Download as pptx, pdf, or txt
You might also like
- Greenspan's 9th Edition (2011) PDFDocument897 pagesGreenspan's 9th Edition (2011) PDFVea Angeles50% (2)
- Chapter 21: Nursing Care of A Family Experiencing A Sudden Pregnancy ComplicationDocument9 pagesChapter 21: Nursing Care of A Family Experiencing A Sudden Pregnancy ComplicationAlyssaGrandeMontimor100% (1)
- 15 - Multiple PregnancyDocument21 pages15 - Multiple PregnancyBharat Thapa100% (5)
- STG and Nemlt 2021Document618 pagesSTG and Nemlt 2021Emmanuel Ngimba100% (2)
- Multiple Pregnancy LectureDocument33 pagesMultiple Pregnancy Lecturefarid_nchep100% (1)
- Miscarriage & Early Pregnancy LossDocument38 pagesMiscarriage & Early Pregnancy LossLuqman OsmanNo ratings yet
- Multiple Pregnancy: Prof Uma SinghDocument53 pagesMultiple Pregnancy: Prof Uma Singhpok yeahNo ratings yet
- Multiple PregnancyDocument17 pagesMultiple PregnancyagnesochanyaodehNo ratings yet
- 2 Multiple - Pregnancy - Lecture 2018Document48 pages2 Multiple - Pregnancy - Lecture 2018abrhamNo ratings yet
- Multiple Pregnancy: Prof Uma SinghDocument53 pagesMultiple Pregnancy: Prof Uma Singhgeng gengNo ratings yet
- Twin TDocument30 pagesTwin TmaezuNo ratings yet
- Understanding Multiple Pregnancy: Maternal & Fetal ComplicationsDocument69 pagesUnderstanding Multiple Pregnancy: Maternal & Fetal Complications966342No ratings yet
- Multiple Gestation: Dr. Hotma Partogi Pasaribu Spog Sub Division of Fetomaternal Medical Faculty - Usu Rsham - RSPM MedanDocument47 pagesMultiple Gestation: Dr. Hotma Partogi Pasaribu Spog Sub Division of Fetomaternal Medical Faculty - Usu Rsham - RSPM MedanSyarifah KhamsiawanNo ratings yet
- Multiple Pregnancy: Nirav Hitesh Kumar ValandDocument28 pagesMultiple Pregnancy: Nirav Hitesh Kumar ValandNirav SharmaNo ratings yet
- 4th Year Multiple PregnancyDocument57 pages4th Year Multiple PregnancyKingsley Calex100% (2)
- Multiple Pregnancy: Kevin AndrewDocument36 pagesMultiple Pregnancy: Kevin AndrewintanpurnNo ratings yet
- Multiple PregnancyDocument55 pagesMultiple PregnancyNathaniel YeriNo ratings yet
- علاااءDocument21 pagesعلاااءalaazeez2000No ratings yet
- Multiple Pregnancy: Fahad ZakwanDocument60 pagesMultiple Pregnancy: Fahad Zakwanhaisuresh100% (1)
- Multiple Pregnancy LectureDocument29 pagesMultiple Pregnancy LectureEuniceNo ratings yet
- Multifetal Pregnancy: Dr. Hani MahdiDocument59 pagesMultifetal Pregnancy: Dr. Hani MahdiArwa QishtaNo ratings yet
- Multiple Pregnancy: Dr. A. Farid Abdullah, SP - OG, M.KesDocument33 pagesMultiple Pregnancy: Dr. A. Farid Abdullah, SP - OG, M.KesAndi Farid A100% (1)
- Multiple PXDocument46 pagesMultiple PXBetelhem EjiguNo ratings yet
- Multiple PregnancyDocument23 pagesMultiple Pregnancy19 KomalNo ratings yet
- Multiple PregnancyDocument15 pagesMultiple PregnancyM.S.H TubeNo ratings yet
- Multiple Pregnancy HatimDocument22 pagesMultiple Pregnancy HatimHatim AbdellateifNo ratings yet
- Multiple PregnancyDocument32 pagesMultiple PregnancyRebbeccah NafulaNo ratings yet
- Multiple Pregnancy: EpidemiologyDocument6 pagesMultiple Pregnancy: EpidemiologyMelissa Aina Mohd YusofNo ratings yet
- Multifetal Pregnancy: Amr Nadim, MDDocument36 pagesMultifetal Pregnancy: Amr Nadim, MDsharenNo ratings yet
- Twin Pregnancy, Materi DM Rsud SdaDocument28 pagesTwin Pregnancy, Materi DM Rsud SdaHilda AmirahNo ratings yet
- Bab IDocument10 pagesBab Iyona sarastikaNo ratings yet
- Multifetal PregnancyDocument68 pagesMultifetal PregnancyHoque Mohammed Newaz ShorifulNo ratings yet
- Successful Pregnancy Outcome in A Case of Bi-Cornuate Uterus With Boh With Secondary Infertility and GDM - A Very Rare Case Report - Medisun AcademyDocument4 pagesSuccessful Pregnancy Outcome in A Case of Bi-Cornuate Uterus With Boh With Secondary Infertility and GDM - A Very Rare Case Report - Medisun AcademyGautom Kumar PaulNo ratings yet
- Book ReportDocument69 pagesBook ReportBarangay MotibotNo ratings yet
- By: Letta Sari Lintang O&G DepartmentDocument28 pagesBy: Letta Sari Lintang O&G Departmentイアン リムホト ザナガNo ratings yet
- Multiple Pregnancies Predisposing FactorsDocument11 pagesMultiple Pregnancies Predisposing FactorseunicesomtinNo ratings yet
- 11-Ectopic PregnancyDocument35 pages11-Ectopic PregnancyDawit g/kidanNo ratings yet
- Muhammad Redzwan Bin Abdullah: 081303583 Batch 25 Group E2Document66 pagesMuhammad Redzwan Bin Abdullah: 081303583 Batch 25 Group E2Suyajna JoshiNo ratings yet
- Multiple Pregnancy GuidelineDocument12 pagesMultiple Pregnancy GuidelineAlia BangeshNo ratings yet
- Multiple Fetal Pregnancy: Riza SufriadiDocument20 pagesMultiple Fetal Pregnancy: Riza SufriadiRizur SufisonNo ratings yet
- Multiple PregnancyDocument52 pagesMultiple Pregnancyazida90100% (4)
- Multiple PregnancesssssDocument29 pagesMultiple PregnancesssssNajjemba ShanitahNo ratings yet
- In ComDocument3 pagesIn ComDeen Deen L OrdonaNo ratings yet
- IUFD Repro21Document31 pagesIUFD Repro21DhianNo ratings yet
- Ectopic Pregnancy - PowerpointDocument60 pagesEctopic Pregnancy - PowerpointAndrada Doţa100% (1)
- Multiple PregnanciesDocument36 pagesMultiple PregnanciesBasudev ch100% (1)
- Malpresntation, Malposition and Breech Presentation 2022 BayisaDocument45 pagesMalpresntation, Malposition and Breech Presentation 2022 BayisaHile ShaNo ratings yet
- Obg AbortionDocument62 pagesObg Abortionkashyap priyankaNo ratings yet
- Twins: SupervisorDocument10 pagesTwins: Supervisorكيرلس مجدىNo ratings yet
- MK Multiple Gestation (OBGY)Document16 pagesMK Multiple Gestation (OBGY)Moses Jr KazevuNo ratings yet
- Twin PregnancyDocument73 pagesTwin Pregnancykrishna mandalNo ratings yet
- Obs Hist 2Document27 pagesObs Hist 2Muneera ONo ratings yet
- Multiple Pregnancy2Document76 pagesMultiple Pregnancy2Murali KrishvanNo ratings yet
- Multiple GestationDocument24 pagesMultiple GestationNura BamaiyiNo ratings yet
- MCN - Individual Activity 3Document23 pagesMCN - Individual Activity 3AngelicaJaneA.SuanNo ratings yet
- Pa Mantas An NG Lungsod NG MarikinaDocument5 pagesPa Mantas An NG Lungsod NG MarikinaMeryl AlcantaraNo ratings yet
- Student Unit 2 Topic 2.5 Jan 2018 TAYLORDocument42 pagesStudent Unit 2 Topic 2.5 Jan 2018 TAYLORKrista KloseNo ratings yet
- 10 - Multiple GestationDocument11 pages10 - Multiple GestationShatha QudahNo ratings yet
- Twins M RoosDocument26 pagesTwins M RoosMichelle RoosNo ratings yet
- Discordant GrowthDocument20 pagesDiscordant GrowthBarangay MotibotNo ratings yet
- 3&4 MiscarraigeDocument90 pages3&4 MiscarraigeAbdullah GadNo ratings yet
- On Autumn's Wing, A Story of Birth Trauma, Brain Injury and Miracles.From EverandOn Autumn's Wing, A Story of Birth Trauma, Brain Injury and Miracles.No ratings yet
- Cancar of Vagina 2021Document9 pagesCancar of Vagina 2021NoahNo ratings yet
- Post MaturityDocument45 pagesPost MaturityNoahNo ratings yet
- Shoulder DystociaDocument18 pagesShoulder DystociaNoahNo ratings yet
- Caesarean SectionDocument3 pagesCaesarean SectionNoahNo ratings yet
- Imbong vs. OchoaDocument8 pagesImbong vs. OchoaFrederick EboñaNo ratings yet
- Menstrual Cycle Biology ProjectDocument4 pagesMenstrual Cycle Biology ProjectaddyNo ratings yet
- Knowledge and Practice of Pelvic Floor Muscle Exercises Among Pregnant Women in Enugu Metropolis, NigeriaDocument7 pagesKnowledge and Practice of Pelvic Floor Muscle Exercises Among Pregnant Women in Enugu Metropolis, NigeriaQORI KARUNIA WANTINo ratings yet
- Multiple ChoiceDocument6 pagesMultiple ChoiceBenmar L. OrterasNo ratings yet
- Lyphochek Immunoassay Plus Control Levels 1, 2 and 3Document11 pagesLyphochek Immunoassay Plus Control Levels 1, 2 and 3Enrique DuarteNo ratings yet
- ObstetricsDocument216 pagesObstetricsሌናፍ ኡሉምNo ratings yet
- Mammalogy, Part I: Origin of MammalsDocument7 pagesMammalogy, Part I: Origin of MammalsashleylaramieNo ratings yet
- C1 Ob-Gyn-2020Document33 pagesC1 Ob-Gyn-2020yabsera mulatuNo ratings yet
- Reproduction (Multiple Choice) 2 QPDocument22 pagesReproduction (Multiple Choice) 2 QPLow Wai LeongNo ratings yet
- Tugas KKPMT Pregnancy, Childbirth and The PuerperiumDocument3 pagesTugas KKPMT Pregnancy, Childbirth and The PuerperiumDyah CitraNo ratings yet
- 陳v Endometrial Cancer 2Document48 pages陳v Endometrial Cancer 201范芷紜No ratings yet
- Congenital Adrenal HyperplasiaDocument10 pagesCongenital Adrenal HyperplasiaJemmy Wijaya100% (1)
- Animal Physiology Nutrition - 2020 - Schmitt - Calcium and Phosphorus Metabolism in Peripartal DogsDocument8 pagesAnimal Physiology Nutrition - 2020 - Schmitt - Calcium and Phosphorus Metabolism in Peripartal Dogsศักดิ์สุวีร์ เจริญวงศ์ศักดิ์No ratings yet
- Anti TPODocument4 pagesAnti TPOhossein mosavi jalaliNo ratings yet
- Theories and Principle of EthicsDocument4 pagesTheories and Principle of Ethicsmichael angelo leonardoNo ratings yet
- Impact of Menstruation On Academic Performance Among Female Nursing StudentsDocument4 pagesImpact of Menstruation On Academic Performance Among Female Nursing StudentsEditor IJTSRDNo ratings yet
- Dr. Bassem W. Yani, MD Diploma of Urology, FEBU, FCS, Cairo, EGYPT Consultant Urologist Uth Lusaka ZambiaDocument43 pagesDr. Bassem W. Yani, MD Diploma of Urology, FEBU, FCS, Cairo, EGYPT Consultant Urologist Uth Lusaka ZambiaMohammed AadeelNo ratings yet
- ANTENATAL ASSESSMENT Form 3Document4 pagesANTENATAL ASSESSMENT Form 3Kaku ManishaNo ratings yet
- Nutritional AnemiaDocument53 pagesNutritional AnemiaANUREET KAURNo ratings yet
- Brandy: What Really Happened To MeDocument90 pagesBrandy: What Really Happened To MerenaNo ratings yet
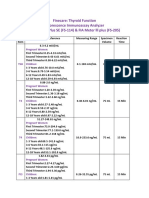
- Thyroid FunctionDocument2 pagesThyroid FunctionSm Bikash Kumar MohonNo ratings yet
- Lebo Mashile - These Hips Have Carried BouldersDocument6 pagesLebo Mashile - These Hips Have Carried BouldersNasim khanNo ratings yet
- Ethical and Legal Issues in Midwifery and ObstetricsDocument9 pagesEthical and Legal Issues in Midwifery and ObstetricsMahenur100% (2)
- Short Practice Test 02 - Test Paper - Lakshya NEET 2025Document6 pagesShort Practice Test 02 - Test Paper - Lakshya NEET 2025rshreyash136No ratings yet
- MetricefDocument2 pagesMetricefPrakashNallappanNo ratings yet
- Genital ProlapseDocument3 pagesGenital Prolapsecraniophage95No ratings yet
- Early Pregnancy Anomaly ScanDocument80 pagesEarly Pregnancy Anomaly ScanCezara Si Bogdan Muresan100% (3)