Download as pptx, pdf, or txt
You might also like
- Christine Piper - After Darkness (Extract)Document34 pagesChristine Piper - After Darkness (Extract)Allen & Unwin100% (3)
- Comunicaciones Digitales Avanzadas DEBER 1 (Select Max. 10 Problems and Answer The Two Questions)Document3 pagesComunicaciones Digitales Avanzadas DEBER 1 (Select Max. 10 Problems and Answer The Two Questions)Cristian Sancho LopezNo ratings yet
- UTI BrochureDocument2 pagesUTI BrochureKaye de LeonNo ratings yet
- Pleural Effusion 31.10.14Document25 pagesPleural Effusion 31.10.14Dr. AHBAB HUSSAINNo ratings yet
- Differential Diagnosis of Pleural Effusion-82892Document56 pagesDifferential Diagnosis of Pleural Effusion-82892Salih AslaNo ratings yet
- Pleura Effusion Bahan Kuliah PakarDocument27 pagesPleura Effusion Bahan Kuliah PakarAfifah NaurahNo ratings yet
- Pleural EffusionDocument24 pagesPleural Effusionalyas alyasNo ratings yet
- Approach To Pleural Diseases2Document153 pagesApproach To Pleural Diseases2Shanza AmaanNo ratings yet
- Pleural Effusion: Hassan Ahmad - Roll Number 381 Final Year MBBS Rawalpindi Medical UniversityDocument30 pagesPleural Effusion: Hassan Ahmad - Roll Number 381 Final Year MBBS Rawalpindi Medical UniversityHassan AhmadNo ratings yet
- Pleura Effusion Bahan Kuliah PakarDocument27 pagesPleura Effusion Bahan Kuliah PakarRudy LusmiandaNo ratings yet
- Disease of PleuraDocument25 pagesDisease of PleuragodzahadesNo ratings yet
- Pleural EffusionDocument72 pagesPleural Effusionmaeliszxc kimNo ratings yet
- Pleural Effusion 23-24Document21 pagesPleural Effusion 23-24bazyan3aNo ratings yet
- Cleveland Clinic Journal of Medicine 2005Document12 pagesCleveland Clinic Journal of Medicine 2005melianasulistioNo ratings yet
- Diseases - of - PleuraDocument110 pagesDiseases - of - PleuraMohamed HefnyNo ratings yet
- Name: Abdirahman Sheikh Abdillahi Farah Faculty: Clinical Officers (CO8) Course: Pediatric Lecturer: DR Amin Assingment: Pleural EffusionDocument46 pagesName: Abdirahman Sheikh Abdillahi Farah Faculty: Clinical Officers (CO8) Course: Pediatric Lecturer: DR Amin Assingment: Pleural EffusionAbdirahman Abdillahi FarahNo ratings yet
- Efusi Pleura & EmpyemaDocument47 pagesEfusi Pleura & EmpyemaArumLaksmitaDewiNo ratings yet
- Definition:: Pleural EffusionDocument4 pagesDefinition:: Pleural EffusionGetom NgukirNo ratings yet
- Pleural EffusionDocument25 pagesPleural EffusionRachanaNo ratings yet
- Efusi PleuraDocument26 pagesEfusi PleuraAhmad Isyai RamadhanNo ratings yet
- Pleural EffusionsDocument41 pagesPleural Effusionssanjivdas100% (1)
- Srishti Gupta - 304 - Day 15Document3 pagesSrishti Gupta - 304 - Day 15Srishti Gupta - 304No ratings yet
- Oncology - Presentation EditedDocument71 pagesOncology - Presentation EditedSarah Racheal AkelloNo ratings yet
- Pleural DiseasesDocument64 pagesPleural DiseasesDONALD UNASHENo ratings yet
- Pleural Effusion2Document42 pagesPleural Effusion2malaiya_anuragNo ratings yet
- Pleural Effusion Med StudentsDocument37 pagesPleural Effusion Med StudentsnickNo ratings yet
- Pleural EffDocument30 pagesPleural EffAlexander Santiago ParelNo ratings yet
- PleuraDocument38 pagesPleuraMuhammad UmarNo ratings yet
- Body Fluids1Document93 pagesBody Fluids1Aliyah Tofani PawelloiNo ratings yet
- The Radiology of PleuraDocument122 pagesThe Radiology of PleuraAimandu ShresthaNo ratings yet
- Pleural Effusion: Dr.S.Sesha Sai (MD), Pulmonary MedicineDocument52 pagesPleural Effusion: Dr.S.Sesha Sai (MD), Pulmonary MedicinevaishnaviNo ratings yet
- HemoperitoneumDocument36 pagesHemoperitoneumnovitafitri123No ratings yet
- ThoracentesisDocument21 pagesThoracentesisAmna BatoolNo ratings yet
- Pleural EffusionDocument13 pagesPleural EffusionAbdirahman Ali YabarNo ratings yet
- Pleural EffusionDocument51 pagesPleural EffusionMinhajul IslamNo ratings yet
- Approach To Pleura LeffusionDocument91 pagesApproach To Pleura Leffusionrodie1050% (1)
- Pleural EffusionDocument8 pagesPleural Effusionrahtu suzi ameliaNo ratings yet
- Transudate: Pneumonia Mesothelioma Rheumatoid ArthritsDocument3 pagesTransudate: Pneumonia Mesothelioma Rheumatoid ArthritsAbdurrahman HakemNo ratings yet
- RadiologyDocument46 pagesRadiologyitho23100% (1)
- Pleuraleffusion 160424141916Document20 pagesPleuraleffusion 160424141916Jessa Adenig100% (1)
- Radiology Pointers Part 1Document6 pagesRadiology Pointers Part 1Tutor VirusNo ratings yet
- HematothoraxDocument15 pagesHematothoraxmail junkNo ratings yet
- Nursing Care of Patients With Pneumothorax: Prepared By: N. WadeDocument33 pagesNursing Care of Patients With Pneumothorax: Prepared By: N. WadeokaciaNo ratings yet
- Pulmonary Embolus (PE)Document3 pagesPulmonary Embolus (PE)Heidi M FischerNo ratings yet
- Pledisuraealse - 30 Oktober 2012Document57 pagesPledisuraealse - 30 Oktober 2012Silvestri PurbaNo ratings yet
- 288 Disorders of PleuraDocument3 pages288 Disorders of Pleuradeepak_anvekarNo ratings yet
- Pleural Effusion: Aarya PR Bds 3 YearDocument22 pagesPleural Effusion: Aarya PR Bds 3 YearThahseen TwzNo ratings yet
- Malignant Pleural EffusionsDocument52 pagesMalignant Pleural EffusionsKai XinNo ratings yet
- 2022 Pleural EffusionDocument36 pages2022 Pleural EffusionYasser KamalNo ratings yet
- Pleural Effusion: Putu AndrikaDocument32 pagesPleural Effusion: Putu Andrikadr.Dewi ShintaherNo ratings yet
- Teknik Operasi Pericardial Window LiusDocument23 pagesTeknik Operasi Pericardial Window LiusDeddy Guu100% (1)
- Pleura Pleural Effusions: o o o o o o o o o o o o oDocument5 pagesPleura Pleural Effusions: o o o o o o o o o o o o oangga nugrahaNo ratings yet
- Pleural EffusionsDocument79 pagesPleural EffusionsDiana_anca6No ratings yet
- Venous ThromboembolismDocument80 pagesVenous Thromboembolismtcj4bpj2pnNo ratings yet
- Massive Pleural EffusionDocument21 pagesMassive Pleural EffusionImam Mohammed ImamNo ratings yet
- Injuries To Genitourinary TractDocument130 pagesInjuries To Genitourinary TractYUFFANo ratings yet
- Imaging in Abdominal Trauma: S ThiyagarajanDocument133 pagesImaging in Abdominal Trauma: S ThiyagarajanEdward Arthur IskandarNo ratings yet
- Pleural Effusion: AetiologyDocument5 pagesPleural Effusion: AetiologyKingman844No ratings yet
- DR M Abdur Rahim M.D.:, Asst. Professor of MedicineDocument43 pagesDR M Abdur Rahim M.D.:, Asst. Professor of Medicinedr_abdurNo ratings yet
- Gi Bleed RadiologyDocument60 pagesGi Bleed RadiologyDINESHNo ratings yet
- A Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisFrom EverandA Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisRating: 3 out of 5 stars3/5 (1)
- Chain of InfectionDocument8 pagesChain of Infectionkim mimiNo ratings yet
- (DPR1000) Modbus Map Tech Data en 201909Document2 pages(DPR1000) Modbus Map Tech Data en 201909Duẩn Nguyễn VănNo ratings yet
- Method 207 Ammonia in Air EmissionDocument49 pagesMethod 207 Ammonia in Air Emissionsalma ghaniNo ratings yet
- Lesson Plan 2 WeeblyDocument5 pagesLesson Plan 2 Weeblyapi-176731501No ratings yet
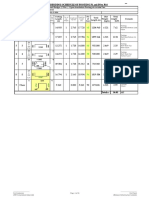
- BBS of All Pier Foundations of MAYARDocument16 pagesBBS of All Pier Foundations of MAYARAmanjot Singh0% (1)
- MQB 09 WS 2Document4 pagesMQB 09 WS 2Nasmer BembiNo ratings yet
- Gma1!2!2015 ContinutDocument64 pagesGma1!2!2015 ContinutSon HoangNo ratings yet
- Readers Theater For Grade OneDocument9 pagesReaders Theater For Grade OneglaidzNo ratings yet
- ALS 204 LH (Top Labelling)Document2 pagesALS 204 LH (Top Labelling)Yashvanth ShettyNo ratings yet
- World's TallestDocument6 pagesWorld's TallestMaryNo ratings yet
- ContentDocument16 pagesContenttootlajosNo ratings yet
- Best Control For FliesDocument30 pagesBest Control For FliesDavidNo ratings yet
- Ir. H. Isnugroho, CES: Faculty of Engineering Civil Engineering Program Study Muhammadiyah University of SurakartaDocument21 pagesIr. H. Isnugroho, CES: Faculty of Engineering Civil Engineering Program Study Muhammadiyah University of SurakartaRhezader AgNo ratings yet
- 5 - NLM Practice Assignment @JEEAdvanced - 2024Document5 pages5 - NLM Practice Assignment @JEEAdvanced - 2024Vineet SierraNo ratings yet
- Quanta G31a Dag31amb6d0 Y61x-6l Rev 1aDocument49 pagesQuanta G31a Dag31amb6d0 Y61x-6l Rev 1aKrystian PalaciosNo ratings yet
- Lesson Plann Highschool FullDocument3 pagesLesson Plann Highschool Fullapi-329957578No ratings yet
- LAB14Document5 pagesLAB14Aizaz HabibNo ratings yet
- Entropy: New Insights Into The Fractional Order Diffusion Equation Using Entropy and KurtosisDocument15 pagesEntropy: New Insights Into The Fractional Order Diffusion Equation Using Entropy and KurtosisBibin FrancisNo ratings yet
- Bridge Abutment DesignDocument14 pagesBridge Abutment Designsharangill100% (1)
- Assignment 1 Art HistoryDocument4 pagesAssignment 1 Art HistoryFarhanNo ratings yet
- A Narrative Report On Informing The Barangay 1 and Barangay 9Document3 pagesA Narrative Report On Informing The Barangay 1 and Barangay 9Heugh Gerard Rizo33% (3)
- CSJ HydraulicDocument43 pagesCSJ HydraulicВаня БойкоNo ratings yet
- Keratin TreatmentDocument2 pagesKeratin TreatmentDilinika PriyadarshaniNo ratings yet
- A Study On Customer Satisfaction of Honda Activa In: ChennaiDocument65 pagesA Study On Customer Satisfaction of Honda Activa In: ChennaiSampath Bengalooru HudugaNo ratings yet
- Sohbi Kohgei - Solar Power System Proposal (Toshiba325W)Document4 pagesSohbi Kohgei - Solar Power System Proposal (Toshiba325W)Jeffcaster ComelNo ratings yet
- UntitledDocument45 pagesUntitledaina ainaNo ratings yet
- DMSCO Log Book Vol.8 6/1930-5/1931Document49 pagesDMSCO Log Book Vol.8 6/1930-5/1931Des Moines University Archives and Rare Book RoomNo ratings yet