Download as pptx, pdf, or txt
You might also like
- Basic of Thorax Imaging - 10 September 2013 - by Robby HermawanDocument126 pagesBasic of Thorax Imaging - 10 September 2013 - by Robby HermawanenriNo ratings yet
- The Radiology Handbook: A Pocket Guide to Medical ImagingFrom EverandThe Radiology Handbook: A Pocket Guide to Medical ImagingRating: 3.5 out of 5 stars3.5/5 (8)
- Gap Assessment Reporting FormatDocument117 pagesGap Assessment Reporting FormatRonit BoraNo ratings yet
- Lec2 X-Rays and FluorosDocument39 pagesLec2 X-Rays and Fluorossana mumtazNo ratings yet
- Gambaran Radiologis Pada Kegawatan Paru: Farah Fatma WatiDocument42 pagesGambaran Radiologis Pada Kegawatan Paru: Farah Fatma WatisabariaNo ratings yet
- The Chest RadiographDocument9 pagesThe Chest RadiographandialisaNo ratings yet
- Dr. Dicky SP.P Materi Gawat Darurat ParuDocument41 pagesDr. Dicky SP.P Materi Gawat Darurat ParuYuni SaviraNo ratings yet
- Chest X-Ray Fundamentals: Dr. Emad EfatDocument241 pagesChest X-Ray Fundamentals: Dr. Emad EfatRutvik Shah100% (1)
- Basic Chest X-Ray Interpretation (5minutes Talk) : DR - Alemayehu (ECCM R1)Document35 pagesBasic Chest X-Ray Interpretation (5minutes Talk) : DR - Alemayehu (ECCM R1)Alex beharuNo ratings yet
- INTRODUCCION Libro RadiologiaDocument9 pagesINTRODUCCION Libro RadiologiaDavid ReyesNo ratings yet
- Neonatal Chest X-Ray-2019Document11 pagesNeonatal Chest X-Ray-2019madhu rathoreNo ratings yet
- Adult Chest X-RayDocument60 pagesAdult Chest X-RayAnil DasNo ratings yet
- Emergency Radiology: The BasicsDocument68 pagesEmergency Radiology: The BasicsArya Vandy Eka PradanaNo ratings yet
- Imaging Modalities For Lung DiseasesDocument14 pagesImaging Modalities For Lung DiseasesYnaffit Alteza Untal100% (1)
- 2 1 Diseases of The Respiratory System Radiological Pathology DRDocument43 pages2 1 Diseases of The Respiratory System Radiological Pathology DRNatnael GetahunNo ratings yet
- Chest X - Ray: Physiotherapy in Cardio-Respiratory Disorders & Intensive Care ManagementDocument25 pagesChest X - Ray: Physiotherapy in Cardio-Respiratory Disorders & Intensive Care ManagementSravan SNo ratings yet
- Chest XrayDocument104 pagesChest Xrayanindia wardhaniNo ratings yet
- Chest Radiography For InternsDocument42 pagesChest Radiography For InternsRose ValeNo ratings yet
- Basic Chest Imaging and Heart FailureDocument57 pagesBasic Chest Imaging and Heart FailureKiaa auliaNo ratings yet
- Neonatal Chest X Ray 2019Document11 pagesNeonatal Chest X Ray 2019Ahmad ApriansahNo ratings yet
- Chest Xray BasicsDocument47 pagesChest Xray BasicsPartha GanesanNo ratings yet
- Basic CXR Mod AdamDocument59 pagesBasic CXR Mod AdamCheska TumulakNo ratings yet
- Chest X-Ray GuideDocument26 pagesChest X-Ray GuideRizky Ayu WirdaningsiNo ratings yet
- Radiology Lecture 4th Year 2022 Part 2Document44 pagesRadiology Lecture 4th Year 2022 Part 2Abubakar JallohNo ratings yet
- XrayDocument15 pagesXraymiguel mendezNo ratings yet
- ChestDocument15 pagesChestmiguel mendezNo ratings yet
- Manuscript For Chest XrayDocument5 pagesManuscript For Chest XrayCharles Vergel Sabaldan MarceraNo ratings yet
- Postgraduate Course 3 Radiological-Pathological Correlation of Tumoural and Non-Tumoural Pathology: An Interdisciplinary ApproachDocument31 pagesPostgraduate Course 3 Radiological-Pathological Correlation of Tumoural and Non-Tumoural Pathology: An Interdisciplinary ApproachBulborea MihaelaNo ratings yet
- Thoracic Imaging Radiographic BasicsDocument130 pagesThoracic Imaging Radiographic BasicsIsak ShatikaNo ratings yet
- Basic of Thorax ImagingDocument105 pagesBasic of Thorax ImagingIlham Matoha100% (1)
- Chest Introduction: Technical AdequacyDocument28 pagesChest Introduction: Technical AdequacyAnshul JainNo ratings yet
- Lecture 09,10 - Foundations of USG PDFDocument78 pagesLecture 09,10 - Foundations of USG PDFWaqas SaeedNo ratings yet
- ABC ChestDocument4 pagesABC ChestSintounNo ratings yet
- Lecture 1 - Imaging Modalities SlidesDocument65 pagesLecture 1 - Imaging Modalities Slidesubcradadmin100% (1)
- The Normal Lung, Anatomy, Physiology, RadioDocument54 pagesThe Normal Lung, Anatomy, Physiology, Radioerrol.williamson19No ratings yet
- Use of Ultrasound in The ICU BestPracResearAnest 2009Document13 pagesUse of Ultrasound in The ICU BestPracResearAnest 2009RicardoNo ratings yet
- 2 POCUS in Emergency FAST IVC LUNGresidents December 2022Document92 pages2 POCUS in Emergency FAST IVC LUNGresidents December 2022dr mohd abdul basithNo ratings yet
- Chest X-Ray & EcgDocument148 pagesChest X-Ray & EcgAsaliwe Borah100% (1)
- Basic of Thorax Imaging - 10 September 2013 - by Robby HermawanDocument126 pagesBasic of Thorax Imaging - 10 September 2013 - by Robby HermawannuradilahyasminNo ratings yet
- What Is Ultrasound?Document15 pagesWhat Is Ultrasound?Al-Mukashfi TahaNo ratings yet
- Chest X Ray SessionDocument110 pagesChest X Ray SessionzakiyaNo ratings yet
- Basics of Chest X-RayDocument44 pagesBasics of Chest X-RayvmamikonNo ratings yet
- Fundamentals of Chest RadiologyDocument119 pagesFundamentals of Chest RadiologyAlexandra DîrțuNo ratings yet
- Ultrasound CourseDocument65 pagesUltrasound CourseRichard KenkelNo ratings yet
- Medical Imaging Overview-Dr FidensDocument92 pagesMedical Imaging Overview-Dr FidensMugisha M. BienfaitNo ratings yet
- XRAYDocument77 pagesXRAYRashmi PandeyNo ratings yet
- MS Lec Reporting MidtermDocument41 pagesMS Lec Reporting MidtermShekinah GeriosaNo ratings yet
- Introduction To Ultrasound in Emergency Department: A&E Medical MeetingDocument24 pagesIntroduction To Ultrasound in Emergency Department: A&E Medical MeetingdhanudgNo ratings yet
- Ctscan-Adoptation and UsesDocument54 pagesCtscan-Adoptation and UsesSourabh KalolikarNo ratings yet
- Emergency Radiology With QuizDocument115 pagesEmergency Radiology With QuizJustisia PadmiyatiNo ratings yet
- Diagnostic Approach To TraumaDocument72 pagesDiagnostic Approach To TraumaJoher MendezNo ratings yet
- Presentacion US Encefalica RSNADocument52 pagesPresentacion US Encefalica RSNAJessicaNo ratings yet
- Imagenology: Medical Imaging Modalities Method For Interpretation of ImagesDocument61 pagesImagenology: Medical Imaging Modalities Method For Interpretation of ImagesSamadrita CNo ratings yet
- Chest X Ray - zp162335Document48 pagesChest X Ray - zp162335Kushmakar VarshneyNo ratings yet
- Basics of Chest X-RayDocument44 pagesBasics of Chest X-RayMelissa Aina Mohd YusofNo ratings yet
- Notes For Neuroimaging: Introduction To Medical Imaging and Common Neurodevelopmental AnomaliesDocument5 pagesNotes For Neuroimaging: Introduction To Medical Imaging and Common Neurodevelopmental AnomaliesHanako Sasaki AranillaNo ratings yet
- Juanico, Clareen Mae (Assignment)Document3 pagesJuanico, Clareen Mae (Assignment)Clareen JuanicoNo ratings yet
- Chest X - Ray InterpretationDocument147 pagesChest X - Ray InterpretationFcsieka FcseikaNo ratings yet
- Chest X Ray (Autosaved)Document194 pagesChest X Ray (Autosaved)772footballNo ratings yet
- Noninvasive Imaging of Congenital Heart Disease Before and After Surgical ReconstructionFrom EverandNoninvasive Imaging of Congenital Heart Disease Before and After Surgical ReconstructionNo ratings yet
- Chest X-ray Interpretation for Radiographers, Nurses and Allied Health ProfessionalsFrom EverandChest X-ray Interpretation for Radiographers, Nurses and Allied Health ProfessionalsNo ratings yet
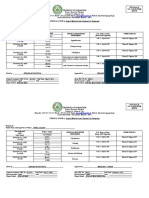
- Date Performed Patient's Name Procedure Performed OR Nurse On Duty Supervised byDocument1 pageDate Performed Patient's Name Procedure Performed OR Nurse On Duty Supervised byjames pasionNo ratings yet
- ESPEN Practical Guideline Home Enteral NutritionDocument21 pagesESPEN Practical Guideline Home Enteral NutritionJeanCarlosNo ratings yet
- Periodontal Instruments 1Document50 pagesPeriodontal Instruments 1Fahriansyah Maulana SudirmanNo ratings yet
- Anesthesiology Clinics Volume 32 Issue 2 2014 (Doi 10.1016/j.anclin.2014.02.022) Anderson, Jennifer Klock, P. Allan PDFDocument17 pagesAnesthesiology Clinics Volume 32 Issue 2 2014 (Doi 10.1016/j.anclin.2014.02.022) Anderson, Jennifer Klock, P. Allan PDFaprinaNo ratings yet
- Perfusion Concept MapDocument1 pagePerfusion Concept Mapapi-639782898No ratings yet
- Imm Mcqs Solved (Umer Hayat and DR RaliDocument129 pagesImm Mcqs Solved (Umer Hayat and DR RaliJaved GabaNo ratings yet
- Resume of Od1206Document3 pagesResume of Od1206api-23436180No ratings yet
- JOralMaxillofacRadiol 2021 9 2 40 325043Document6 pagesJOralMaxillofacRadiol 2021 9 2 40 325043divya reddyNo ratings yet
- 6.infratemporal FossaDocument63 pages6.infratemporal Fossaqns8mhb7wyNo ratings yet
- Stress-Induced Cardiomyopathy: A Case of Takotsubo Cardiomyopathy and Review of LiteratureDocument7 pagesStress-Induced Cardiomyopathy: A Case of Takotsubo Cardiomyopathy and Review of LiteratureInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Acute Abdomen &peritonitisDocument63 pagesAcute Abdomen &peritonitisSamar Ahmad100% (1)
- Incision and DrainageDocument35 pagesIncision and DrainageVilma Delos Reyes100% (1)
- VoucherDocument4 pagesVoucherAnne B.No ratings yet
- Uterine Anomalies - OB-GYNDocument4 pagesUterine Anomalies - OB-GYNNatnael GetahunNo ratings yet
- 2019 v13n4 008Document5 pages2019 v13n4 008Hanh LeNo ratings yet
- CPR PresentationDocument33 pagesCPR Presentationathar.shahNo ratings yet
- 27th CAFT Surgery GADVASU PDFDocument2 pages27th CAFT Surgery GADVASU PDFsumanth gowdaNo ratings yet
- HemorrhageDocument13 pagesHemorrhagekins.bhojaniNo ratings yet
- Self Study Handout - Medical Terminology - 2022Document14 pagesSelf Study Handout - Medical Terminology - 2022rhn 5b1coolNo ratings yet
- University of Pangasinan Phinma Education Network Arellano ST., Dagupan CityDocument5 pagesUniversity of Pangasinan Phinma Education Network Arellano ST., Dagupan CitymyannbeguasNo ratings yet
- Interventional Pain Management Low Back PainDocument13 pagesInterventional Pain Management Low Back PainAshok Jadon100% (4)
- Osteoid Osteoma: Multimodality Imaging With Focus On Hybrid ImagingDocument18 pagesOsteoid Osteoma: Multimodality Imaging With Focus On Hybrid ImagingCătălin Paul CernișencuNo ratings yet
- Risk Factors in Implant DentistryDocument168 pagesRisk Factors in Implant DentistryNeil Schembri100% (1)
- Bipolar Lead Manual - 2017Document43 pagesBipolar Lead Manual - 2017Srijan DeyNo ratings yet
- Get Through MRCOG Part 1 2nd EditionDocument142 pagesGet Through MRCOG Part 1 2nd Editionmustafa benmuhsen50% (2)
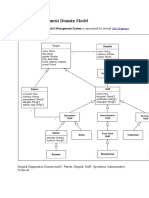
- Hospital Management Domain ModelDocument4 pagesHospital Management Domain Modelvinod kapateNo ratings yet
- Ultimate Examination Bundle - 221111 - 203054Document717 pagesUltimate Examination Bundle - 221111 - 203054musayyab muz100% (1)
- Manual of General Local Examination (Medicine - Paediatrics - Surgery) V 12.0Document50 pagesManual of General Local Examination (Medicine - Paediatrics - Surgery) V 12.0Epun B. DissanayakeNo ratings yet
- Gross Veterinary Anatomy: Binarao, Maria Beatriz L. DVM Ii-A 1Document3 pagesGross Veterinary Anatomy: Binarao, Maria Beatriz L. DVM Ii-A 1BeatrizNo ratings yet