Download as pptx, pdf, or txt
You might also like
- 429 History Taking and Physical Examination Booklet 2nd Edition 2013Document152 pages429 History Taking and Physical Examination Booklet 2nd Edition 2013Aloah122346100% (2)
- топик a visit to a dentistDocument2 pagesтопик a visit to a dentistEyeless DanteJackNo ratings yet
- The Surgical PatientDocument20 pagesThe Surgical PatientMikel MMarshallNo ratings yet
- Physical ExaminationDocument39 pagesPhysical ExaminationMutegeki AdolfNo ratings yet
- From Clinical Observations To Research: Dr. Dick Menzies June 10, 2005Document36 pagesFrom Clinical Observations To Research: Dr. Dick Menzies June 10, 2005Santi PadmasariNo ratings yet
- OSCE Final 1 PDFDocument204 pagesOSCE Final 1 PDFamalNo ratings yet
- E.N.T Guide For Medical Students: Neck Examination: Dr. Giovanni Henry ENT Resident 2016Document79 pagesE.N.T Guide For Medical Students: Neck Examination: Dr. Giovanni Henry ENT Resident 2016John M. HemsworthNo ratings yet
- SURGICAL TALK FinalpptDocument30 pagesSURGICAL TALK FinalpptRazeen RiyasatNo ratings yet
- Case History1Document38 pagesCase History1kali natiNo ratings yet
- Examination of The Head Neck 2018Document77 pagesExamination of The Head Neck 2018hayafalqasemiNo ratings yet
- 第一次课history-taking - 瞿立辉 2.29Document88 pages第一次课history-taking - 瞿立辉 2.29Mar ClrNo ratings yet
- Health Screening and Hereditary Diseases - v2Document57 pagesHealth Screening and Hereditary Diseases - v2Alice LowNo ratings yet
- 2023 Introduction To Physical DiagnosisDocument37 pages2023 Introduction To Physical DiagnosisNejibMohe Abagisa100% (1)
- OSCE S BibleDocument66 pagesOSCE S BibleApoorva SaxenaNo ratings yet
- General Principles of Gastroentorylogy.Document32 pagesGeneral Principles of Gastroentorylogy.hirsi200518No ratings yet
- 3rd Year Introduction NOTESDocument21 pages3rd Year Introduction NOTESalexandermason2003No ratings yet
- Clinical ReasoningDocument60 pagesClinical ReasoningFrances DeiNo ratings yet
- ASSESSMENTDocument52 pagesASSESSMENTPaul walkerNo ratings yet
- OSCEDocument58 pagesOSCEAbubakar JallohNo ratings yet
- CommunicationConsultation Skills and Data GatheringDocument18 pagesCommunicationConsultation Skills and Data GatheringLamyaa Ali Hasan100% (1)
- Epidemiology: Chapter 1: IntroductionDocument134 pagesEpidemiology: Chapter 1: IntroductionLoai Mohammed IssaNo ratings yet
- Epidemiology: Chapter 1: IntroductionDocument134 pagesEpidemiology: Chapter 1: IntroductionLoai Mohammed IssaNo ratings yet
- Internship Manual For MBBSDocument29 pagesInternship Manual For MBBSKoustav ChakrabortyNo ratings yet
- History Taking For C-1Document48 pagesHistory Taking For C-1Merahit AberaNo ratings yet
- Systemic Lupus ErythematosusDocument25 pagesSystemic Lupus ErythematosusdaliaNo ratings yet
- Approach To Physical ExaminationDocument23 pagesApproach To Physical Examinationjustfree786No ratings yet
- Diploma in Medical and Health Science Case ClerkingDocument9 pagesDiploma in Medical and Health Science Case ClerkingWan AmeeramirulzamanNo ratings yet
- Veterinary Clinical DiagnosisDocument77 pagesVeterinary Clinical Diagnosismmohammed seidNo ratings yet
- Session 10 - Experimental Study DesignDocument33 pagesSession 10 - Experimental Study Designsaurabh chaturvediNo ratings yet
- Notes of GynecologyDocument104 pagesNotes of GynecologyJean Pierre Hitimana100% (1)
- 4 Medical ConsultationDocument34 pages4 Medical ConsultationSelin SakarNo ratings yet
- Case Presentation OsteomylitisDocument64 pagesCase Presentation OsteomylitisDemi Rose Bolivar100% (1)
- HISTORYDocument28 pagesHISTORYrxmskdkd33No ratings yet
- Practice Station Headache HXDocument7 pagesPractice Station Headache HXWenbin GuoNo ratings yet
- Introduction To Diagnostics: Hu Suping 1st Clinical College, Wuhan UniversityDocument68 pagesIntroduction To Diagnostics: Hu Suping 1st Clinical College, Wuhan Universityapi-19641337No ratings yet
- Surgery Long Cases Scripts N Q&ADocument118 pagesSurgery Long Cases Scripts N Q&Asofea zamriNo ratings yet
- 1a-History Taking in SurgeryDocument19 pages1a-History Taking in SurgeryMohammad Farouq Omar100% (1)
- Introduction To PhlebotomyDocument39 pagesIntroduction To PhlebotomyLyrics District100% (1)
- Anamnesis Status GeneralisDocument103 pagesAnamnesis Status GeneralisHusnanMujiburrahmanNo ratings yet
- Prev MedDocument51 pagesPrev MedJam JamaNo ratings yet
- Triage in Emergency Department: Triage Waiting Room Team LeaderDocument27 pagesTriage in Emergency Department: Triage Waiting Room Team LeaderJerry AbleNo ratings yet
- 2beginning The History Taking-1Document30 pages2beginning The History Taking-1Wizz Háķìm ĻêşòwNo ratings yet
- DR - Muse Medical History & Physical ExmnDocument27 pagesDR - Muse Medical History & Physical Exmnaxmedfare138No ratings yet
- AMC Clinicals Sample ExamDocument36 pagesAMC Clinicals Sample Examadrenaline_medico100% (2)
- A Case Study of "Meningitis": Mary Chiles College Gastambide St. Sampaloc ManilaDocument16 pagesA Case Study of "Meningitis": Mary Chiles College Gastambide St. Sampaloc ManilaJessa BorreNo ratings yet
- Ebook2024 6073Document52 pagesEbook2024 6073raymond.timmer111No ratings yet
- 1 - Case HistoryDocument47 pages1 - Case HistoryAishwarya S. NairNo ratings yet
- Prep 5012Document64 pagesPrep 5012EbcNo ratings yet
- Clinical Diag of ADRs IntroductionDocument27 pagesClinical Diag of ADRs IntroductionecaicedoNo ratings yet
- Emergency Care in NursingDocument32 pagesEmergency Care in NursingPauline Añes100% (1)
- Practice Station History Breathless 1Document8 pagesPractice Station History Breathless 1Wenbin GuoNo ratings yet
- Approach To The Surgical PatientDocument51 pagesApproach To The Surgical Patientsanjivdas100% (1)
- Basic Tips in Clinical SurgeryDocument92 pagesBasic Tips in Clinical SurgeryZion_MilgemNo ratings yet
- Phlebotomy BookDocument130 pagesPhlebotomy Bookamrutha tkNo ratings yet
- Communication SkillsDocument37 pagesCommunication Skillskarine ChanNo ratings yet
- OSCE Preparation TipsDocument18 pagesOSCE Preparation TipsMin Maw100% (1)
- Unit 8 HLTH AssmtDocument25 pagesUnit 8 HLTH Assmtsaranya amuNo ratings yet
- 1) Identification Data:: Guide For Taking History in PediatricsDocument5 pages1) Identification Data:: Guide For Taking History in PediatricsAhmed Mansor AlariqiNo ratings yet
- Head To Toe SurveyDocument4 pagesHead To Toe SurveyKURIMAONGNo ratings yet
- PCDDocument15 pagesPCDana100% (1)
- BlacksmithDocument2 pagesBlacksmithTahpehs PhiriNo ratings yet
- E WasteDocument2 pagesE WasteTahpehs PhiriNo ratings yet
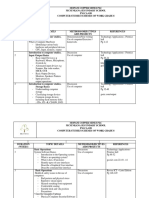
- 2023 Grade 8 Mid-Term Test (95 Copies) - ComputersDocument6 pages2023 Grade 8 Mid-Term Test (95 Copies) - ComputersTahpehs PhiriNo ratings yet
- 2023 Grade 10 EOT1 Computer StudiesDocument4 pages2023 Grade 10 EOT1 Computer StudiesTahpehs PhiriNo ratings yet
- Fatsch-MOCK 2022-P1Document10 pagesFatsch-MOCK 2022-P1Tahpehs PhiriNo ratings yet
- Final Mongu Conference Presentation 2023 - 123743Document35 pagesFinal Mongu Conference Presentation 2023 - 123743Tahpehs PhiriNo ratings yet
- GCE1Document4 pagesGCE1Tahpehs PhiriNo ratings yet
- 2022 Grade9 SBA #08 - PublisherDocument2 pages2022 Grade9 SBA #08 - PublisherTahpehs PhiriNo ratings yet
- 5 Feasibility ReportDocument37 pages5 Feasibility ReportTahpehs PhiriNo ratings yet
- Cog 13 LipidsDocument27 pagesCog 13 LipidsTahpehs PhiriNo ratings yet
- Table of Contents PDFDocument3 pagesTable of Contents PDFTahpehs PhiriNo ratings yet
- Cog 13 - VitaminsDocument36 pagesCog 13 - VitaminsTahpehs PhiriNo ratings yet
- Cog 13 - MineralsDocument26 pagesCog 13 - MineralsTahpehs PhiriNo ratings yet
- Computer Studies Grade 8-9: Read These Instructions FirstDocument8 pagesComputer Studies Grade 8-9: Read These Instructions FirstTahpehs PhiriNo ratings yet
- Cog 13 Disorders of Metabolism (Carbohydrates and Protein)Document8 pagesCog 13 Disorders of Metabolism (Carbohydrates and Protein)Tahpehs PhiriNo ratings yet
- Design and Technology G 5 7Document27 pagesDesign and Technology G 5 7Tahpehs PhiriNo ratings yet
- Social Studies Grade 1 7Document40 pagesSocial Studies Grade 1 7Tahpehs Phiri100% (1)
- Computer Studies SchemesDocument5 pagesComputer Studies SchemesTahpehs PhiriNo ratings yet
- Ministry of Education, Science, Vocational Training and Early Education Curriculum Development CentreDocument49 pagesMinistry of Education, Science, Vocational Training and Early Education Curriculum Development CentreTahpehs PhiriNo ratings yet
- Grade 12 End of Term 2 2020Document12 pagesGrade 12 End of Term 2 2020Tahpehs PhiriNo ratings yet
- G10-12 Computer Studies SchemesDocument12 pagesG10-12 Computer Studies SchemesTahpehs Phiri100% (1)
- Circular Number 4, Term 1, 2021Document4 pagesCircular Number 4, Term 1, 2021Tahpehs PhiriNo ratings yet
- Kitwe District: Ministry of General EducationDocument11 pagesKitwe District: Ministry of General EducationTahpehs PhiriNo ratings yet
- Computer Studies End of Term 3 TestDocument4 pagesComputer Studies End of Term 3 TestTahpehs Phiri100% (1)
- Eya MukwaiDocument1 pageEya MukwaiTahpehs PhiriNo ratings yet
- NAQ ToolDocument14 pagesNAQ ToolJulie MayNo ratings yet
- Assessment Three: Analysis of Legal and Professional Issues (2,200-Word Assignment, 50% of Available Mark)Document2 pagesAssessment Three: Analysis of Legal and Professional Issues (2,200-Word Assignment, 50% of Available Mark)Ayesha NaseerNo ratings yet
- Niaid Strategic Plan For COVID-19 Research: FY2020 - FY2024Document12 pagesNiaid Strategic Plan For COVID-19 Research: FY2020 - FY2024s pNo ratings yet
- Scientific Programme BookletDocument44 pagesScientific Programme BookletPreetam PatnalaNo ratings yet
- Drugs and The BodyDocument5 pagesDrugs and The BodyValones BeaNo ratings yet
- GASTRECTOMYDocument3 pagesGASTRECTOMYMaria Ydela MeradoresNo ratings yet
- It Feels Good To Laugh AnswersDocument3 pagesIt Feels Good To Laugh Answersapi-36173144314% (7)
- Brfo193 Radiotherapy Dose Fractionation Third-Edition PDFDocument137 pagesBrfo193 Radiotherapy Dose Fractionation Third-Edition PDFMed MedNo ratings yet
- Frequently Asked Questions On The Referral To Treatment (RTT) Data CollectionDocument24 pagesFrequently Asked Questions On The Referral To Treatment (RTT) Data Collectionraduben5403No ratings yet
- Surgery For Breast CancerDocument12 pagesSurgery For Breast Cancerpooja singhNo ratings yet
- Rubella Quantitative IgG - IMMULITE 2000 SystemsDocument40 pagesRubella Quantitative IgG - IMMULITE 2000 SystemsMaria Ruth Moreno VargasNo ratings yet
- Mcgraw-Hill Companies, IncDocument2 pagesMcgraw-Hill Companies, IncLu LubNaNo ratings yet
- Therapy of Digestive Disorders PDFDocument3 pagesTherapy of Digestive Disorders PDFRistikNo ratings yet
- UNIT - 10 Infection Control: MeasuresDocument27 pagesUNIT - 10 Infection Control: MeasuresReeycha ShresthaNo ratings yet
- IPD. 2. DR Theo - PPOKDocument96 pagesIPD. 2. DR Theo - PPOKTheopilus Obed LayNo ratings yet
- NCP EdemaDocument1 pageNCP EdemaR Hornilla ArcegaNo ratings yet
- Ncbi List of Books and Dental ArticlesDocument6 pagesNcbi List of Books and Dental ArticlesIulia Isacov0% (1)
- 10 Golden Rules in MedicationDocument2 pages10 Golden Rules in MedicationYha Nha Rhu100% (1)
- CardiomegalyDocument91 pagesCardiomegalyMariquita Buenafe100% (1)
- Enf Tiroidea y Embarazo Lancet 2018Document12 pagesEnf Tiroidea y Embarazo Lancet 2018Jair Alexander Quintero PanucoNo ratings yet
- Ketamine Psychedelic Psychotherapy: Focus On Its Pharmacology PHDocument59 pagesKetamine Psychedelic Psychotherapy: Focus On Its Pharmacology PHMartin Girard100% (1)
- Anesthesia-Assisted Vs Buprenorphine - or Clonidine-Assisted Heroin Detoxification and Naltrexone InductionDocument11 pagesAnesthesia-Assisted Vs Buprenorphine - or Clonidine-Assisted Heroin Detoxification and Naltrexone InductionAndy PurnomoNo ratings yet
- Week 1 - Day 2 - Tracheostomy-Care-and-SuctioningDocument3 pagesWeek 1 - Day 2 - Tracheostomy-Care-and-SuctioningPaola CruzNo ratings yet
- Novilyn C. Pataray BSN - Ii: Assessment Diagnosi S Pathophysiolog Y Planning Interevention Rationale EvaluationDocument1 pageNovilyn C. Pataray BSN - Ii: Assessment Diagnosi S Pathophysiolog Y Planning Interevention Rationale EvaluationCharina AubreyNo ratings yet
- Presentation Facilitated by Madam: Saima Mateen: Group Members: Shahzad Raza Saba KaleemDocument54 pagesPresentation Facilitated by Madam: Saima Mateen: Group Members: Shahzad Raza Saba KaleemParas MauriceNo ratings yet
- Eye Essentials Cataract Assessment Classification and Management PDFDocument245 pagesEye Essentials Cataract Assessment Classification and Management PDFihsansiregarNo ratings yet
- 2023 Updated ACVIM Consensus Statement On Leptospirosis in DogsDocument17 pages2023 Updated ACVIM Consensus Statement On Leptospirosis in DogsAkın SeverNo ratings yet
- Qsen Competencies 2Document4 pagesQsen Competencies 2api-2691700450% (1)
- What Is Anemia?: Anemia Blood Cells Hemoglobin Blood Cells Symptoms of Anemia FatigueDocument5 pagesWhat Is Anemia?: Anemia Blood Cells Hemoglobin Blood Cells Symptoms of Anemia FatigueLIPTANo ratings yet