Download as ppt, pdf, or txt
You might also like
- Definitions and Pillars For Safemother HoodDocument39 pagesDefinitions and Pillars For Safemother HoodDengAwut100% (5)
- Drawing HandsDocument11 pagesDrawing Handsjefffm80% (5)
- HANSEN P4 Service ManualDocument44 pagesHANSEN P4 Service ManualNinad Monpara67% (3)
- Care of Pregnant MotherDocument14 pagesCare of Pregnant MotherBhumika RathiNo ratings yet
- Intl J Gynecology Obste - 2023 - Killeen - Using FIGO Nutrition Checklist Counselling in Pregnancy A Review To SupportDocument12 pagesIntl J Gynecology Obste - 2023 - Killeen - Using FIGO Nutrition Checklist Counselling in Pregnancy A Review To SupportJuan Carlos CachonNo ratings yet
- Research PaperDocument20 pagesResearch Paperapi-545538199No ratings yet
- Research ReportDocument19 pagesResearch Reportapi-545001894No ratings yet
- What Is Prenatal Care and Why Is It ImportantDocument2 pagesWhat Is Prenatal Care and Why Is It Importantapi-395468231No ratings yet
- Jurnal RCT PrekonsepsiDocument11 pagesJurnal RCT PrekonsepsiDyah FiharjatinNo ratings yet
- School of Health and Allied Health Sciences Nursing DepartmentDocument4 pagesSchool of Health and Allied Health Sciences Nursing DepartmentJeane Louise PalmeroNo ratings yet
- Chapter 8 - Continuation of Maternal and Child Care: Lawrence Ryan A. Daug, RN, MPM CHN 1 - InstructorDocument49 pagesChapter 8 - Continuation of Maternal and Child Care: Lawrence Ryan A. Daug, RN, MPM CHN 1 - InstructorLawrence Ryan DaugNo ratings yet
- Anaesthesia - 2020 - Mitchell - Guideline On Anaesthesia and Sedation in Breastfeeding Women 2020Document12 pagesAnaesthesia - 2020 - Mitchell - Guideline On Anaesthesia and Sedation in Breastfeeding Women 2020ANGELICANo ratings yet
- Claudio Et Al HE Vol 3Document17 pagesClaudio Et Al HE Vol 3Elizalde HusbandNo ratings yet
- Guideline On Anaesthesia and Sedation in Breastfeeding Women 2020 Guideline From The Association of AnaesthetistsDocument12 pagesGuideline On Anaesthesia and Sedation in Breastfeeding Women 2020 Guideline From The Association of Anaesthetistsantonio123valenciaNo ratings yet
- SDL ActivitiesDocument11 pagesSDL Activitiesella retizaNo ratings yet
- Rough Draft For Capstone To Turn in Actual OneDocument14 pagesRough Draft For Capstone To Turn in Actual Oneapi-282022477No ratings yet
- Normal Diagnostic and Laboratory Findings/ Nutritional Health of Pregnant WomenDocument8 pagesNormal Diagnostic and Laboratory Findings/ Nutritional Health of Pregnant WomenArianna Jasmine MabungaNo ratings yet
- Final Draft For CapstoneDocument15 pagesFinal Draft For Capstoneapi-282022477No ratings yet
- Pre-Pregnancy Care (Webinar 25.5.2022)Document27 pagesPre-Pregnancy Care (Webinar 25.5.2022)SHELLY NOVITA SARI 1904053No ratings yet
- Notes On Maternal and Child Health NursingDocument3 pagesNotes On Maternal and Child Health NursingErika Bea PaculanangNo ratings yet
- Pre-Conceptional Counselling and Pre-Conceptional Care2Document61 pagesPre-Conceptional Counselling and Pre-Conceptional Care2divyamathew100% (1)
- Nutrition During LactationDocument5 pagesNutrition During LactationAyesha Snbcan008No ratings yet
- Promotion of Folate For The Prevention of Neural Tube Defects: Who Benefits?Document10 pagesPromotion of Folate For The Prevention of Neural Tube Defects: Who Benefits?Kandykane05No ratings yet
- FFT Policy Environment For Folic Acid InterventionsDocument16 pagesFFT Policy Environment For Folic Acid Interventionsbelete fentaNo ratings yet
- A Framework For Maternal and Child Health Nursing Care NCM 107Document3 pagesA Framework For Maternal and Child Health Nursing Care NCM 107Kyle VargasNo ratings yet
- IYCF Book Final 30-01-2018Document96 pagesIYCF Book Final 30-01-2018Hafeez SaleemiNo ratings yet
- Chapter II Edited JeffDocument20 pagesChapter II Edited JeffRoderick AgbuyaNo ratings yet
- Boado, Melody A. - NUPC108 - Assignment #1 (Finals)Document3 pagesBoado, Melody A. - NUPC108 - Assignment #1 (Finals)Melody BoadoNo ratings yet
- Frameworks MCHNDocument33 pagesFrameworks MCHNJerald FernandezNo ratings yet
- Assess Theknowledge & Practice of Pregnant and Lactating Women Related To Nutrition DeficiencyDocument16 pagesAssess Theknowledge & Practice of Pregnant and Lactating Women Related To Nutrition DeficiencyZohrahLiaqatNo ratings yet
- Maternal Health - Group 3Document30 pagesMaternal Health - Group 3Maryam AhmariNo ratings yet
- Folic Acid Deficiency PaperDocument5 pagesFolic Acid Deficiency Paperapi-401073891No ratings yet
- About The Conference: Benefits of Attending PCOS Conference 2020Document8 pagesAbout The Conference: Benefits of Attending PCOS Conference 2020Roxana FrincuNo ratings yet
- Assessment of Knowledge of Antenatal Mothers Regarding Selected Health Problems of Complicated Pregnancy-A Cross Sectional StudyDocument7 pagesAssessment of Knowledge of Antenatal Mothers Regarding Selected Health Problems of Complicated Pregnancy-A Cross Sectional StudyAjay DNo ratings yet
- Breastfeeding Is Priceless: There Is No Substitute For Human MilkDocument4 pagesBreastfeeding Is Priceless: There Is No Substitute For Human MilkmeetNo ratings yet
- Epidemiological Aspects of Maternaland Child HealthDocument42 pagesEpidemiological Aspects of Maternaland Child HealthSusmita SenNo ratings yet
- NDOH - PMTCT Apr 2008Document43 pagesNDOH - PMTCT Apr 2008fosuahlucy685No ratings yet
- Dos and Donts in PregnancyDocument9 pagesDos and Donts in PregnancyNadia UnitassiaNo ratings yet
- Northern University Assignment DemoDocument5 pagesNorthern University Assignment Demoasiansadia6No ratings yet
- BPH313Family and Reproductive Health Group 9 Presentation, SID 027-491Document17 pagesBPH313Family and Reproductive Health Group 9 Presentation, SID 027-491duku mosesNo ratings yet
- Breastfeeding Benefits HandoutDocument4 pagesBreastfeeding Benefits Handoutapi-313912304No ratings yet
- Breastfeeding PolicyDocument66 pagesBreastfeeding PolicyFrancisca MarcellaNo ratings yet
- Materi MandiriDocument6 pagesMateri Mandirip17311191006 RANINDYA DWI NOVIYANTINo ratings yet
- Breastfeeding and The Use of Human Milk 2005Document13 pagesBreastfeeding and The Use of Human Milk 2005Juan Pablo Anabalón SaavedraNo ratings yet
- Final PaperDocument25 pagesFinal Paperapi-453846317No ratings yet
- Sociology WHODocument3 pagesSociology WHO22518043drishtikhannaNo ratings yet
- PBL AllDocument14 pagesPBL Allxd7xopNo ratings yet
- History of Present IllnessDocument30 pagesHistory of Present IllnessTrixia Joy R NachorNo ratings yet
- Preconception Care ofDocument11 pagesPreconception Care ofsipen poltekkesbdgNo ratings yet
- Public Health Program Family HealthDocument183 pagesPublic Health Program Family HealthPrince Jhessie L. Abella100% (1)
- Public Health Program Family HealthDocument183 pagesPublic Health Program Family HealthPrince Jhessie L. AbellaNo ratings yet
- Hauwa'u - Chap-1-5Document51 pagesHauwa'u - Chap-1-5Usman Ahmad TijjaniNo ratings yet
- Module 2 - Maternal Health and NutritionDocument30 pagesModule 2 - Maternal Health and Nutritionkristal gail basitaoNo ratings yet
- Frequency of Malnutrition Among Children Under 2 Years and Its Relationship With Inadequate Breast Feeding PracticeDocument3 pagesFrequency of Malnutrition Among Children Under 2 Years and Its Relationship With Inadequate Breast Feeding PracticeAndhika SatriyaNo ratings yet
- Mother: I. Defintion/DescriptionDocument28 pagesMother: I. Defintion/Descriptionfaye kimNo ratings yet
- RESEARCH093016Document28 pagesRESEARCH093016Satra Sabbuh100% (1)
- Preconceptional and Prenatal CareDocument130 pagesPreconceptional and Prenatal CareAJAY MANDALNo ratings yet
- Magnitude of Maternal and Child Health ProblemsDocument21 pagesMagnitude of Maternal and Child Health ProblemsSusmita SenNo ratings yet
- Jurnal PDFDocument5 pagesJurnal PDFWaica PratiwiNo ratings yet
- INTRAPARTUMDocument59 pagesINTRAPARTUMastraia celesteNo ratings yet
- Hydrogen System ValidationDocument4 pagesHydrogen System Validationanita shindeNo ratings yet
- Cell Structure and Organisation NotesDocument27 pagesCell Structure and Organisation NotesGift Blessed NgoveNo ratings yet
- Factsheet The Later Stages of DementiaDocument20 pagesFactsheet The Later Stages of DementiaMspamNo ratings yet
- Transformer Winding Resistance MeterDocument15 pagesTransformer Winding Resistance MeterSyed Haider FaizanNo ratings yet
- Environmental DeterminismDocument7 pagesEnvironmental DeterminismSafdar HussainNo ratings yet
- Dobie Clay Fills in RSS PIT-XIV HATTI ID - 2011Document11 pagesDobie Clay Fills in RSS PIT-XIV HATTI ID - 2011Satriansyah EllenyudhaNo ratings yet
- Manufacturing Operations Checklist (Readiness Review For Ppap/Run@Rate)Document5 pagesManufacturing Operations Checklist (Readiness Review For Ppap/Run@Rate)khmorteza100% (1)
- Hypertension As A Health Deficit Criteria Computation Actual Score JustificationDocument8 pagesHypertension As A Health Deficit Criteria Computation Actual Score JustificationEunika Castro GarcesNo ratings yet
- Steel Dynamics' New Continuous Coil Coating Line For Steel StripDocument12 pagesSteel Dynamics' New Continuous Coil Coating Line For Steel StripJJNo ratings yet
- Case StudyDocument3 pagesCase Study-No ratings yet
- Tillamook Creamery IceCream Menu 07.01.21Document1 pageTillamook Creamery IceCream Menu 07.01.21Samantha AndersonNo ratings yet
- Workshop Block: Section B B'Document1 pageWorkshop Block: Section B B'Aditya KapoorNo ratings yet
- Audio Compression Using Daubechie WaveletDocument4 pagesAudio Compression Using Daubechie WaveletIOSRjournalNo ratings yet
- Receiver Mounted Motorcycle Carrier: Set Up and Operating InstructionsDocument8 pagesReceiver Mounted Motorcycle Carrier: Set Up and Operating InstructionsVeljko KercevicNo ratings yet
- Asignacion Ingles II Unidad I para EnviarDocument2 pagesAsignacion Ingles II Unidad I para EnviarMariaRamirezNo ratings yet
- Fosroc Dekguard Primer TDSDocument1 pageFosroc Dekguard Primer TDSRyaz AhamedNo ratings yet
- List of Nouns That Start With ADocument5 pagesList of Nouns That Start With Ajnk987No ratings yet
- Physics Problem Set S y 2020 21Document3 pagesPhysics Problem Set S y 2020 21GeeklyGamer 02No ratings yet
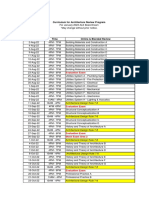
- Ale Jan 2023 - ScheduleDocument6 pagesAle Jan 2023 - ScheduleBenjie LatrizNo ratings yet
- Heat Transfer Operation Winter 2019 Question PaperDocument4 pagesHeat Transfer Operation Winter 2019 Question PaperMitesh ThakurNo ratings yet
- Complete Block DesignsDocument80 pagesComplete Block DesignsTaddese GashawNo ratings yet
- User Manual: Wireless N 300 ADSL2+ Modem RouterDocument70 pagesUser Manual: Wireless N 300 ADSL2+ Modem RouterMaamar DeryisheNo ratings yet
- ER420 - MS of G.I Pipe Crossing - r0Document12 pagesER420 - MS of G.I Pipe Crossing - r0Wr ArNo ratings yet
- Kama Da 1989Document9 pagesKama Da 1989kleopanNo ratings yet
- CA 2 Remedials Paper AY 2022-2023 - Math G4Document4 pagesCA 2 Remedials Paper AY 2022-2023 - Math G4Ceria Kue SoesNo ratings yet
- MFC-151 Manual enDocument11 pagesMFC-151 Manual enathanasiosNo ratings yet
- BSN 2-D - Rle Group 7Document10 pagesBSN 2-D - Rle Group 7Kyla VillafrancaNo ratings yet