-Negative Bacilli General Characteristics Growth PatternsDocument14 pagesHaemophilus and Other Fastidious Gram-Negative Bacilli General Characteristics Growth PatternsAnna Charisa HernandezNo ratings yet
- Haemophilus and BordetellaDocument12 pagesHaemophilus and BordetellaDaiki AomineNo ratings yet
- Gram Negative CocciDocument21 pagesGram Negative CocciAyeshaNo ratings yet
- StreptococciDocument43 pagesStreptococciAyeshaNo ratings yet
- Kuliah Respi Bakteri TDK Lazim Revisi TambahanDocument23 pagesKuliah Respi Bakteri TDK Lazim Revisi TambahanIzza Ayudia HakimNo ratings yet
- Haemo Phil UsDocument11 pagesHaemo Phil UsDayana PrasanthNo ratings yet
- Lec No (4) - Viral Respiratory Tract InfectionsDocument60 pagesLec No (4) - Viral Respiratory Tract InfectionsMohammedu IhthishamNo ratings yet
- Diagnostic Testing For Community-Acquired Pneumonia (CAP) and InfluenzaDocument48 pagesDiagnostic Testing For Community-Acquired Pneumonia (CAP) and InfluenzaKartika RezkyNo ratings yet
- Fastidious Organisms: Brett Crawley MASM, MACTM, MAIMS Reference: Manual of Clinical Microbiology, 11 Ed. ASM PressDocument128 pagesFastidious Organisms: Brett Crawley MASM, MACTM, MAIMS Reference: Manual of Clinical Microbiology, 11 Ed. ASM Pressnur100% (1)
- Apicomplexa 2023Document39 pagesApicomplexa 2023Ming YanNo ratings yet
- Disclaimer: Christian Medical College Networked HospitalsDocument44 pagesDisclaimer: Christian Medical College Networked HospitalsJohn DorNo ratings yet
- It 38 Microbiology in Obgyn 24Document146 pagesIt 38 Microbiology in Obgyn 24dhjekwkwNo ratings yet
- SEPTICEMIA in Neonatal Period in FMCDocument40 pagesSEPTICEMIA in Neonatal Period in FMCIghodaro IsokenNo ratings yet
- BDS - Corynebacterium (Autosaved)Document35 pagesBDS - Corynebacterium (Autosaved)Just a PersonNo ratings yet
- DR Anil Sabharwal MDDocument57 pagesDR Anil Sabharwal MDsaump3No ratings yet
- ANAPLASMOSISDocument19 pagesANAPLASMOSISAshfaq Ahmad KhanNo ratings yet
- Family Spirochaetaceae AND LeptospiraceaeDocument33 pagesFamily Spirochaetaceae AND Leptospiraceaeyosef awokeNo ratings yet
- 2 PneumoniaDocument53 pages2 PneumoniaLucyellowOttemoesoeNo ratings yet
- Gram +/-Cocci: Thao Nguyen, PHD Thao - Nguyen@Ttu - Edu.VnDocument98 pagesGram +/-Cocci: Thao Nguyen, PHD Thao - Nguyen@Ttu - Edu.VnNguyen Phan TrongNo ratings yet
- Foundations in Microbiology: TalaroDocument71 pagesFoundations in Microbiology: Talaromertx013No ratings yet
- Fastidious Gram Negative RodsDocument74 pagesFastidious Gram Negative RodsMaria ClaraNo ratings yet
- Pharyngitis 0104 SlidesDocument144 pagesPharyngitis 0104 SlidesZammira MutiaNo ratings yet
- Microbial Diseases of The Cardiovascular and Lymphatic SystemsDocument27 pagesMicrobial Diseases of The Cardiovascular and Lymphatic SystemsAbhishek Isaac MathewNo ratings yet
- Micro Bio Disease ListDocument168 pagesMicro Bio Disease Listspiff spacemanNo ratings yet
- H.influenzae Modified 2012Document12 pagesH.influenzae Modified 2012MoonAIRNo ratings yet
- 3 Bacterial PneumoniaDocument30 pages3 Bacterial PneumoniaAP ShrivastavNo ratings yet
- Meningitis LectureDocument20 pagesMeningitis LectureIDIOVWA PRINCENo ratings yet
- MalariaDocument49 pagesMalaria2253010837No ratings yet
- VaccinationDocument64 pagesVaccinationnancymhd99No ratings yet
- Therapy 2 ch4Document74 pagesTherapy 2 ch4Emad MustafaNo ratings yet
- Pneumonia DR M ManiDocument69 pagesPneumonia DR M ManimaniNo ratings yet
- Malaria FalciparumDocument35 pagesMalaria FalciparumAboubakar Moalim Mahad moh'dNo ratings yet
- Foundations in Microbiology: The Cocci of Medical Importance TalaroDocument71 pagesFoundations in Microbiology: The Cocci of Medical Importance TalaroOdurNo ratings yet
- Practical Seminar1.13Document35 pagesPractical Seminar1.13chrisibinuNo ratings yet
- Yesinia and PasturellaDocument25 pagesYesinia and PasturellaThefatRatNo ratings yet
- Pediatric NotesDocument61 pagesPediatric NotesMatusala BafaNo ratings yet
- L - 2 - GR (-) CocciDocument82 pagesL - 2 - GR (-) CocciFahim NadvyNo ratings yet
- DiphtheriaDocument40 pagesDiphtheriaAP ShrivastavNo ratings yet
- MD PPTDocument105 pagesMD PPTtoxiczarrar.pubgNo ratings yet
- 13ffd1fa Eda0 4eb8 Bb3a 7802feec40daDocument40 pages13ffd1fa Eda0 4eb8 Bb3a 7802feec40daapi-26938624No ratings yet
- Respiratory Tract Infection 8Document66 pagesRespiratory Tract Infection 8JusticeNo ratings yet
- Aerobic Non-Spore Forming Gram-Positive BacilliDocument31 pagesAerobic Non-Spore Forming Gram-Positive BacilliCagar Irwin TaufanNo ratings yet
- Malaria PresentationDocument56 pagesMalaria PresentationMuhammad Shiddiq DwisuryaNo ratings yet
- Gram-Negative Rods Related To TheDocument28 pagesGram-Negative Rods Related To ThekebaridukeNo ratings yet
- Patologi Penyakit Infeksi: Willy Sandhika, Dr. M.Si. SP - PA Bagian Patologi Anatomi FK - Unair - SurabayaDocument38 pagesPatologi Penyakit Infeksi: Willy Sandhika, Dr. M.Si. SP - PA Bagian Patologi Anatomi FK - Unair - SurabayaArum Rasyiidta Windi SumbogoNo ratings yet
- Bacterial Infection On Upper Respiratory Tract Hemofillus Moraxella Fusobacterium Ed 1Document29 pagesBacterial Infection On Upper Respiratory Tract Hemofillus Moraxella Fusobacterium Ed 1Cintya Risti MawarniNo ratings yet
- Common Childhood Infections For CIDocument89 pagesCommon Childhood Infections For CIBeamlak Getachew WoldeselassieNo ratings yet
- 40 MalariaDocument68 pages40 MalariaShiv SharmaNo ratings yet
- Plasmodium Ovale: Phylum Subphylum Class Subclass Family Genes Species:Plasmodium OvaleDocument36 pagesPlasmodium Ovale: Phylum Subphylum Class Subclass Family Genes Species:Plasmodium OvaleAditya MuchayatsyahNo ratings yet
- Presentation 2Document18 pagesPresentation 2Shaafici MahamudNo ratings yet
- Malaria MB CHB January 2018-FinalDocument36 pagesMalaria MB CHB January 2018-Finalokwadha simionNo ratings yet
- Espiratory Infections BitseatDocument90 pagesEspiratory Infections BitseatAhmed KitawNo ratings yet
- Pneumonia: Martianus P, S.Farm.,M.Farm - Klin.,AptDocument30 pagesPneumonia: Martianus P, S.Farm.,M.Farm - Klin.,AptmadewikewirantiNo ratings yet
- 10 Anti InfectivesDocument29 pages10 Anti InfectivesFrançoise BNo ratings yet
- MeaslesDocument33 pagesMeaslesObi EmereuwaNo ratings yet
- Malaria: Charis Segeritz and Jo-Ann Osei-TwumDocument30 pagesMalaria: Charis Segeritz and Jo-Ann Osei-TwumzaheerbdsNo ratings yet
- ORTHOMYXOVIRUSES Inflenza Viruses A, B & CDocument16 pagesORTHOMYXOVIRUSES Inflenza Viruses A, B & CRandy BerryNo ratings yet
- Rhinoorbital MucormycosisDocument2 pagesRhinoorbital MucormycosisrgumralNo ratings yet
- Mucormycosis of The Hard Palate A Case ReportDocument3 pagesMucormycosis of The Hard Palate A Case ReportrgumralNo ratings yet
- 108 Orbitorhinocerebral MucormycosisDocument10 pages108 Orbitorhinocerebral MucormycosisrgumralNo ratings yet
- Epidemiology and Outcome ofDocument20 pagesEpidemiology and Outcome ofrgumralNo ratings yet
- 491 PDFDocument7 pages491 PDFrgumralNo ratings yet
- JBT 97Document6 pagesJBT 97rgumralNo ratings yet
- Vdocuments - MX - Intestinal Parasites Helminths Cestodes Protozoa Intestinal Parasites HelminthsDocument55 pagesVdocuments - MX - Intestinal Parasites Helminths Cestodes Protozoa Intestinal Parasites HelminthsrgumralNo ratings yet
- ParasitologyDocument31 pagesParasitologyrgumralNo ratings yet
- Bioorganic & Medicinal Chemistry Letters: Shaoyi Sun, Qi Jia, Zaihui Zhang TDocument16 pagesBioorganic & Medicinal Chemistry Letters: Shaoyi Sun, Qi Jia, Zaihui Zhang TjulianaNo ratings yet
- The Immune System and Lymphoid OrgansDocument68 pagesThe Immune System and Lymphoid OrgansAbraham Dawson machachaNo ratings yet
- 2017 6 KINGDOMS OF LIFE CHART AnswersDocument1 page2017 6 KINGDOMS OF LIFE CHART AnswersOliver ChantNo ratings yet
- Harmful Effect by MicroorganismsDocument2 pagesHarmful Effect by MicroorganismsKhairun NisaNo ratings yet
- Micros Very Small Bios Life Logos Study of : Introduction To Microbiology Microbiology "Micrographia" (Book)Document7 pagesMicros Very Small Bios Life Logos Study of : Introduction To Microbiology Microbiology "Micrographia" (Book)YayoNo ratings yet
- Manuscript-Ikmo LeavesDocument79 pagesManuscript-Ikmo LeavesQuebec GC RPhNo ratings yet
- Complement: Kathleen Basa Kris Nicole de Guzman Jessica Mae Ong 3HmtDocument70 pagesComplement: Kathleen Basa Kris Nicole de Guzman Jessica Mae Ong 3HmtCherry Reyes-Principe100% (1)
- Worksheet 1 (Before Lec 1) PDFDocument4 pagesWorksheet 1 (Before Lec 1) PDFLei Zaira BiendimaNo ratings yet
- Nejm 2016:374:562Document9 pagesNejm 2016:374:562Piya TangNo ratings yet
- Development of A QPCR Assay For Quantification of SaccharibacteriaDocument15 pagesDevelopment of A QPCR Assay For Quantification of SaccharibacteriaJLinNo ratings yet
- SULFOSALICYLIC ACID - Confirmatory Test For Urine Protein: PrincipleDocument5 pagesSULFOSALICYLIC ACID - Confirmatory Test For Urine Protein: Principlemezuniga1No ratings yet
- Pediatricobesity: Etiologyandtreatment: Melissa K. Crocker,, Jack A. YanovskiDocument24 pagesPediatricobesity: Etiologyandtreatment: Melissa K. Crocker,, Jack A. YanovskiAyline Araceli AlavaNo ratings yet
- Effect of Clarithromycin in Patients With Suspected Gram-Negative Sepsis: Results of A Randomized Controlled TrialDocument8 pagesEffect of Clarithromycin in Patients With Suspected Gram-Negative Sepsis: Results of A Randomized Controlled TrialH Yudi IriantoNo ratings yet
- Renin - Angiotensin System RAS Renin - Angiotensin-Aldosterone System RaasDocument3 pagesRenin - Angiotensin System RAS Renin - Angiotensin-Aldosterone System RaasReynaKatNo ratings yet
- Turkish Health Exam Basci-April 2016Document56 pagesTurkish Health Exam Basci-April 2016Ali Jama100% (2)
- Ent 25 ExamDocument8 pagesEnt 25 ExamAbd Alsalihi100% (1)
- FRACP Recall Paper 2002: Part A - 70 Questions, 2 HoursDocument43 pagesFRACP Recall Paper 2002: Part A - 70 Questions, 2 HoursZH. omg sarNo ratings yet
- D0685 Biology Paper2Document9 pagesD0685 Biology Paper2Aryan SinghNo ratings yet
- Next-Generation Vaccines: Nanoparticle-Mediated DNA and mRNA DeliveryDocument17 pagesNext-Generation Vaccines: Nanoparticle-Mediated DNA and mRNA DeliveryKaren BurgosNo ratings yet
- Global Covid Report PDFDocument73 pagesGlobal Covid Report PDFmunirjssipgkperlisgm100% (3)
- Methods of Classification and Identifying MicroorganismsDocument3 pagesMethods of Classification and Identifying MicroorganismsBecca TayNo ratings yet
- Pancreas: Anatomy & Physiology: Sanjay Munireddy Sinai Hospital 11/21/2006Document35 pagesPancreas: Anatomy & Physiology: Sanjay Munireddy Sinai Hospital 11/21/2006pedros43No ratings yet
- Airway Sensory Nerves in Asthma-Targets For TherapyDocument18 pagesAirway Sensory Nerves in Asthma-Targets For TherapySaraNo ratings yet
- Skenario IDocument12 pagesSkenario IRajasa FathahilllahNo ratings yet
- Annex 3: Recommendations To Assure The Quality, Safety and Efficacy of BCG VaccinesDocument50 pagesAnnex 3: Recommendations To Assure The Quality, Safety and Efficacy of BCG VaccinesDemo 1002No ratings yet
- Consumables RequiredDocument7 pagesConsumables RequiredSiva ShankarNo ratings yet
- Pharmacology AssignmentDocument3 pagesPharmacology AssignmentmorphimistNo ratings yet
- Catalog - SPC Alcohol Wipes 2020Document4 pagesCatalog - SPC Alcohol Wipes 2020aduan.ictzon8No ratings yet
- Lecture 2Document32 pagesLecture 2alizeh amanNo ratings yet