Download as pptx, pdf, or txt
You might also like
- Service Manual M5521cdn-cdw-M5526cdnDocument700 pagesService Manual M5521cdn-cdw-M5526cdnabm50318187% (31)
- GE2777 PentaPals The Urbanization in Davao City and Its Impacts To Climate ChangeDocument7 pagesGE2777 PentaPals The Urbanization in Davao City and Its Impacts To Climate Changewendell tatoy1No ratings yet
- Components of Polishing and Cleaning AgentsDocument55 pagesComponents of Polishing and Cleaning AgentsJohn J Cadavid100% (6)
- Cardiac ChamberDocument45 pagesCardiac ChamberguzmansayrieNo ratings yet
- Principles of HemodynamicDocument48 pagesPrinciples of HemodynamicdevdsantoshNo ratings yet
- Blood Flow Mechanics (Medicalstudyzone - Com)Document31 pagesBlood Flow Mechanics (Medicalstudyzone - Com)Lordoc DoctorsaabNo ratings yet
- Cardiovascular NotesDocument23 pagesCardiovascular NotesEmily DongNo ratings yet
- Blood, Blood Vessels & CirculationDocument59 pagesBlood, Blood Vessels & CirculationNermeinKhattabNo ratings yet
- 3A HemodynamicsDocument42 pages3A Hemodynamicspmm23d177No ratings yet
- Hemodinamika Dan Tekanan Darah: Denny AgustiningsihDocument38 pagesHemodinamika Dan Tekanan Darah: Denny AgustiningsihSofia Nur RahmaniaNo ratings yet
- Dr. S. Wulandari, M.SCDocument38 pagesDr. S. Wulandari, M.SCzuma_zedNo ratings yet
- Arteries and VeinsDocument47 pagesArteries and VeinsArianna MohiuddinNo ratings yet
- Blood CirculationDocument28 pagesBlood CirculationIngrid RaineNo ratings yet
- Cardiovascular Physiology & Urine Formation: Biology 25 A. SantiagoDocument39 pagesCardiovascular Physiology & Urine Formation: Biology 25 A. Santiagoapi-3826751No ratings yet
- 8 Venous ReturnDocument19 pages8 Venous ReturnDmNo ratings yet
- Cardiovascular Lecture 1 - 2023 2024Document31 pagesCardiovascular Lecture 1 - 2023 2024inegbenosegideonNo ratings yet
- Determinants of Blood Pressure NewDocument31 pagesDeterminants of Blood Pressure NewRiyaNo ratings yet
- Topic 6 Circulation FullDocument41 pagesTopic 6 Circulation Fullazankha1990No ratings yet
- Hemodynamics: DR Axelle Saverettiar Mbbs Physiology Department SSR Medical CollegeDocument31 pagesHemodynamics: DR Axelle Saverettiar Mbbs Physiology Department SSR Medical CollegeÑäd ÉèmNo ratings yet
- Cardio. Vascular System (The Circulatory System) : Blood 2' HeartDocument12 pagesCardio. Vascular System (The Circulatory System) : Blood 2' Heartعزوز الراويNo ratings yet
- Final Integrated Labcon Batch 2010Document32 pagesFinal Integrated Labcon Batch 2010api-3700579No ratings yet
- CVS & HypertensionDocument92 pagesCVS & HypertensionNimesh ModiNo ratings yet
- Cardiovascular Physiology DR AnjilaDocument167 pagesCardiovascular Physiology DR AnjilaJacob MasikaNo ratings yet
- Hemodynamics 0Document9 pagesHemodynamics 0Ehtiram HuseynovNo ratings yet
- 1-ch 20 - CardiovascularDocument142 pages1-ch 20 - Cardiovascularlouise navorNo ratings yet
- Physio-DES-6 (Cardiac)Document56 pagesPhysio-DES-6 (Cardiac)Joseph Kim100% (1)
- Reviewer in ANAPIYA Finale Part 1Document9 pagesReviewer in ANAPIYA Finale Part 1Llyana paula SuyuNo ratings yet
- 3 CVSDocument10 pages3 CVSzabdullahstud1No ratings yet
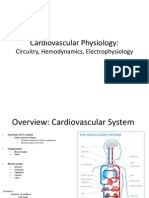
- Cardiovascular Physiology:: Circuitry, Hemodynamics, ElectrophysiologyDocument27 pagesCardiovascular Physiology:: Circuitry, Hemodynamics, Electrophysiologyrsmoney3No ratings yet
- Chapter 14 - Overview of The CirculationDocument26 pagesChapter 14 - Overview of The Circulationmuna sNo ratings yet
- The Circulation: Dr. Adelina VladDocument72 pagesThe Circulation: Dr. Adelina VladalexcargosaNo ratings yet
- Biophysics Lecture 4 HemodynamicsDocument18 pagesBiophysics Lecture 4 HemodynamicsmalyaaNo ratings yet
- Introduction To Cardiovascular PhysiologyDocument29 pagesIntroduction To Cardiovascular PhysiologyMariuca MaryNo ratings yet
- Circulation. Lec On HemodynamicsDocument30 pagesCirculation. Lec On HemodynamicsMudassar RoomiNo ratings yet
- HEARTDocument8 pagesHEARTSJane FeriaNo ratings yet
- Chapter 20bDocument6 pagesChapter 20baexillisNo ratings yet
- The Heart PDFDocument13 pagesThe Heart PDFMary Ann SacramentoNo ratings yet
- Physics in Medicine: PH3708 DR R.J. StewartDocument27 pagesPhysics in Medicine: PH3708 DR R.J. StewartAndi ZaidanNo ratings yet
- Animal Transport Revision NotesDocument19 pagesAnimal Transport Revision NotesNada Abu ShweimehNo ratings yet
- CV-5 PH MicrocircDocument34 pagesCV-5 PH Microcircaya najemNo ratings yet
- Hemodynamics: Ncmb418 - Critical Care Nursing Rle Midterm LectureDocument7 pagesHemodynamics: Ncmb418 - Critical Care Nursing Rle Midterm LectureKyle Saberon100% (1)
- Swan Ganz FinalDocument36 pagesSwan Ganz FinalDanial HassanNo ratings yet
- Lecture 6 Cardiovascular: Vascular System - The HemodynamicsDocument70 pagesLecture 6 Cardiovascular: Vascular System - The HemodynamicsAndreea ŞtefănescuNo ratings yet
- 5.4 Heart f2f-s1b2-23Document36 pages5.4 Heart f2f-s1b2-23shlokNo ratings yet
- DR Lakshmi MMM 2009 FINALDocument33 pagesDR Lakshmi MMM 2009 FINALsubha shreeNo ratings yet
- Cardiovascular Physiology Raw FileDocument47 pagesCardiovascular Physiology Raw FileRishabh KashyapNo ratings yet
- Cardiac Physiology PDFDocument17 pagesCardiac Physiology PDFAli Aborges Jr.No ratings yet
- HemodynamicsDocument19 pagesHemodynamicsMariam ShekhaniNo ratings yet
- 12 Circulatory Systems IIDocument39 pages12 Circulatory Systems IIImansyah PutraNo ratings yet
- The Heart: Basis of Life .?Document94 pagesThe Heart: Basis of Life .?Diksha AgrawalNo ratings yet
- Physiology DES: Biruk A. (Balemaye@sgu - Edu) & Sami Ahmed. (Sahmed10@sgu - Edu)Document56 pagesPhysiology DES: Biruk A. (Balemaye@sgu - Edu) & Sami Ahmed. (Sahmed10@sgu - Edu)Joseph KimNo ratings yet
- Vascular Resistant: Saja Al-Marshad Senior RC Student Dammam UniversityDocument15 pagesVascular Resistant: Saja Al-Marshad Senior RC Student Dammam Universitysaja100% (1)
- Review of The Anatomy of The HeartDocument9 pagesReview of The Anatomy of The HeartJhasseryne Orias SanchezNo ratings yet
- (Dragged) 1Document36 pages(Dragged) 1Alexandra Ramos MNo ratings yet
- NCMB 418 Hemodynamics Week 7Document34 pagesNCMB 418 Hemodynamics Week 7Jennifer Ambrosio100% (1)
- Heartstructurenotes PDFDocument3 pagesHeartstructurenotes PDFcyprianNo ratings yet
- ELEC4810 Notes-7 PDFDocument61 pagesELEC4810 Notes-7 PDFKwan ChanNo ratings yet
- Cardiorespiratory System: Structure and FunctionsDocument19 pagesCardiorespiratory System: Structure and FunctionsKasam ANo ratings yet
- Physiology Notes V 06Document6 pagesPhysiology Notes V 06miraNo ratings yet
- Cardiovascular SystemDocument35 pagesCardiovascular Systemdelacruzchristinejoie.kldNo ratings yet
- 05 Cardiovascular System Physiology Part2Document37 pages05 Cardiovascular System Physiology Part2Kaye Alyssa EnriquezNo ratings yet
- 2 Hemodynamic Theory On SICPDocument62 pages2 Hemodynamic Theory On SICPantoni_gamundi3942No ratings yet
- 08 Neurons Cell Networks Edit NoQuesDocument62 pages08 Neurons Cell Networks Edit NoQuesugjdk djfgNo ratings yet
- 15 Blood Flow Control Edit NOquesDocument34 pages15 Blood Flow Control Edit NOquesugjdk djfgNo ratings yet
- 13 Motor Control and Reflexes Edit NOquesDocument22 pages13 Motor Control and Reflexes Edit NOquesugjdk djfgNo ratings yet
- 06 Homeostasis Edit NoQuesDocument13 pages06 Homeostasis Edit NoQuesugjdk djfgNo ratings yet
- 05 - Just 5 - 7 RMPDocument14 pages05 - Just 5 - 7 RMPugjdk djfgNo ratings yet
- Wondfo Fia Finecare Plus Se Fs 114Document2 pagesWondfo Fia Finecare Plus Se Fs 114Toto FollyNo ratings yet
- 01.24 MA App Form Version 20.0Document3 pages01.24 MA App Form Version 20.0Jen EugenioNo ratings yet
- Market Study of Fine Flavour Cocoa - Revised VersionDocument109 pagesMarket Study of Fine Flavour Cocoa - Revised VersionJose Ramon Ruiz LedezmaNo ratings yet
- Reacción de GombergDocument32 pagesReacción de GombergDiegoRiveraNo ratings yet
- Ca 2 Cardiovascular-Oxygenation Assignment Part 1Document8 pagesCa 2 Cardiovascular-Oxygenation Assignment Part 1Joseph AbangNo ratings yet
- Vent Silencer Data SheetDocument1 pageVent Silencer Data SheetRamazan YaşarNo ratings yet
- Fabm 21Document6 pagesFabm 21kristelNo ratings yet
- Summer CaMP Participants Application FormDocument1 pageSummer CaMP Participants Application Formjoshua gaspadoNo ratings yet
- Supervision Procedure: Oml100 (Fso Unity)Document8 pagesSupervision Procedure: Oml100 (Fso Unity)Ezemeh Nigeria100% (1)
- 3a - Oil Displacement MechanismDocument14 pages3a - Oil Displacement MechanismrizkiNo ratings yet
- UV-Curing Coatings Coatings: For Textiles: WithDocument10 pagesUV-Curing Coatings Coatings: For Textiles: WithIsmail BayraktarNo ratings yet
- Step by Step Lihation of The Internal Iliac ArteryDocument6 pagesStep by Step Lihation of The Internal Iliac ArteryAkbar PurnadiputraNo ratings yet
- TeaTime - July-August 202Document68 pagesTeaTime - July-August 202Anonymous LpUQ1pVyjONo ratings yet
- Practice Teaching On Administer A Test, Score, Grade VS MarkDocument13 pagesPractice Teaching On Administer A Test, Score, Grade VS MarkAjay KolageNo ratings yet
- Clinical Oral Implants Res - 2022 - Lamperti - Cemented Versus Screw Retained Zirconia Based Single Implant RestorationsDocument9 pagesClinical Oral Implants Res - 2022 - Lamperti - Cemented Versus Screw Retained Zirconia Based Single Implant RestorationsIsaac MoNo ratings yet
- Lightweight Particles in Aggregate: Standard Test Method ForDocument3 pagesLightweight Particles in Aggregate: Standard Test Method Formanuel davilaNo ratings yet
- The Eastern Countries Trail MapDocument32 pagesThe Eastern Countries Trail MapSergio Carrisi100% (1)
- 10.4324 9781003216261 PreviewpdfDocument40 pages10.4324 9781003216261 PreviewpdfmeitaNo ratings yet
- TIB-723-GB-0613 AP 2way Valves With Electric Actuator English PDFDocument67 pagesTIB-723-GB-0613 AP 2way Valves With Electric Actuator English PDFnguyenvanhai19031981No ratings yet
- Evaluation of Stability DataDocument21 pagesEvaluation of Stability DataMartin Celestino100% (2)
- Comprehention - EngyDocument12 pagesComprehention - Engyascom asNo ratings yet
- Research Chpter 1 With Chpter 2Document3 pagesResearch Chpter 1 With Chpter 2Aron JaroNo ratings yet
- Dass42 PDFDocument2 pagesDass42 PDFJohaima HaronNo ratings yet
- Practice: Deep Vein ThrombosisDocument6 pagesPractice: Deep Vein ThrombosisAri Setiyawan NugrahaNo ratings yet
- Short Notes Form 4 Biology Chapter 1 4 PDFDocument6 pagesShort Notes Form 4 Biology Chapter 1 4 PDFTanUeiHorngNo ratings yet
- EREC-43 Load ScheduleDocument61 pagesEREC-43 Load SchedulePartha SundarNo ratings yet