Download as pptx, pdf, or txt
You might also like
- CholecystitisDocument34 pagesCholecystitisapi-26762768100% (1)
- Large Intestine HistologyDocument24 pagesLarge Intestine HistologyMudassar RoomiNo ratings yet
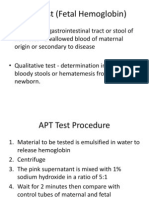
- APT Test (Fetal Hemoglobin)Document11 pagesAPT Test (Fetal Hemoglobin)Diovic TanNo ratings yet
- Disorders of Biliary SystemDocument29 pagesDisorders of Biliary SystemAjibola OlamideNo ratings yet
- Extrahepatic Biliary Tract Pathology - Cholidolithiasis, Cholidocholithiasis, Cholecystitis and CholangitisDocument60 pagesExtrahepatic Biliary Tract Pathology - Cholidolithiasis, Cholidocholithiasis, Cholecystitis and CholangitisDarien LiewNo ratings yet
- GB P LectureDocument32 pagesGB P LecturearthiNo ratings yet
- 8 - Disorders of The GallbladderDocument33 pages8 - Disorders of The Gallbladdersohaib salamehNo ratings yet
- Cholelithiasis: - Other Names: - Gallbladder Attack - Biliary Colic - Gallstone Attack - Bile Calculus - Biliary CalculusDocument101 pagesCholelithiasis: - Other Names: - Gallbladder Attack - Biliary Colic - Gallstone Attack - Bile Calculus - Biliary CalculusYvonne100% (1)
- Billiary Diseases Lecture 2023-2024Document10 pagesBilliary Diseases Lecture 2023-2024Taha MuhammedNo ratings yet
- Cholelithiasis GallstoneDocument22 pagesCholelithiasis GallstoneBheru LalNo ratings yet
- Gall Bladder Diseases 2023Document58 pagesGall Bladder Diseases 2023Ebuka AniNo ratings yet
- Case StudyDocument24 pagesCase StudyPatricia Marie BuenafeNo ratings yet
- Ntroduction: (1) (2) (3) Go ToDocument6 pagesNtroduction: (1) (2) (3) Go ToretnaNo ratings yet
- PRAVEENDocument33 pagesPRAVEENNaviNo ratings yet
- CHOLELITHIASISDocument12 pagesCHOLELITHIASISShenbagam MahalingamNo ratings yet
- Cholelithiasis: Group MembersDocument12 pagesCholelithiasis: Group MembersShiela GutierrezNo ratings yet
- Gallbladder Disease and Its Management-1Document39 pagesGallbladder Disease and Its Management-1adamu mohammadNo ratings yet
- ReportDocument12 pagesReportTomi Basallo BarriosNo ratings yet
- C P PPPP P PPPPPPDocument3 pagesC P PPPP P PPPPPPsildesireNo ratings yet
- 19 - Diseases of The Gallbladder and The Extrahepatic BiliaryDocument42 pages19 - Diseases of The Gallbladder and The Extrahepatic BiliarySuhayb CumarNo ratings yet
- GallstoneDocument6 pagesGallstoneMushfique HussainNo ratings yet
- Background: Biliary Colic Acute Cholecystitis Acute PancreatitisDocument14 pagesBackground: Biliary Colic Acute Cholecystitis Acute PancreatitisrhopmaeNo ratings yet
- I&IDocument7 pagesI&IJdee XNo ratings yet
- Case Stydy On CholithiasisDocument29 pagesCase Stydy On CholithiasisDaniel TalleyNo ratings yet
- Approach To Right Hypochondrium PainDocument34 pagesApproach To Right Hypochondrium PainkhansamrNo ratings yet
- Morphology of Gallbladder Tumors (Autosaved)Document25 pagesMorphology of Gallbladder Tumors (Autosaved)Rajeev NaikNo ratings yet
- Cholecystitis Litiasis EctomyDocument23 pagesCholecystitis Litiasis EctomyTimothy WilliamsNo ratings yet
- CholedocholithiasisDocument3 pagesCholedocholithiasisPao AcelajadoNo ratings yet
- Discussion of Disease (CholecystitisDocument3 pagesDiscussion of Disease (Cholecystitisjean paola nolascoNo ratings yet
- 13 CholecystitisDocument11 pages13 CholecystitisdorajuangaterNo ratings yet
- Pathogenesis of Diseases of The Gallbladder and Biliary TractDocument28 pagesPathogenesis of Diseases of The Gallbladder and Biliary TractMuhammad MakkiNo ratings yet
- 4.gall StoneDocument35 pages4.gall Stonejitendra magarNo ratings yet
- Gallstones CholelithiasisDocument35 pagesGallstones Cholelithiasiszerish0208No ratings yet
- 7 - The Biliary TractDocument48 pages7 - The Biliary TractKim RamosNo ratings yet
- Cholelithiasis & CholecystitisDocument2 pagesCholelithiasis & CholecystitisKate DNo ratings yet
- Common Name:: Gallstones Description: Gallstones Are A Collection of One or More Stones in The GallbladderDocument4 pagesCommon Name:: Gallstones Description: Gallstones Are A Collection of One or More Stones in The GallbladderKaren BumatayNo ratings yet
- CHOLECYSTITIS With CHOLECYSTOLITHIASISDocument33 pagesCHOLECYSTITIS With CHOLECYSTOLITHIASISSherry100% (3)
- Cholecystolithiasis: Characteristics and CompositionDocument7 pagesCholecystolithiasis: Characteristics and Compositionjesabel_caraigNo ratings yet
- CholelithiasisDocument6 pagesCholelithiasisLara GatbontonNo ratings yet
- Biliary Tract DiseasesDocument35 pagesBiliary Tract DiseasesSoumya Ranjan PandaNo ratings yet
- 1 Gallbladder Disease 2Document68 pages1 Gallbladder Disease 2salsabeelNo ratings yet
- Week 14 - BiliaryDocument102 pagesWeek 14 - BiliaryEditha LucasNo ratings yet
- CHOLELITIASISDocument31 pagesCHOLELITIASISRara ChanNo ratings yet
- CHolelitiasis, CholesistitisDocument44 pagesCHolelitiasis, CholesistitistrianaamaliaNo ratings yet
- Gall StonesDocument26 pagesGall StonesNia SinghNo ratings yet
- Cholelithiasis RLDocument29 pagesCholelithiasis RLPrincess Joanna Marie B DelfinoNo ratings yet
- Progesterone Has Been Shown To Decrease Gall-Bladder Motility, WhichDocument9 pagesProgesterone Has Been Shown To Decrease Gall-Bladder Motility, WhichFerreze AnnNo ratings yet
- Progesterone Has Been Shown To Decrease Gall-Bladder Motility, WhichDocument9 pagesProgesterone Has Been Shown To Decrease Gall-Bladder Motility, WhichFerreze AnnNo ratings yet
- CHOLELITHIASISSDocument29 pagesCHOLELITHIASISSAngelica Mercado SirotNo ratings yet
- Gallbladder 2Document8 pagesGallbladder 2hussain AltaherNo ratings yet
- Dave Jay S. Manriquez RN. Acute CholecystitisDocument11 pagesDave Jay S. Manriquez RN. Acute CholecystitisChilleMaeNo ratings yet
- CHOLELITHIASISDocument13 pagesCHOLELITHIASISMaria Nadeem, BS Home Economics Student, UoPNo ratings yet
- B. Synthesis of The DiseaseDocument5 pagesB. Synthesis of The DiseaseQaz ZaqNo ratings yet
- Cholecystitis Full With EditDocument43 pagesCholecystitis Full With Editmustafalotfy01No ratings yet
- Colilithiasis 2Document53 pagesColilithiasis 2Worku KifleNo ratings yet
- Gallstone DiseaseDocument104 pagesGallstone DiseaseTan DanNo ratings yet
- Hepatobiliary Tract and Pancreatic Pathology Assignment - PAYSONDocument22 pagesHepatobiliary Tract and Pancreatic Pathology Assignment - PAYSONRodrigo Joseph PaysonNo ratings yet
- The Diseases of GallbladderDocument27 pagesThe Diseases of GallbladderAroosha IbrahimNo ratings yet
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- A Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisFrom EverandA Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisRating: 3 out of 5 stars3/5 (1)
- The Slim Book of Health Pearls: Symptoms Never to IgnoreFrom EverandThe Slim Book of Health Pearls: Symptoms Never to IgnoreNo ratings yet
- Potential Use of Probiotics: Ekachai ChukeatiroteDocument8 pagesPotential Use of Probiotics: Ekachai ChukeatiroteDanu EffendiNo ratings yet
- Stoma Care BasicsDocument83 pagesStoma Care BasicsTeoh HsNo ratings yet
- Unit-6 PHYSIOLOGY OF GASTROINTESTINAL SYSTEMDocument43 pagesUnit-6 PHYSIOLOGY OF GASTROINTESTINAL SYSTEMAmrita RanaNo ratings yet
- 1st Quarter Summative Test No.2Document1 page1st Quarter Summative Test No.2Marilou Kimayong50% (2)
- Histology of GIT: Esophagus and StomachDocument39 pagesHistology of GIT: Esophagus and StomachZara HaiderNo ratings yet
- Generic Name:: Is Used To Dissolve (Cholesterol) Gallstones and PDocument9 pagesGeneric Name:: Is Used To Dissolve (Cholesterol) Gallstones and PZAY EMNo ratings yet
- Food Poisoning-Elim Gluten-Elim The Effects of Gluten (Lectins) Eliminate Cause of High HCLDocument10 pagesFood Poisoning-Elim Gluten-Elim The Effects of Gluten (Lectins) Eliminate Cause of High HCLNavin Ramroop100% (2)
- Acute Abdomen and PeritonitisDocument17 pagesAcute Abdomen and PeritonitisAgatha Billkiss IsmailNo ratings yet
- Colostomy IrrigationDocument2 pagesColostomy IrrigationMallory FernandezNo ratings yet
- Hirschsprung 'S Disease: Incidence and Classi FicationDocument6 pagesHirschsprung 'S Disease: Incidence and Classi FicationGhina Mauizha WulandariNo ratings yet
- The Use of Pyloric Exclusion For Treating Duodenal Trauma: Case SeriesDocument5 pagesThe Use of Pyloric Exclusion For Treating Duodenal Trauma: Case SeriesHanny RusliNo ratings yet
- Advanced Nutrition and Human Metabolism 7th Edition Gropper Test BankDocument36 pagesAdvanced Nutrition and Human Metabolism 7th Edition Gropper Test Bankimpoorfoveola.a0gvs4100% (45)
- Summative Test 4th - DigestiveDocument2 pagesSummative Test 4th - DigestiveMay Joy VitorioNo ratings yet
- c12 Digestive System Monog - Rum.YoungDocument4 pagesc12 Digestive System Monog - Rum.YoungAlexandra AlexandraNo ratings yet
- Digestion and Absorption 111Document6 pagesDigestion and Absorption 111Brijesh BalachandranNo ratings yet
- Ateneo de Zamboanga University College of Nursing NCM 112j RLEDocument3 pagesAteneo de Zamboanga University College of Nursing NCM 112j RLEsenyorakath0% (1)
- CT AbdoDocument2 pagesCT AbdoDR NIKNo ratings yet
- Human Digestive SystemDocument4 pagesHuman Digestive SystemmadamNo ratings yet
- 5 Poll - Z-05 (20 Ques.)Document2 pages5 Poll - Z-05 (20 Ques.)Mag GamingNo ratings yet
- Female RTOG Normal Pelvis Atlas PDFDocument129 pagesFemale RTOG Normal Pelvis Atlas PDFsusdoctor100% (1)
- RT 105 Midterm NotesDocument17 pagesRT 105 Midterm NotesLouiseNo ratings yet
- (2020) Pearls and Pitfalls of Interpretation in CT ColonographyDocument9 pages(2020) Pearls and Pitfalls of Interpretation in CT ColonographyChristian ToalongoNo ratings yet
- Sunarlim 2008Document10 pagesSunarlim 2008Gabriel BoggieNo ratings yet
- Small IntDocument59 pagesSmall IntCatalin SavinNo ratings yet
- Digistive Detailed Lesson PlanDocument5 pagesDigistive Detailed Lesson PlanMark Anthony Telan Pitogo100% (2)
- Liver Cirrhosis PDFDocument9 pagesLiver Cirrhosis PDFDennis CobbNo ratings yet
- Life Processes (Nutrition)Document4 pagesLife Processes (Nutrition)Rajender Kumar SharmaNo ratings yet
- Ezzat PaperDocument15 pagesEzzat PaperMohamedAbdelmonaemNo ratings yet