Download as pptx, pdf, or txt
You might also like
- Plab 1 Lectures Endo NotesDocument81 pagesPlab 1 Lectures Endo NotesmesutNo ratings yet
- MedSurg Notes - Cancer of The LiverDocument2 pagesMedSurg Notes - Cancer of The LiverMae CeaesarNo ratings yet
- Homeopathy First Aid RemediesDocument91 pagesHomeopathy First Aid Remedieskasradin4791% (22)
- Oralmed MCQDocument6 pagesOralmed MCQRavi Shankar Kolluru100% (5)
- Grimmer Arthur Hill. - The Homeopathic Treatment of CancerDocument4 pagesGrimmer Arthur Hill. - The Homeopathic Treatment of CancerElanghovan ArumugamNo ratings yet
- Parathyroid Gland and Other Endocrine GlandsDocument35 pagesParathyroid Gland and Other Endocrine GlandsDrRahma Ali HeissNo ratings yet
- Calcium Metabolism-Board Questions 2018: Azar Khosravi April 2018Document55 pagesCalcium Metabolism-Board Questions 2018: Azar Khosravi April 2018Abdullah SiddiqiNo ratings yet
- Parathyroid Adenoma: Chou Chien-Wen M.D. Endocrine & Metabolism Section Chi-Mei Medical Center 10 Jan 2003Document30 pagesParathyroid Adenoma: Chou Chien-Wen M.D. Endocrine & Metabolism Section Chi-Mei Medical Center 10 Jan 2003anand787No ratings yet
- Parathyroid Gland Diseases: Classification of Diseases of PTGDocument11 pagesParathyroid Gland Diseases: Classification of Diseases of PTGgashbin latifNo ratings yet
- 9 Anaesthesia For ProstatectomyDocument7 pages9 Anaesthesia For ProstatectomySilvie DinNo ratings yet
- Parathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022Document42 pagesParathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022juanrangoneNo ratings yet
- Parathyroid DiseaseDocument10 pagesParathyroid Diseasemohammedghassan53No ratings yet
- Endocrine TumorsDocument107 pagesEndocrine TumorsBinit BharatiNo ratings yet
- Dr. Putu Anda Tusta Adiputra, SP.B (K) OnkDocument37 pagesDr. Putu Anda Tusta Adiputra, SP.B (K) OnkNym Angga SantosaNo ratings yet
- Zeng 2019Document3 pagesZeng 2019Andrei MarianNo ratings yet
- Vitamin DDocument25 pagesVitamin DSyeda AlizaNo ratings yet
- Benign Prostatic Hyperplasia (BPH)Document8 pagesBenign Prostatic Hyperplasia (BPH)miftah ar rahmahNo ratings yet
- Hyperparathyroidism Mancini 100401060921 Phpapp02Document41 pagesHyperparathyroidism Mancini 100401060921 Phpapp02anand787No ratings yet
- HiperparatiroidDocument23 pagesHiperparatiroidrahmaNo ratings yet
- What Is The Diagnosis?Document2 pagesWhat Is The Diagnosis?Mel ObisNo ratings yet
- Parathyroid Disease Lecture SlidesDocument50 pagesParathyroid Disease Lecture SlidesMaxwell PalSingh100% (1)
- Hyper para Thyroid Is MDocument3 pagesHyper para Thyroid Is MAriefNo ratings yet
- Surgical Diseases of The Parathyroid GlandsDocument34 pagesSurgical Diseases of The Parathyroid Glandsanand787No ratings yet
- Para ThyroidDocument41 pagesPara ThyroidAdham YounesNo ratings yet
- IDK HiperparatiroidDocument23 pagesIDK HiperparatiroidWidya GladiantariNo ratings yet
- Pathology BinderDocument406 pagesPathology BinderFaisol KabirNo ratings yet
- HyperparathyroidismDocument41 pagesHyperparathyroidismShabeel PnNo ratings yet
- CA A Cancer J Clinicians - 2011 - Lewis - Oncologic Emergencies Pathophysiology Presentation Diagnosis and TreatmentDocument28 pagesCA A Cancer J Clinicians - 2011 - Lewis - Oncologic Emergencies Pathophysiology Presentation Diagnosis and TreatmentUtami DewiNo ratings yet
- Thyroiditis and Parathyroid GlandDocument29 pagesThyroiditis and Parathyroid GlandTheoder RobinsonNo ratings yet
- Paraneoplastic Hypercalcaemia As A Cause of Unexplained Renal Impairment in A Patient With Seminoma A Case ReportDocument5 pagesParaneoplastic Hypercalcaemia As A Cause of Unexplained Renal Impairment in A Patient With Seminoma A Case Reportkshwel.pNo ratings yet
- Hypercalcemia & MSCCDocument29 pagesHypercalcemia & MSCCSA NodeNo ratings yet
- HyperparathyroidismDocument15 pagesHyperparathyroidismMuhamad ZulfiqarNo ratings yet
- The Parathyroid GlandDocument66 pagesThe Parathyroid GlandMohammed GamalNo ratings yet
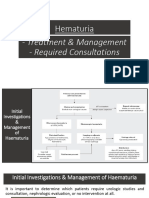
- Hematuria Treatment Management and Required ConsultationsDocument10 pagesHematuria Treatment Management and Required ConsultationsDiyana ZatyNo ratings yet
- Lec#49 Calcium DisordersDocument105 pagesLec#49 Calcium DisordersKhaldoun AlmomaniNo ratings yet
- Liver CA. SheDocument5 pagesLiver CA. SheSheryl OcampoNo ratings yet
- Hypercalcemia: Colorado ACP Meeting February 2017 David Tanaka MD FACPDocument33 pagesHypercalcemia: Colorado ACP Meeting February 2017 David Tanaka MD FACPRo KohnNo ratings yet
- Hypercalcaemia Guideline For Primary CareDocument5 pagesHypercalcaemia Guideline For Primary Caredesak indryNo ratings yet
- Diagnosis and Management of Parathyroid Disease: Nino Zaya, MD December 1, 2005Document43 pagesDiagnosis and Management of Parathyroid Disease: Nino Zaya, MD December 1, 2005taqadasabbasdrNo ratings yet
- Liver Cirrhosis and Its ComplicationsDocument34 pagesLiver Cirrhosis and Its ComplicationsEthel ChakotaNo ratings yet
- Hypercalcemia: Bibek Ghimire 3 Batch, PAHSDocument25 pagesHypercalcemia: Bibek Ghimire 3 Batch, PAHSBibek GhimireNo ratings yet
- Acute Pancreatitis in AdultsDocument107 pagesAcute Pancreatitis in AdultsBurhan MinervaNo ratings yet
- Superior Vena Cava Obstruction-Raised ICP-BleedingDocument31 pagesSuperior Vena Cava Obstruction-Raised ICP-BleedingSA NodeNo ratings yet
- Adrenal Disorders - RaasiDocument39 pagesAdrenal Disorders - RaasiArun kumarNo ratings yet
- Anestesia Transplat FigadoDocument7 pagesAnestesia Transplat FigadocaioaccorsiNo ratings yet
- Liver Cancer Pathophysiology: Predisposing FactorDocument3 pagesLiver Cancer Pathophysiology: Predisposing FactorTarantado100% (2)
- 0815 Skugor HyperAndHypocalcemiaDocument79 pages0815 Skugor HyperAndHypocalcemiaSirNorman BalinoNo ratings yet
- 2022-OXFORD-HANDBOOK-OF-ANAESTHESIA-Oxford-Press-5th-Edition ExportDocument4 pages2022-OXFORD-HANDBOOK-OF-ANAESTHESIA-Oxford-Press-5th-Edition ExportHany ElbarougyNo ratings yet
- LEC 3 Parathyroid Gland DisordersDocument39 pagesLEC 3 Parathyroid Gland Disordersalhusien.abd2000No ratings yet
- Disorders of The Parathyroid GlandsDocument30 pagesDisorders of The Parathyroid Glandsikram ullah khan100% (1)
- BPH (Benign Prostatic Hyperplasia)Document11 pagesBPH (Benign Prostatic Hyperplasia)AviZhafiraNo ratings yet
- Solitary Thyroid Nodule Done by Dr. Dana Al-Zarraq Supervised y Dr. Saleh HammadDocument50 pagesSolitary Thyroid Nodule Done by Dr. Dana Al-Zarraq Supervised y Dr. Saleh HammadMohammad BanisalmanNo ratings yet
- Parathyroid DisordersDocument44 pagesParathyroid DisordersBIAN ALKHAZMARI100% (1)
- HYPERTHYROIDISMDocument48 pagesHYPERTHYROIDISMManoj Ghimire100% (1)
- Hypoparathyroidism / Hypocalcemia: Abrar Alharbi, F1Document32 pagesHypoparathyroidism / Hypocalcemia: Abrar Alharbi, F1abrarNo ratings yet
- Principles of Preoperative and Operative SurgeryDocument71 pagesPrinciples of Preoperative and Operative SurgeryRajarshi KumarNo ratings yet
- Urology Nursing Presentation Emily MarsallDocument37 pagesUrology Nursing Presentation Emily MarsallHerdy Rizky SusetyoNo ratings yet
- Parathyroid DiseaseDocument29 pagesParathyroid DiseaseTara AzadNo ratings yet
- Primary HyperparathyroidismDocument16 pagesPrimary HyperparathyroidismHamza AhmedNo ratings yet
- 2 - Parathyroid GlandDocument21 pages2 - Parathyroid Glandtaha55860No ratings yet
- Urinary Bladder and Renal Cell CarcinomaDocument21 pagesUrinary Bladder and Renal Cell CarcinomaYazeed AsrawiNo ratings yet
- Labs & Imaging for Primary Eye Care: Optometry In Full ScopeFrom EverandLabs & Imaging for Primary Eye Care: Optometry In Full ScopeNo ratings yet
- Obstetrical HemorrhageDocument10 pagesObstetrical Hemorrhagemendato marcabanNo ratings yet
- Abnormal LaborDocument6 pagesAbnormal Labormendato marcabanNo ratings yet
- Ectopic PregnancyDocument7 pagesEctopic Pregnancymendato marcabanNo ratings yet
- AnemiaDocument9 pagesAnemiamendato marcabanNo ratings yet
- AbortionDocument9 pagesAbortionmendato marcabanNo ratings yet
- Abnormal Uterine BleedingDocument5 pagesAbnormal Uterine Bleedingmendato marcabanNo ratings yet
- 13 - Physiology of Penile Erection and Pa Tho Physiology of Erectile DysfunctionDocument6 pages13 - Physiology of Penile Erection and Pa Tho Physiology of Erectile DysfunctionJasen Liu100% (1)
- Bio Investigatory Project of Class 12Document34 pagesBio Investigatory Project of Class 12Aditya Kadapa75% (4)
- NCP For COLON Cancer PatientDocument4 pagesNCP For COLON Cancer PatientCarolina Tardecilla100% (1)
- Atlas of Endocrine Pathology - Erickson, Lori ADocument208 pagesAtlas of Endocrine Pathology - Erickson, Lori Aoyenen100% (1)
- Lung Examination: Abnormal Arcot J. Chandrasekhar, M.D.: StepsDocument6 pagesLung Examination: Abnormal Arcot J. Chandrasekhar, M.D.: StepsadjcdaughtNo ratings yet
- Profound Ai: For Digital Breast TomosynthesisDocument2 pagesProfound Ai: For Digital Breast TomosynthesisJuanGabrielVillamizarNo ratings yet
- Complications of Upper GI SDocument30 pagesComplications of Upper GI SNavin ChandarNo ratings yet
- 85 Linearny Urychlovac Clinac IxDocument12 pages85 Linearny Urychlovac Clinac IxTài NguyễnNo ratings yet
- Handbook 4th Ed 2014 PDFDocument241 pagesHandbook 4th Ed 2014 PDFStacy SmithNo ratings yet
- From The Words Listed Below, Choose The Ones Which Best Fit The Space, A, B, C or DDocument6 pagesFrom The Words Listed Below, Choose The Ones Which Best Fit The Space, A, B, C or DAndronache MihaiNo ratings yet
- WallstreetjournalDocument32 pagesWallstreetjournalMeherJazibAli0% (1)
- PPM May08 Kneebone LaserAcupunctureDocument4 pagesPPM May08 Kneebone LaserAcupuncturejoseNo ratings yet
- The Endocrine System Work SheetDocument3 pagesThe Endocrine System Work SheetLucia SpaninksNo ratings yet
- Material Safety Data Sheet: Emergency Phone Number: 1-866-272-4378Document1 pageMaterial Safety Data Sheet: Emergency Phone Number: 1-866-272-4378So MayeNo ratings yet
- HEADACHE in NeurologyDocument80 pagesHEADACHE in NeurologyIhsanAkbarNo ratings yet
- Bahasa Inggris 3Document9 pagesBahasa Inggris 3vinavzenirNo ratings yet
- Essential Notes in Internal Medicine - 1st EdDocument163 pagesEssential Notes in Internal Medicine - 1st EdEhsanullah HikmatNo ratings yet
- Kuliah Tiroid (Prof - Dr. Harsinen S, SP - pd-kEMD)Document138 pagesKuliah Tiroid (Prof - Dr. Harsinen S, SP - pd-kEMD)aliimranzNo ratings yet
- SWDDocument58 pagesSWDakheel ahammedNo ratings yet
- Diseases of Oral CavityDocument60 pagesDiseases of Oral Cavityfredrick damian80% (5)
- Case Study 102Document6 pagesCase Study 102Cheska Lopez100% (1)
- Recurrent Respiratory Papillomatosis: FaringDocument49 pagesRecurrent Respiratory Papillomatosis: FaringIchsanJuliansyahNo ratings yet
- Takayasu Arteritis Challenges in DiagnosisDocument9 pagesTakayasu Arteritis Challenges in DiagnosisYesenia HuertaNo ratings yet
- Bishop Score of PregnancyDocument13 pagesBishop Score of PregnancydrvijeypsgNo ratings yet
- Exam 4 Practice QuestionsDocument11 pagesExam 4 Practice Questionslaramyy100% (1)
- PPCMDocument7 pagesPPCMRizki FitriantoNo ratings yet
- Tonation - Spectro-Chrome MetryDocument5 pagesTonation - Spectro-Chrome MetryitounosNo ratings yet